INTRODUCTION
The pediatric population is vulnerable to anterior cruciate ligament (ACL) injuries. The peak incidence of ACL tears occurs in high school and the rate of resulting reconstruction surgeries has steadily been increasing over the past decades.1–4 Additionally, young athletes recovering from ACL reconstruction demonstrate sub-optimal outcomes with a lower than expected rate of return to play (RTP),5,6 an elevated risk of suffering second ACL injuries,7 and a high likelihood of developing long term disabilities.8
The high risk of re-injury is associated with a large proportion of children and adolescents returning to high risk cutting and pivoting sports following surgery.7 Poor quadriceps strength recovery, identified in young athletes cleared to return to sport,9 brings into question athletes’ preparedness to face the demands of their sports. The management of quadriceps function following ACL reconstruction is a foundational element of a successful recovery, as evidenced by its important place in post-op rehabilitation clinical practice guidelines.10 The key role of post-operative quadriceps strength recovery is further supported by reports that knee extension strength deficits are associated with increased likelihood of not returning to pre-injury level sport,11 suffering a knee re-injury,12 and developing knee arthritis.13
Multiple interventions have been shown to improve quadriceps function recovery following surgery such as resistance training,14 neuromuscular electrical stimulation,15 biofeedback,16 and blood-flow restriction therapy17; however, each of these interventions requires access to health care professionals or resources and may not be available to all individuals. Social determinants of health (SDOH), referring to social and economic factors that influence disease development, access to healthcare, outcomes, and patient’s health status, have been found to contribute to delay in access to care and inferior outcomes following ACL reconstruction.18
During the past decade, researchers have primarily relied on demographics and singular variable proxies such as sex/gender, race/ethnicity, insurance status, and median household income to study the impact of SDOH following pediatric ACL injuries.2,4,19–24 The complexity of SDOH might be better captured by multivariate indices, representing composite measures based on multiple indicators.25 In the past few of years, several index-based approaches have emerged to investigate health disparities following ACL reconstruction including the Area Deprivation Index (ADI), Medically Underserved Areas (MUA) status, Social Deprivation Index (SDI), and Child Opportunity Index (COI).25–28
The interactions between SDOH, represented by a combination of demographics, singular surrogate indicators, and multivariate indices have not been investigated in children and adolescents following ACL reconstruction. Optimizing quadriceps muscle recovery following surgery – and thereby improving post- operative recovery for pediatric patients undergoing ACL reconstruction – requires a more comprehensive appreciation of the interplay between SDOH. Consequently, the purpose of this study was to assess the relationships between SDOH variables, including demographics, singular surrogate indicators and multivariate indices, and quadriceps strength recovery at time of return-to-play testing following pediatric ACL reconstruction.
The authors hypothesized that SDOH will be associated with quadriceps function recovery at six months following surgery and that multivariate indices will help explain the impact of demographics and singular variable proxies.
METHODS
Participants
A retrospective cross-sectional study was conducted by reviewing the electronic medical records of children and adolescents following institutional review board approval. All patients underwent ACL reconstruction at a pediatric tertiary-care center by one senior orthopedic surgeon with both pediatric and sports medicine fellowship training, between May 2016 and October 2022. Patients were included in this study if they (1) underwent primary ACL reconstruction with an autograft, (2) were less than 19 years of age at time of surgery, and (3) completed a standard RTP battery of tests 6 months post-operatively. Six months post-operatively is a critical time point during rehabilitation when athletes frequently initiate the transition toward modified sport activities.29,30 Patients who underwent additional knee surgical procedures performed concomitantly were included. Patients were excluded if they (1) had a past medical history of an ACL reconstruction (involved or uninvolved limbs), (2) underwent ACL reconstruction as part of a two-phase surgical plan, or (3) were diagnosed with congenital ACL deficiency.
Rehabilitation
All patients were provided with a structured rehabilitation protocol31,32 and were recommended to initiate physical therapy at the facility of their choice one-week post-operatively. Weight-bearing and range of motion restrictions were implemented during the first six weeks post-operatively only if ACL reconstruction was performed with an ITB autograft or if a concomitant meniscal repair procedure was conducted. At the time of the six-month post-operative follow-up visit with the surgeon, all patients participated in a standardized physical therapy evaluation designed to help with the RTP decision-making process. During the visits, three physical therapists collected objective measures on range of motion, strength, lower extremity functional performance, and patient-reported outcome measures. All physical therapists had completed a competency training program.
