

INTRODUCTION
Hamstring strain injuries (HSI) is a common sports injury,1–3 with a recurrence rate exceeding 30%.4 Of these recurring HSI, 59% occur within the first year3 and require longer recovery times than the initial injury.4 This high recurrence rate has been attributed to inadequate rehabilitation protocols and premature return-to-play (RTP).5,6
RTP criteria focus on magnetic resonance imaging (MRI) findings,7 pain,8–10 muscle strength,11,12 and flexibility11–13 differences between the injured and uninjured sides. However, relying on these criteria alone has shown limitations in predicting recurrence. The only risk factors consistently supported by strong evidence are a history of HSI and older age, while concentric and eccentric muscle strength and flexibility have not been conclusively linked to injury risk.14 Moreover, while MRI significantly contributes to assessing HSI, it remains challenging to use MRI findings alone to determine RTP criteria or predict recurrence rates.9 These findings suggest limitations in the current physical and imaging assessments to provide RTP criteria.
HSI typically occurs during the late swing or early stance phases of sprinting, when the knee flexion angle is 5–30° and the hip flexion angle is 40–60°.15–17 Additionally, high-speed movements occur at both the hip and knee joints throughout the swing phase.18 Furthermore, HSI frequently occurs during the last 15 min of each half of a match, a period often characterized by fatigue,19 suggesting the importance of evaluating both speed and endurance components.
The maximum-speed single-leg bridge test (MS-SLBT) was designed to incorporate high-speed functional movements into the existing single-leg bridge test (SLBT), to evaluate hamstring endurance at joint angles that mimic the mechanism of HSI.20 The MS-SLBT involves placing the heel on a platform and raising the buttocks as fast and as high as possible.
The purpose of this case report was to highlight the use of the MS-SLBT to identify functional impairments in a rugby player with a fourth recurrence of HSI that were not detectable with conventional assessments, and to describe how HSI can be addressed by using the test as an intervention.
Case Description
Subject Information
