
INTRODUCTION
Team handball athletes are considered unilateral, executing 100% of their throws with one arm. Although strength and conditioning targets the entire body, the sport-specific demands of handball often lead to muscle strength imbalance and structural adaptations.1 Unfortunately, acute and overuse injuries are both frequently reported in team handball2 and handball players are at high risk of developing shoulder injuries.3–6 The term “thrower’s shoulder” describes the adaptations in range of motion resulting from the repetitive high demands of throwing.7,8 The term “throwers paradox” refers to the balance between mobility and stability in the dominant shoulder. Increased shoulder mobility (external shoulder rotation) can create larger cocking during overhead throwing and, thereby, a longer trajectory for conducting force to the ball with the possibility of greater ball velocity.9 However, the range of motion must remain balanced to maintain the integrity of the shoulder’s dynamic and static structures.10
Structural adaptations are common within overhead athletes.11 Previous studies have categorized the risk factors for shoulder injuries in handball, focusing primarily on physical anatomical variations.12,13 Glenohumeral (GH) internal and external range of motion14,15 and internal and external shoulder strength1,16,17 have been identified as risk factors in overhead athletes. Abnormalities in previously mentioned risk factors are believed to increase the risk of shoulder pain, particularly when combined with an acute increase in training load of more than 20%.18 However, reduced GH internal rotation ROM combined with an increased external shoulder rotation ROM is a known risk factor for handball players.19–21 Structural adaptation, such as decreased internal shoulder rotation (i.e., glenohumeral internal rotation deficit, GIRD) and increased external rotation (i.e., external rotation gain), have been observed in the dominant shoulders of handball players.22 Previous research suggests that GIRD is a common phenomenon among throwing athletes, but these adaptations are permanent, and athletes can dynamically adapt to sport-specific movements.10,11,22,23
Handball athletes also often show an imbalance in strength between the external and internal shoulder rotators of the dominant arm.24 Although shoulder strength imbalance is suggested as a risk factor, the evidence is conflicting.25 Previous research has estimated that an isometric strength ratio of 0.70 ± 0.15 is common among adolescent elite handball players with shoulder injury symptoms.26
However, to the best of the authors’ knowledge, no previous study has included top elite handball players with a history of shoulder pain. While previous research has investigated rotational shoulder strength and range of motion in handball athletes, none have compared these factors among handball players who play handball at a top elite level who have current or previous shoulder pain.2,13,18,21
Therefore, this study aimed to compare the external and internal shoulder rotation range of motion and isometric strength among elite male and female handball players with current shoulder pain, previous shoulder pain, and no shoulder pain. It was hypothesized that men would exhibit greater shoulder strength than women, and the no-pain group would show greater IR and ER strength compared to the pain groups.17 Additionally, the authors anticipated that no differences would exist in external/internal shoulder range of motion across sex.6 but expected variations in the range of motion among players with current, previous, and no shoulder pain.21
MATERIALS AND METHODS
Study design and participants
Elite handball players, playing in the highest Romanian and Dutch leagues, and the top two leagues in Denmark and Norway were recruited. All players volunteered for the project after providing written and oral consent. All participants had to actively participate in the offensive and defensive parts of the game during both training and matches. Players were excluded from the study if they were recovering from a musculoskeletal injury anywhere in the body that had excluded them from participation in the prior six weeks. Furthermore, players with present or previous shoulder pain that was associated with a traumatic event or shoulder surgery were excluded.
All participants were fully informed about the protocol before participating in this study, and informed consent was obtained prior to all testing in accordance with the regulations of the Norwegian Center for Research Data and the principles of the Declaration of Helsinki. Ethical approval was obtained from the Norwegian ethics committee REK Midt in September 2019 (ref number. 7189).
Participants who consented to participate completed a medical questionnaire regarding shoulder pain, pain history, injury history, training, and match exposure. Based on their answers, the participants were divided into three groups: playing handball 1) with shoulder pain, 2) with previous shoulder pain, and 3) with no shoulder pain (Table 1). The presence of shoulder pain was established by the validated Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire.27 Furthermore, a supplementary oral interview was performed by a physical therapist to determine whether the pain registered in the pain and previous pain groups had a non-traumatic occurrence.