Quadriceps Strength Testing Procedure
Before isokinetic strength testing, each patient participated in a standardized warm-up routine. The program included cycling for five minutes on a stationary recumbent bicycle and completing a dynamic warm-up involving functional movement of the lower limbs. The evaluating physical therapist assessed quadriceps strength recovery using an electromechanical dynamometer (Biodex Medical Systems, Shirley, NY, USA). Quadriceps strength recovery was selected as the primary outcome measure for the study based on its unique relationship with successful post-operative outcomes.11–13 The highest peak concentric torque for knee extensors was obtained out of five trials on each limb, at 60 degrees per second (°/s), from 90 degrees of flexion to full extension. Testing at 60 °/s, the most often selected velocity to objectively assess strength as part of a RTP decision-making process, detects greater quadriceps strength deficits compared to testing at higher speed.33,34 Isokinetic testing at 60 °/s also corresponds to the sole strength testing protocol identified to predict knee re-injury following ACL reconstruction.12 Isokinetic quadriceps testing at 60 °/s, conducted as part of a battery of tests, has shown good to high within- and between-session reliability among individuals who underwent ACL surgery.35 Limb symmetry index (LSI) was calculated by multiplying the ratio between the involved limb peak torque and the uninvolved limb peak torque by 100.
Data Collection
In addition to the isokinetic strength test results obtained from the physical therapy notes, information collected from the medical record included (1) demographic data: age, legal sex (used for legal/administrative purposes), race, ethnicity, and insurance status (dichotomized into public – government sponsored programs – and private categories) (2) surgical detail: graft type, and (3) address of residence at time of surgery. The address was used to obtain the distance to the hospital,36 determine if the patient lived in a rural or urban area (Rural-Urban Commuting Area code – 1.0 to 3.0 coded as urban and 4.0 to 10.6 coded as rural ),4 and calculate four multivariate indices: (1) ADI national percentile, (2) SDI score, (3) nationally normed COI, and (4) MUA status. The ADI national percentile, SDI score, and nationally-normed COI are composite measures calculated from multiple census variables reflecting on the neighborhood socioeconomic resources and advantages.25,27,28 The MUA status, designated by the Health Resources & Service Administration, identifies geographic areas with a lack of access to primary care services.26 Data were collected and managed using Research Electronic Data Capture tools (REDCap) hosted at the University of Arkansas for Medical Sciences.37,38
Statistical Analysis
Data on quadriceps strength recovery, demographic, and SDOH variables, measured on a continuum, were evaluated for normality with box-and-whisker plots and Shapiro-Wilk tests. Normally distributed variables were summarized as means and standard deviations. Variables not meeting the assumption of normality were described by the median and interquartile range. Categorical factors were presented as frequencies and percentages. Univariate regression analyses were initially performed to determine what demographic, surgical, and SDOH variables were significantly associated with knee extension peak torque LSI. Categorical variables were dummy coded for analyses. Non-normally distributed continuous variables were log-transformed.