The subject was a 21-year-old male rugby player (height: 170.9 cm, weight: 69.8 kg) with a history of three right medial HSI over the preceding 4 years. The initial injury occurred four years prior and was a non-contact Grade II right medial HSI. The subject sustained another injury in the same area in 2022, and a proximal right medial hamstring injury in 2023.
Clinical Findings
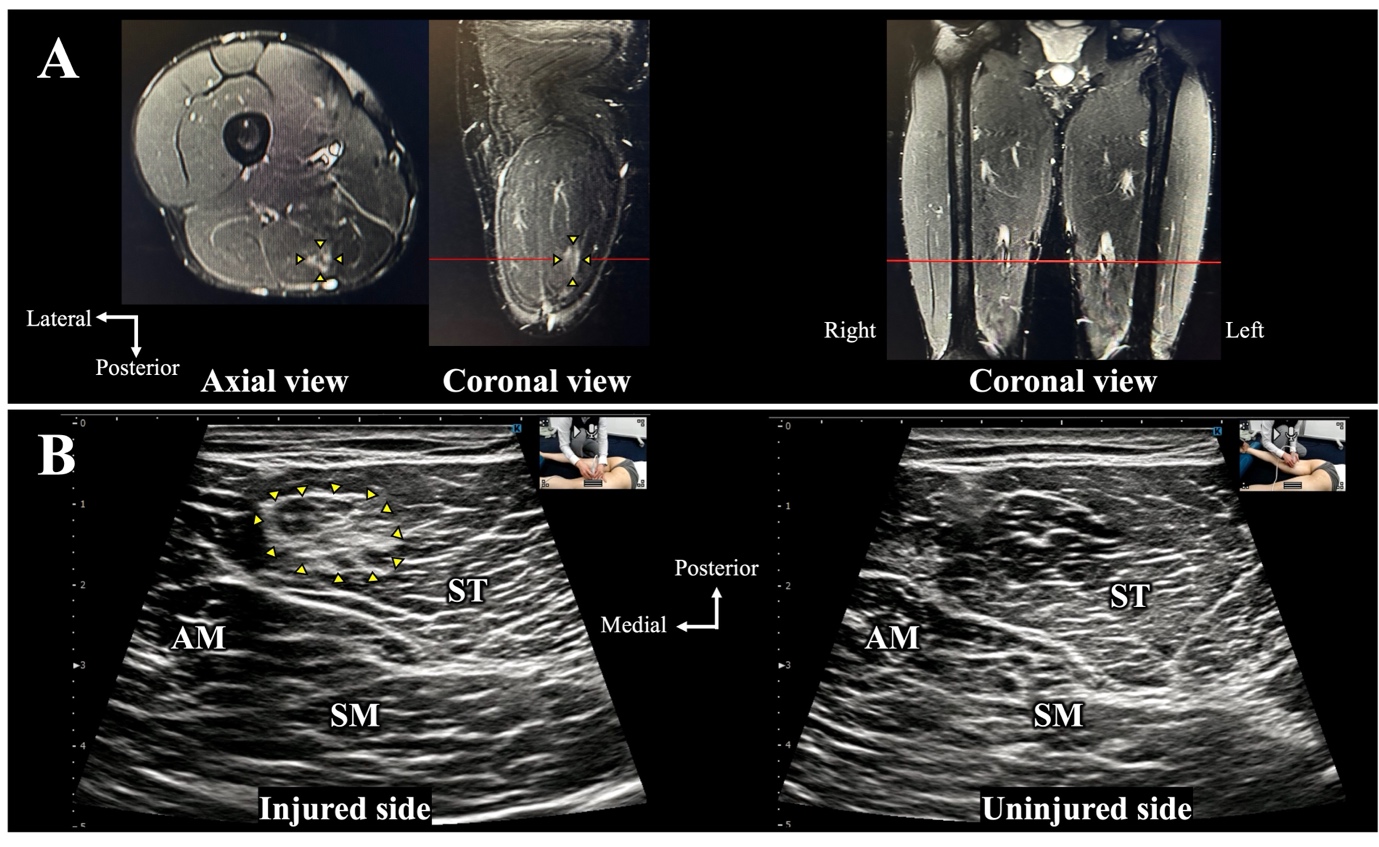
In March 2024, the subject developed acute pain in the posteromedial area of the right thigh after sprinting during a match. At the time of injury, physical examination revealed tenderness and discomfort in the posteromedial thigh during extension and resistance to knee flexion. On six days post-injury, the subject was examined by an orthopedic surgeon and diagnosed with a mild right medial HSI. MRI performed on 19 days post-injury confirmed a Grade I injury in the semitendinosus, and ultrasound images (SONIMAGE MX1 SNiBLE yb, KONICA MINOLTA, INC., Tokyo, Japan) revealed irregularities in the muscle fibers of the semitendinosus at the site of pain (Figure 1).

Timeline of Events
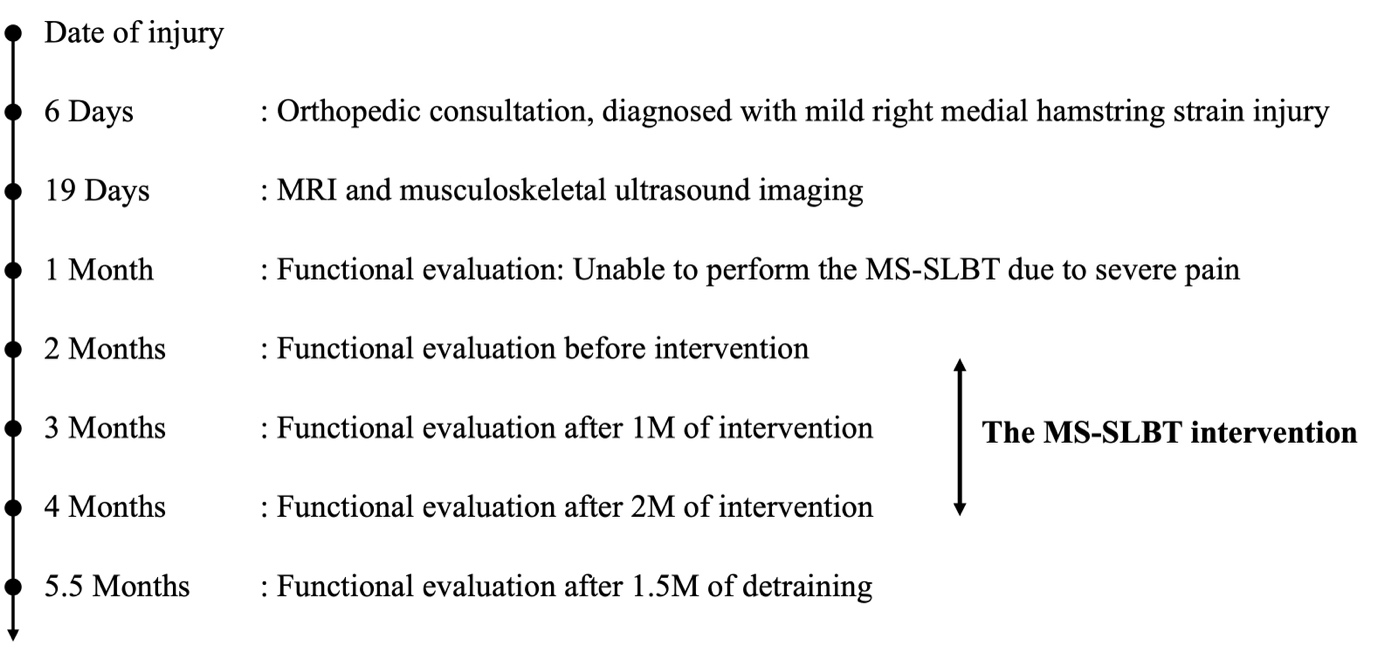
Functional assessments, including visual analog scale (VAS) pain assessment and MS-SLBT performance, were conducted as outlined in Figure 2.
.jpeg)
Diagnostic Assessment
At one month post-injury, pain was assessed using the VAS (0–100 mm). Tenderness was present; however, there was no pain during stretching, isometric contraction at 30° of knee flexion in the prone position, eccentric contractions using the Nordic hamstring exercise (NHE), or during maximal effort sprinting. Additionally, there was no difference between the injured and uninjured sides in isometric knee flexor strength and flexibility assessments using the Active Knee Extension Test. However, during the MS-SLBT, the subject experienced severe pain, with a VAS score of 60.1 and significant apprehension during the first attempt, which contributed to his inability to complete the 20-repetition endurance test (Table 1).
One month later, at two months post-injury, the MS-SLBT was conducted again. The results indicated a reduction in pain (VAS, 15 mm) with no discomfort, allowing for 20 repetitions. However, the buttock-raising height and speed remained lower on the injured side, whereas the heel-bearing force showed no significant differences (Table 1). To address these