For the participants in the pain group, the shoulder pain had developed over time and was present for at least four weeks. Participants with previous shoulder pain were obliged to report no current pain and when they last had shoulder pain (start and stop of previous shoulder pain), and participants in the no-pain group had never experienced shoulder pain.
Test procedure
All tests were examined and administered by the same physical therapist who had 10 years of experience in physical testing in team handball and physical therapy. Before starting the test protocol, the participant received an oral introduction to each test procedure. Before the clinical tests were performed, anthropometrics were measured.
Range of motion
Passive glenohumeral range of motion was measured in the dominant shoulder using a digital goniometer (EasyAngle; Meloq AB; EU). Each measurement was performed two times, and the average was noted as the players’ internal and external range of motion. The total range of motion was calculated as the sum of the internal and external range of motion.
For the passive range of motion shoulder assessment, participants laid supine on a standard treatment table with their shoulder at a 0-degree rotation, 90 degrees of abduction, and the elbow in a 90-degree flexion. If necessary, the humerus was supported by a towel to ensure neutral horizontal positioning (humerus level with acromial process). First, the anatomical landmarks were placed at the center of the olecranon and the lateral point of the ulnar styloid process, and the digital goniometer was placed to follow the line between the two anatomical landmarks. Second, the examiner started by stabilizing the scapula by putting the thumb on the coracoid process and the four fingers on the spine of the scapula. In this position (0-degrees of rotation), the examiner passively externally/internally rotated the shoulder while stabilizing the scapula. The end range of external/internal rotation was defined when scapular movement was registered by the tester.6,28
Isometric shoulder strength
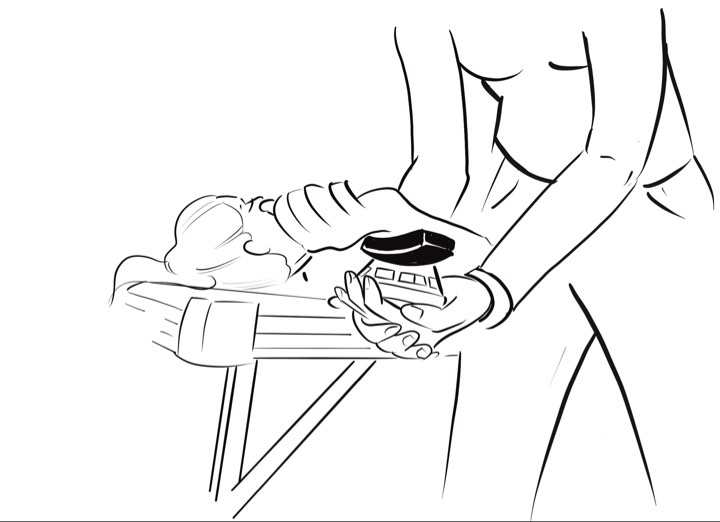
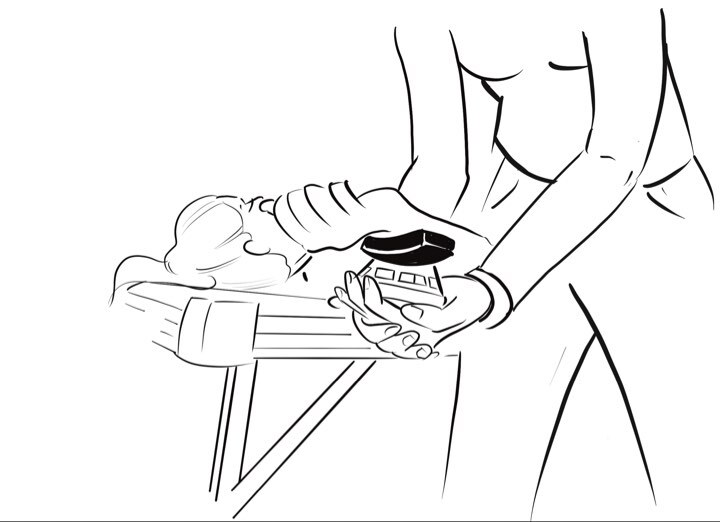
Dominant shoulder internal and external rotator isometric strength was measured using a handheld dynamometer (microFET, Hoggan Health Industries, Salt Lake City, Utah, USA). Participants lay supine on a standard treatment table with their shoulder in 90 degrees of abduction, 90 degrees of external rotation, and the elbow in 90-degrees of flexion, a position modified from Clarsen et al. (Figures 1 and 2).21

The participants were instructed to keep their legs straight and place the opposite arm along their side. The examiner placed the handheld dynamometer, which was strapped around the fingers of hand of the examiner, 1 cm proximal to the radiocarpal joint line. The participants were guided through the movement, and a training sub-maximal trial was performed before the two maximal efforts. The participant was instructed to increase force over three seconds and hold the maximal isometric force contraction for five seconds according to Clarsen et al.21 Two maximal tests were performed with 30 seconds of rest in between, and the best score was registered.21 An isometric strength ratio was calculated by dividing external rotational shoulder strength and internal rotational shoulder strength.