Variables found to be significant at p < 0.20 on univariate analysis with knee extension peak torque LSI were selected for the next stage in the analysis. Variables were entered into a general linear model (i.e., GLM procedure) after employing the VARCLUS procedure to identify redundant variables within clusters. The final GLM contained only variables significant at the 0.05 level. All analyses were conducted in SAS software, version 9.4 (SAS Inc., Cary, NC, USA)
RESULTS
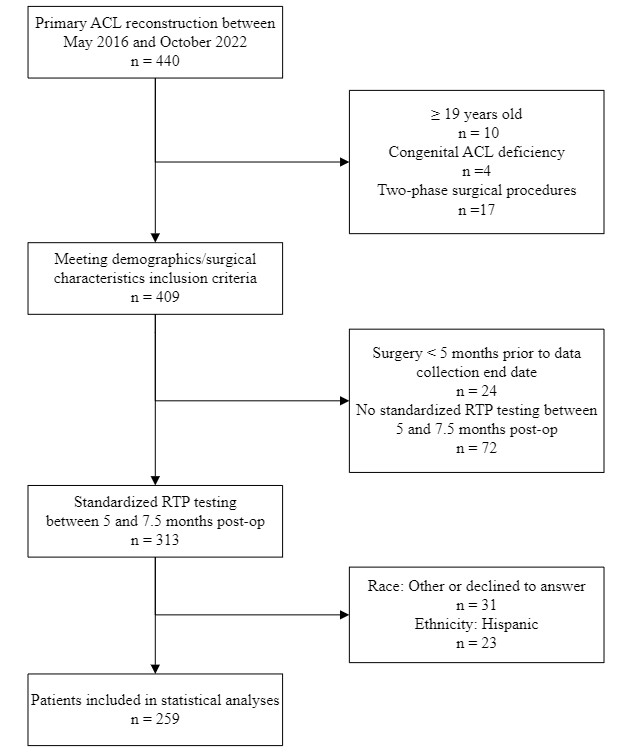
A total of 313 patients underwent ACL reconstruction and completed the six-month (mean 6.0 ± 0.5 months) post-op standardized RTP testing during the data collection time frame (Figure 1); however, 31 were excluded because they declined to designate a race or checked “other”. Additionally, there were seven female and 16 male Hispanic patients that were excluded due to a sample size that was insufficient for analysis and generalization of the results. A total of 259 observations on non-Hispanic, Black or African American and White patients were utilized for analyses. Table 1 displays the demographic and SDOH information for the sample.

The primary outcome variable, knee extension peak torque LSI tested six months post-operatively, ranged from 16.1 to 126.7% with a mean (standard deviation) of 76.4% (21.7). Univariate regression analyses of demographic, surgical, and SDOH variables on knee extension peak torque LSI are shown in Table 2. Patient’s age, graft type, sex, and race, as well as ADI national percentile, SDI score, and nationally normed COI were significantly associated with knee extension peak torque LSI.
Table 3 contains the final general linear model that best accounted for the variance in knee extension peak torque LSI. Each SDOH multivariate indices (ADI national percentile, SDI score, and nationally normed COI) was no longer statistically significant when entered into a model with graft type and age included as covariates. After accounting for variance in knee extension peak torque LSI due to graft type and age, only race, sex and their interaction were statistically significant. Table 4 presents the corresponding adjusted means for knee extension peak torque LSI by race and sex. White males and females and Black or African American males had similar mean values for knee extension peak torque LSI. However, Black or African American females had a significantly lower knee extension peak torque LSI compared to Black or African American males and White patients.
DISCUSSION
The findings of this retrospective study partially support the authors’ original hypotheses. Social determinants of health, represented by demographics and multivariate indices, were statistically significantly associated with quadriceps strength recovery in children and adolescents six months following ACL reconstruction. However, ADI national percentile, SDI score, and nationally normed Child Opportunity Index no longer explained variance in knee extension peak torque LSI after controlling for demographics and surgical characteristics. The only variables remaining statistically significant after controlling for age and graft type were sex and race. Additionally, a significant interaction was noted between sex and race, identifying poorer quadriceps strength recovery specifically in Black or African American females.
Investigation of the impact of race on ACL injury management in children and adolescents is still in its infancy. Conflicting findings have been reported on the relationships between race and ethnicity and access to care,20,22,39 the presence or severity of concurrent meniscus injury,4,20,22,39 and the risk of suffering a second ACL injury.22,23 Bram et al22 identified that Black/Hispanic patients under 21 years of age demonstrated greater knee extension strength and ROM deficits at time of RTP testing. Black/Hispanic children were also less likely to achieve documented physician RTP clearance.22 However, contrary to this study the impact of race/ethnicity on strength recovery was not assessed after controlling for other potentially important variables.
These findings shed further light on the relationship between race and quadriceps strength recovery in young athletes following ACL reconstruction by confirming a statistically significant association while controlling for demographic and surgical characteristics. The effect of race on post-operative outcomes following ACL reconstruction involves the intersection of many variables.40,41 Proposed factors include socioeconomic barriers,28,41,42 lower education and health literacy,41,42 reduced access to health care professionals and gym equipment,22,43,44 and low racial/ethnic concordance with health care professionals.40 However, contrary to the authors’ hypothesis, no SDOH multivariate indices remained statistically significant in the final statistical model explaining quadriceps strength recovery, highlighting the complexity of the mechanisms at play.