functional deficits, an intervention was initiated using MS-SLBT as the primary intervention. The exercises were performed as a self-managed home exercise program using a 40-cm chair or platform. An instructional session was conducted before the intervention to ensure proper movement execution and to make necessary adjustments, as this was the first time the MS-SLBT exercise had been applied. The intervention protocols are shown in Table 2. Initially, the subject was advised to perform four sets per day for six to eight weeks; however, the set count was reduced to three sets due to reports of excessive fatigue.
Outcome
Subject compliance was monitored through the daily submission of exercise videos via email, with a compliance rate of 94.3%. Functional evaluations were conducted monthly, and an evaluation of sustainability was carried out after one and a half months of detraining period. Improvements in knee flexor torque and flexibility were noted after both the one month and two months of intervention, and sustainability was assessed after a one and one half month of detraining period (Table 1). Improvements in buttock-raising height, speed, and heel-bearing force were also observed after the intervention. Figure 3 shows the improvement in buttock-raising height after the intervention. During the before intervention (Figure 3a), the buttock-raising height shows the center of the hip joint clearly positioned below the 40-cm platform height. One month (Figure 3b) and two months after the intervention (Figure 3c), a marked improvement is shown, with the center of the hip joint clearly positioned above the 40-cm platform, indicating a significant increase in buttock-raising height. After one and a half months of detraining (Figure 3d), although there was a slight decrease, the center of the hip joint remained aligned with the 40-cm platform, indicating that the effects of the two months of intervention were maintained.

The progression of buttock-raising height and speed over 20 repetitions showed notable increases in height and speed after one month of intervention, with further enhancement in endurance after two months of intervention (Figure 4). The buttock-raising height and speed were maintained after one and a half months of detraining, although the heel-bearing force decreased slightly.