Statistical Analysis
A sample size calculation was based on previously published estimations in external strength containing people with and without pain in the upper limbs of mixed sexes.6,29–31 The target number of participants was 125 subjects, according to an alpha of 0.05 and a power of 0.80.
All data distributions were tested for normality with the Shapiro–Wilk test, histograms, and qq plots. Differences in anthropometrics between sexes were investigated by conducting an independent t-test. A 2 (sexes: men vs. women) x 3 (pain condition: pain, previous pain, no pain) analysis of variance (ANOVA) was used to compare the internal and external shoulder range of motion and strength. If the sphericity assumption was violated, the Greenhouse–Geisser adjustments of the P-values were reported in the results. A post hoc test using Holm–Bonferroni probability adjustments was used to locate significant differences. The criterion level for significance was set at p < 0.05. The effect size was evaluated with η2 (ETA partial squared), where 0.01 < η2 < 0.06 constitutes a small effect, 0.06 < η2 < 0.14 constitutes a medium effect, and η2 > 0.14 constitutes a large effect.32 All variables are expressed as mean ± standard deviation (SD). Statistical analysis was performed using SPSS 27.0 for Windows (SPSS, Inc., Chicago, IL).
RESULTS
A total of 136 elite team handball players: 57 women (age 22.4 ± 4.9 yr., body mass 72.4 ± 8.3 kg, height 1.74 ± 0.06 m) and 79 men (age 22.3 ± 5.2 yr., body mass 90.8 ± 11.8 kg, height 1.89 ± 0.08 m) participated in this explorative cross-sectional study.
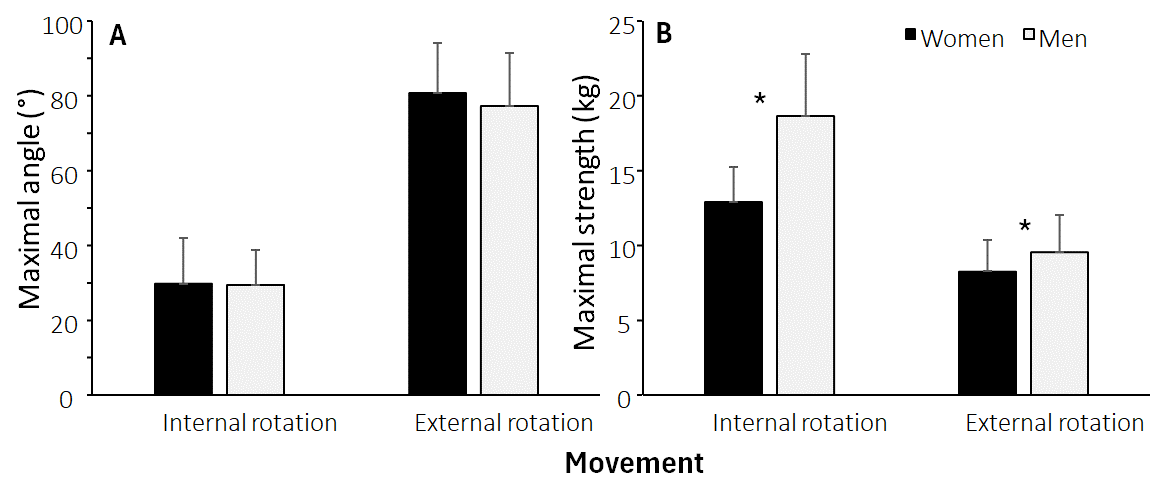
Men were significantly taller and heavier than women (p < 0.001), but no significant difference in age (p = 0.93) between sexes was found. No significant differences in internal (F = 0.54, p = 0.46, η2 = 0.004) and external shoulder range of motion (F = 3.73, p = 0.056, η2 = 0.03) were observed (Figure 3). Furthermore, significant differences in maximal internal (F = 72.3, p < 0.001, η2 = 0.31) and external shoulder rotation strength (F = 8.4, p = 0.004, η2 = 0.06) between sexes were found. Post hoc comparisons revealed that men had greater internal and external shoulder rotation strength than women (Figure 3).