In the model utilized, Black or African American females demonstrated inferior outcomes at six months post-operatively compared to Black or African American males as well as both White males and females. To the authors knowledge, sexed (i.e., unevenly distributed between males and females) SDOH have not been reported in the sports medicine literature. Females have been noted to be less likely to engage in muscle-strengthening activities in a non-clinical setting.45–47 However, females have been identified to attend PT at a greater frequency and for a greater total number of visits following ACL reconstruction compared to males.48–50 Black patients, on the other hand, have been reported to attend fewer post-operative physical therapy visits compared to White patients.28 Although a formal investigation is warranted, it is possible that a lower participation in physical therapy in Black patients – and thereby less opportunity to address strength impairments – is compensated to a greater degree in males than females by participation in strengthening activities at school or private gyms.
Female patients have inferior post-operative outcomes compared to males regarding laxity, return to sport rate, self-reported function, and revision rate following ACL reconstruction.51 Children and adolescent girls have overall demonstrated inferior quadriceps strength recovery compared to boys at time of return to play testing.52 Investigation in the root causes of sex disparity in post-operative outcomes have focused heavily on sex-based biological traits but has rarely explored wider social influence and environmental disparities.53 Programs and environments designed to build strength have been described as heavily gendered in ways that disadvantage women’s participation.53 Although limiting factors are believed to vary according to socio-cultural backgrounds, examples of barriers to resistance training participation in school aged girls include gender/sex norms of what it means to be feminine, perceived lack of competence in abilities, lack of positive support and role models, and limited access to equipment and female instructors.53–56
Identifying mechanisms underlying outcome disparity in pediatric orthopedics is the first step in exploring avenues to challenge the status quo.41,42 The development of multicomponent interventions targeting the multiple factors involved is warranted to close the gap in pediatric orthopedic care.55 Initiatives that have been proposed to reduce both racial and sex disparities includes improving access to physical therapy care and gym equipment,4,28,55,56 creating an environment with adequate support from caretakers, peers, role models, and health care professionals,54–58 providing targeted education to all parties while accounting for different perspectives,41,55,56 and promoting a more diverse and representative work force in both clinical and non-clinical exercise settings.41,54,56
Several limitations are important to consider when interpreting the results of this study. Data was collected within a retrospective design allowing for greater sources of bias and confounding variables. The clinical applicability of our results is, however, reinforced by the authentic clinical environment of the RTP testing. Threats to external validity are also evident with the sole inclusion of children and adolescents who underwent ACL reconstruction at a single pediatric site by one orthopedic surgeon. Additionally, due to the racial and ethnic makeup of the eligible patient sample, statistical inferences were reserved to non-Hispanic, White and Black or African American patients. Although caution is required regarding generalization of the findings to other settings and populations, the reduced source of variability strengthens the internal validity of our interpretations. Finally, the information collected in the medical electronic record for race and sex is limited in its ability to accurately quantify all the social constructs at play.4
Further investigations are warranted to create more robust and sophisticated models explaining the relationship between SDOH and post-operative outcomes following ACL reconstruction in children and adolescents. Gaining a better understanding of the impact of the interaction between race and sex on the participation in resistance training within and outside of physical therapy is critical to develop future research projects and test initiatives. Finally, this research focused on quadriceps strength recovery, which is but one of multiple factors across the biopsychosocial framework required to improve to reduce outcome disparity following pediatric ACL reconstruction. Additional research must continue to expand on a more diverse complement of outcome measures, including long-term outcomes such as return to sport rate and risk of second ACL injury.
CONCLUSION
Among SDOH variables, including demographics, singular surrogate indicators, and multivariate indices, only sex, race, and their interaction significantly affected quadriceps strength recovery when controlling for age and surgical characteristic following pediatric ACL reconstruction. This study suggests that Black or African American females have inferior post-operative outcomes at time of RTP testing compared to Black or African American males as well as both White males and females. Further studies should work toward deepening the understanding of the impact of SDOH on post-operative outcomes to identify root causes of disparities and guide strategies required to close the gap in pediatric orthopedic care.
Acknowledgement
The authors would like to acknowledge Parker Davidson, MD, for his contribution to data collection.
The project described was supported by the Translational Research Institute (TRI), grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declarations of Interest
None
Ethical statement
Approval from the University of Arkansas for Medical Sciences Institutional Review Board approved was obtained prior to study commencement. Protocol #: 206414