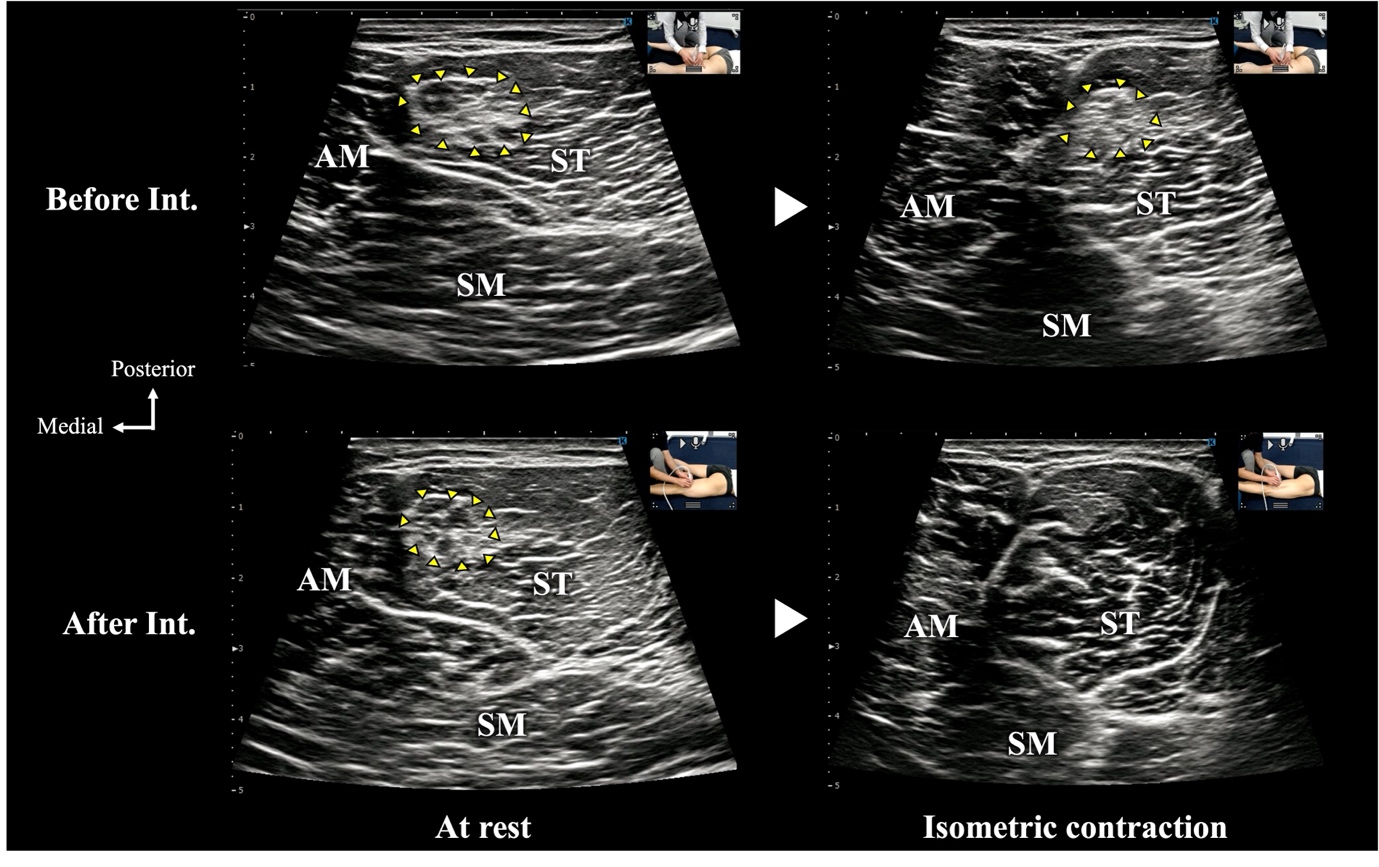
After one month of intervention, the pain during the MS-SLBT disappeared, and although tenderness remained at VAS 10.5 mm, all pain resolved after two months of intervention (Table 1). When comparing ultrasound images before and after the intervention, a reduction in muscle fiber irregularities was observed along with centralization of muscle contraction and improvements in contraction speed on the short axis (Figure 5).