_of_a)_maximal_internal_and_external_shoulder_rotation_angle_range_of_motion_and.png)
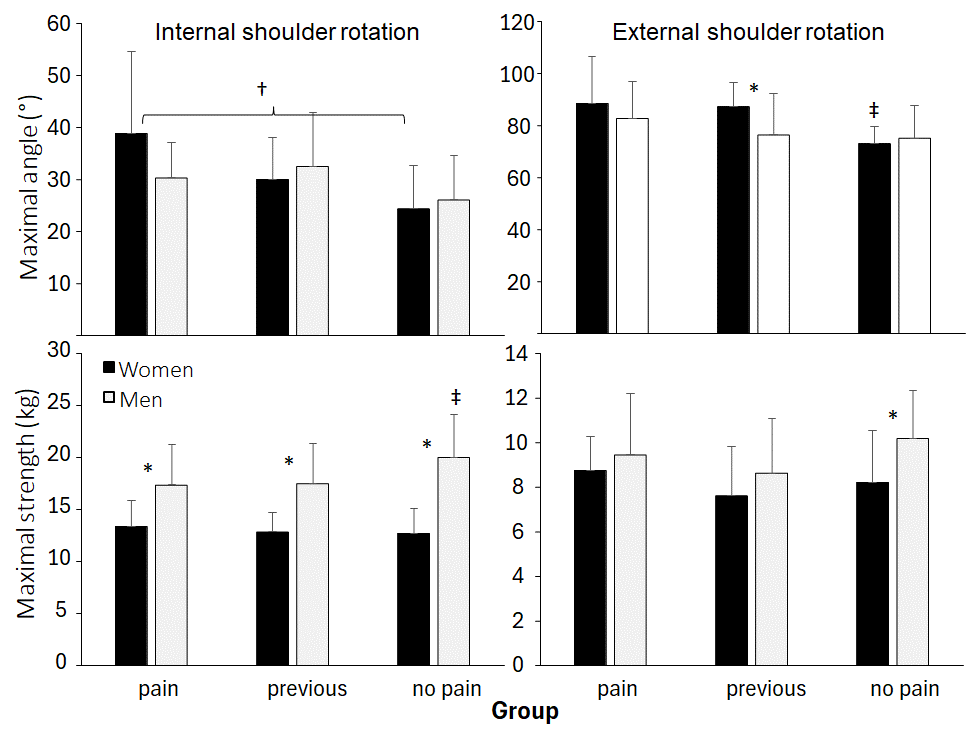
When analyzing the range of motion and shoulder rotation strength while categorized by pain condition, significant effects were found for maximal internal (F = 8.86, p < 0.001, η2= 0.13) and external shoulder rotation range of motion (F = 8.0, p < 0.001, η2= 0.12). In contrast, no significant effects were found for maximal internal (F = 1.7, p = 0.187, η2 = 0.02) and external shoulder strength (F = 2.48, p = 0.088, η2 = 0.01).
Furthermore, a significant sex × pain condition interaction effect was observed for maximal internal shoulder strength (F = 3.2, p = 0.042, η2 = 0.03), while for the other three variables, the interaction effect was not significant (F ≤ 2.9, p ≥ 0.059, η2 ≤ 0.04). Post hoc comparisons revealed that maximal internal and external shoulder rotation angles were significantly lower in the no-pain group compared with the other groups, especially in women (Figure 4). For strength, only the maximal internal shoulder strength was significantly higher in men without pain than in the other two groups (Figure 4). In addition, maximal internal shoulder rotation strength was higher in all pain conditions and maximal external shoulder rotation strength in the no-pain group for men compared with women. Meanwhile, women in the previous pain group had significantly more range of external shoulder rotation than men in this group (Figure 4).
_of_maximal_internal_and_external_shoulder_rotation_angle_and_maximal_internal_a.png)
The isometric strength ratios were significantly different between sexes but not between groups (Table 2), with a higher ratio in men for both external and internal shoulder strength.
DISCUSSION
This study aimed to compare the shoulder rotation strength and rotation range of motion among elite handball players experiencing current or previous non-traumatic shoulder pain with those with no pain. The main findings were that maximal internal and external shoulder rotation strength was higher in men than women, while range of motion was comparable between sexes. Furthermore, maximal internal and external shoulder range of motion was reduced in women with no shoulder pain compared to the other two groups. In contrast, in men, higher internal shoulder rotation strength was observed in the no-pain group than in the other groups.
The only differences in shoulder range of motion were found in women between the three groups. The women in the no-pain group had less passive internal and external shoulder rotation than the other groups (Figure 2), which indicates decreased total range of motion. Almeida et al.20 found a significantly greater GIRD and external rotation range of motion gain among team handball players playing with shoulder pain compared with athletes without throwing-related shoulder pain. Previous research estimated that a GIRD with a 20-degree reduction is a risk factor in developing shoulder pain, but it is only seen as pathological if the total range of motion is significantly different in a side-to-side comparison.22 However, in the present study, the non-dominant side was not measured and thereby this cannot be confirmed. Clarsen et al.21 investigated shoulder problems among Norwegian elite male handball players and found that a reduction in the total range of motion (ROM) in the throwing shoulder was associated with shoulder problems. However, this could not be confirmed in a mixed-sex group of Norwegian elite handball players a few years later, which reported that greater IR ROM had a higher risk of overuse shoulder injuries throughout season.6 In the literature, there have been several assumptions and debates as to why ROM adaptations occur. Muscle tightness,22,33 tightness in the posterior capsule,34 or osseous adaptions like humeral retroversion35 have been discussed as potential causes. However, all the abovementioned assumptions have been made based upon participants from baseball and softball, and only some of these findings have been confirmed in handball.8
Maximal shoulder strength was higher in men than women, especially maximal internal shoulder rotation strength, which is consistent with previous research in handball.6 Gender differences were anticipated due to known physical differences, such as increased muscle mass in elite athletes.12 Furthermore, the test position was modified from previously published protocols, where a 90-degree external shoulder rotation was added due to a closer performance position.16,18,21 However, when analyzing maximal isometric shoulder rotation strength only in men, a significant difference was observed: the no-pain group exhibited greater internal rotation strength than the other two groups, indicating that current or previous shoulder pain influences strength. Although the included handball players were active in offensive and defensive roles, previous literature has shown those with pain or previous pain modified their playing style.19
Pain may affect the function of the muscles around the scapula and shoulder, and a painful arc often leads to changed movement patterns, potentially provoking pain in an existing pathological condition in the shoulder.36 It is possible that some muscles are inhibited by pain and cannot contribute as much to maximal internal shoulder rotation strength.37,38 Notably, men displayed a higher isometric strength ratio than women (Table 2), primarily due to a significantly higher internal shoulder rotation strength in men across all groups compared to the corresponding groups within the women (Figure 2). This difference may suggest that men, within team handball, tend to focus more on strengthening the muscles on the front of the body during training, and therefore potentially leading to a decreased focus on shoulder external rotation exercises.