DISCUSSION
This case report demonstrates that in a rugby player with a history of multiple HSI, there were no significant differences in muscle strength and flexibility between the injured and uninjured sides at one month post-injury. Despite being able to perform the NHE without pain, the MS-SLBT was the only test that elicited pain and apprehension. Additionally, at two months post-injury, although other evaluation parameters showed no differences, the MS-SLBT identified deficits in buttock-raising height, speed, and heel-bearing force. The buttock-raising height on the injured side during the MS-SLBT was 0.19 m (14% lower than the uninjured side), and the buttock-raising speed was 0.83 m/s, 18% lower than that on the uninjured side. Data from a cohort of 26 healthy recreational athletes showed that the average buttock-raising speed is 0.98 m/s,21 indicating that 0.83 m/s represents a significant functional deficit. This suggests that even in cases of mild HSI or during the recovery phase, when a patient is asymptomatic and meets the criteria for RTP,22 MS-SLBT can reveal pain and functional deficits through high-speed, biarticular movements. While the SLBT has previously been shown to be inadequate for assessing isolated hamstring endurance in healthy individuals23 or for evaluating maximal hamstring strength,24 its applicability to dynamic and high-speed biarticular movements remains underexplored. These findings suggest that the SLBT may fail to fully capture the functional characteristics of the hamstrings, particularly those dominated by Type II fibers,25,26 which play a crucial role in high-speed movements.
The MS-SLBT intervention targeted high-speed concentric contractions of the hamstrings to improve buttock-raising height, speed, and force output, as well as increase muscle strength and flexibility. This is likely because high-speed training greatly contributes to muscle strength and activation.27,28 After HSI, a decrease in contraction capacity due to chronic changes in the musculotendon structure, such as fibrosis or scarring, may reduce contraction capacity.29 In this case, ultrasound images in the short-axis view showed a reduction in muscle fiber irregularities and improvements in muscle contraction speed and performance. These findings suggest that the MS-SLBT intervention may induce changes in the musculotendinous structure of injured areas. Furthermore, after two months of intervention, the absolute values of buttock-raising height, speed, and heel-bearing force decreased slightly compared to after one month of intervention. The intervention protocol involved setting low repetition counts (5–10 repetitions) for weeks 1–4, focusing on speed, and higher repetitions (15–30 repetitions) for weeks 5–8, focusing on endurance. However, at week 6, the subject reported excessive fatigue due to the increased number of repetitions per set, which led to a modification of the intervention protocol and a reduction in the number of repetitions per set. Follow-up videos revealed a decline in movement speed and consistency owing to fatigue, suggesting that the high repetition count per set in this protocol may have contributed to these issues. Therefore, when using this protocol in a rehabilitation setting, it may be necessary to consider the number of repetitions per set and perform exercises at an intensity that maintains a high-speed movement.
The results of this case report suggest that the MS-SLBT may have clinical applications as a functional assessment and intervention tool. By revisiting the mechanism of HSI and incorporating speed and endurance assessments, the MS-SLBT allows the evaluation of speed and endurance functions in addition to muscle strength and flexibility evaluations. Furthermore, the presence of functional deficits even at two months after a mild HSI may explain the high recurrence rate within the first month post-RTP.3 Given that using the test as an intervention method effectively improves functional deficits within one month, MS-SLBT has the potential to become a part of rehabilitation protocols and return-to-play criteria.
There are limitations to this case report regarding the utility of the MS-SLBT. First, in this case, the HSI involved the semitendinosus rather than the more commonly injured biceps femoris. Although the functions of the biceps femoris and semitendinosus are similar, there are slight differences in their roles. Therefore, although this method may be useful to detect residual dysfunction in semitendinosus injuries, it remains unclear whether similar findings would apply to biceps femoris or semimembranosus injuries. Second, the follow-up period was short, and it remains uncertain whether resolving the function deficits identified using MS-SLBT can prevent future recurrences.
CONCLUSIONS
The MS-SLBT provided a specific and valuable tool to assess concentric contraction deficits in the hamstrings during high-speed movements in a rugby athlete with HSI. Additionally, using the MS-SLBT as an intervention resulted in improvements in high-speed movement performance, muscle strength, and flexibility, along with a reduction in muscle fiber irregularities and enhanced coordination and centralization of muscle contraction during isometric hamstring contractions.