However, no significant differences in isometric strength ratios were found between the groups. Previous research by Achenbach et al.26 and Lubiatowski et al.8 estimated an isometric strength ratio of 0.70 ± 0.15 among elite youth handball players with shoulder injury symptoms, much lower than the ratios found within all groups in this current study. An explanation for these ratio differences is probably due to the groups tested: elite youth players versus elite adult players. The participants in the current study played at the top elite level, and periodization can be expected to optimize physical capacity during a long season of national and international matches. Thereby, implementation of prevention strategies of external shoulder strength could also be a part of the athlete’s routine, and one might expect the motivation/discipline to do the prevention training to be higher among the elite athletes, especially when one had experienced shoulder pain, while in elite youth players, this is probably not yet established. This may explain why no differences were found between the three groups in external rotator strength, which was expected.31,39–41
LIMITATIONS
The present study has some limitations. The isometric shoulder test was performed using a handheld dynamometer, which was not secured to the ground or a wall, which potentially could influence the readings when participants are too strong for the examiner to keep the dynamometer fixed. Due to the longer limbs within the male group this made the standardized test position on a traditional treatment bench challenging. All clinical tests were conducted by the same physical therapist, which is a strength of the study.42 However, since the physical therapist was the main researcher who also collected the data regarding shoulder pain, thus, the test measurements were not blinded. Moreover, due to the use of only one examiner, the tests were not conducted simultaneously at the same time during the season for all athletes, as it is difficult to test participants in different countries from different leagues all at the same time. Factors influencing the timing of data collection could have influenced the results as Fieseler, et al.23 found that physiological adaptations in the shoulder are not permanent, and athletes dynamically adapt to sport-specific movements during a season and career. In addition, the modification of the testing position should be addressed when comparing this study to others measuring isometric shoulder strength in handball players, as it differs considerably.
Furthermore, this study did not examine the non-dominant extremity, to investigate side-to-side differences, anatomical GIRD, and pathological GIRD43 the investigation was focused on comparing strength and ROM of the throwing arm between handball players with, previous, or without shoulder pain. Thus, whether the participants exhibited abnormal shoulder strength and range of motion (ROM) between the two sides and whether these alterations are different between elite handball athletes playing with and without shoulder pain cannot be answered.
Another limitation is the number of participants in the different categories as there were only 34 in the pain group, 36 participants in the previous pain group, which was less than the no-pain group (n=64). However, when considering together the pain and previous pain groups, who had similar results, the number of participants with pain (at some time) was almost equal to that of the no-pain group. Based upon the limitations observed in the present study, future studies should focus on conducting frequent measurements during a season to provide a better view of the potential changes in elite handball players playing with shoulder pain, previous pain, and no pain to investigate if it would change much over a season or longer time by an examiner that is blinded for information of shoulder pain of the participants. Furthermore, the measurement tool for isometric shoulder strength should be fixed to a wall or ground to avoid eventual arm movements of the participants and measurements should be taken both sides, to investigate if this is different between players with or without shoulder pain.
CONCLUSION
This study provides novel data on top elite handball players, examining how playing with and having a history of shoulder pain influences strength and range of motion, compared to athletes without shoulder pain. A significant difference in strength between male and female athletes was found. Among male athletes, the no-pain group had higher internal rotator strength than the two other groups, indicating that even mild shoulder pain may influence the ability to generate shoulder torque in this muscle group. No significant difference in range of motion was found between male and female athletes. However, female athletes in the no-pain group showed significantly less internal and external rotation range of motion compared to those playing with shoulder pain and those with previous pain. Additionally, female athletes in the previous pain group had a greater external rotation range of motion, which cannot be considered the sole cause of shoulder pain, but a part of the bigger picture. It is important to continue studying the possible connection between shoulder rotational strength, range of motion, and the development of shoulder pain.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
ACKNOWLEGDEMENTS
The authors would particularly like to thank all the elite handball players for participating in the project. Furthermore, we thank the medical staff in the clubs and the Olympic Center for supporting the Nordic throwing shoulder project research.