

INTRODUCTION
Isolated Posterior Cruciate Ligament (PCL) injuries or multiligament PCL injuries alter knee biomechanics with excessive posterior tibial translation, resulting in pain, symptomatic knee instability and articular degeneration.1,2 A recent review presented an update on when to manage the PCL injury non-operatively and when to choose surgical treatment.3 The non-operative management with a focus on ligament healing is typically the first-line treatment for acute isolated PCL injuries Grades 1-3.2,4,5 General principles of non-operative management include avoiding posterior tibial translation in the initial period to optimize ligament healing, as well as progressive training with an emphasis on Range of Motion (ROM) and quadriceps-dominated strength exercises.1,5,6
Few studies have reported clinically relevant long-term subjective outcomes of prospectively followed non-operative management of patients with acute PCL injuries.2,7,8 In a study by Shelbourne et al.2 the authors reported a mean International Knee Documentation Committee Subjective Knee Form (IKDC) score of 73 points at a mean of 17 years after injury in 68 patients. Another study by Ahn et al.8 with 38 patients showed a mean IKDC score of 83 points at two-year follow-up. A third study by Boynton and Tietjens7 used a standardized questionnaire and reported a mean functional score (maximum 50 points) of 40 points in 30 patients 13.2 years after injury. Additionally, Tegner Activity Scale (TAS) scores ranging between level 7 and level 8 have been reported after non-operative PCL injury treatment4,7,9 These studies have investigated patient-reported outcomes from various time points after non-operative management without including a baseline and results were reported as one final outcome. The studies were not able to examine the possible statistically significant improvements in patient-reported outcomes from baseline to final follow-up. A recent study investigated changes in patient-reported outcomes from injury to specific follow-ups.10 However, the study only presented one- and two-year follow-up and not long-term follow-up. Furthermore, reviews have reported that previous studies have not sufficiently guided the non-operative management of PCL injuries in terms of describing the interventions used.11–14 In order to establish an optimal set of guidelines for the non-operative rehabilitation there is a need for prospective studies reporting long-term outcomes of well-described non-operative interventions. Therefore, the primary aim was to investigate long-term (after five years) patient-reported outcomes of a physiotherapy-led exercise and support brace intervention in patients with an acute PCL injury. The secondary aim was to report conversion to surgical PCL reconstruction.
MATERIAL AND METHODS
STUDY DESIGN
All patients gave informed consent to be included in this prospective case series. The study was conducted in accordance with the World Medical Association Code of Ethics and the Danish Code of Conduct for Research Integrity and was notified to the Central Jutland Region Committee on Health Research Ethics (case number 1-10-72-1-19). The Danish Data Protection Agency approved the handling of personal data (1-16-02-549-13).
PARTICIPANTS
Eligible patients from the study cohort who originally had not undergone reconstructive surgery were invited to participate in this five-year follow-up. The cohort included patients with both isolated PCL injury and multiligament PCL injuries diagnosed by Magnetic Resonance Imaging (MRI) and clinical examination. Patients with fibular head fractures or avulsion fractures of the tibia were not included. All patients were recruited consecutively between June 2015 and January 2018 and represent the distribution of isolated PCL injuries and multiligament PCL injuries at Aarhus University Hospital, Denmark. The study cohort was followed for five years.
EXERCISE AND BRACE INTERVENTION
The study participants had all undergone non-operative management, which included a 12-week PCL support brace intervention and a 16-week progressive exercise protocol. The non-operative intervention was previously described by other authors10 and has been described in detail in Additional File 1. The exercise intervention typically focused on effusion control, and progressive ROM and strength training including proprioception and knee stability exercises. All exercises were individually selected and tailored to each patient.
DATA COLLECTION
Patient-reported outcomes were mailed to patients and prospectively recorded at the five-year follow-up. Previously published one- and two-year follow-up data were presented in this manuscript to examine improvements in patient-reported outcomes.10 Data on possible conversion to surgical PCL reconstruction were retrospectively extracted from patients’ medical records.
PRIMARY OUTCOMES
The primary outcome measures were the IKDC, the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the TAS.15–17
The IKDC is a site-specific score and it is one of the most frequently used outcome measures for patients with ACL or PCL deficiency undergoing non-operative or surgical management.18 Unfortunately, the IKDC has not been validated in a PCL injury population. The Danish translation of the IKDC score has demonstrated excellent test-retest reliability at group and individual level and adequate responsiveness with an intra class correlation of 0.94, standard error of measurement of 2.6 points and a minimal clinically important change of 7.0 points.19 The IKDC provides a total score ranging from 0 to 100 points with 100 points representing the best possible outcome. The KOOS is a site-specific, valid, reliable and responsive instrument measuring short-term and long-term knee symptoms and function in patients with osteoarthritis and several types of knee injuries, including ACL injuries, meniscal injuries and cartilage injuries after non-operative and operative interventions.20,21 The KOOS has high test-retest reliability with an ICC across subscales ranging from 0.61 to 0.95 and the minimum detectable change across subscales ranging from 5 to 12 points.22 The questionnaire consists of 42 questions divided into five separate subscales: Pain, Symptoms, Activities of Daily Living, Function in Sport and Recreation, and knee-related Quality of Life (QoL). Each subscale ranges from 0 to 100 points with 100 points representing the best possible outcome. A difference of 8 to 10 points in a subscale is usually considered to represent a clinically relevant effect. It is recommended to evaluate each subscale independently when considering outcome measures.21
The TAS is the most widely used activity rating scale for patients with knee disorders and it has been tested for validity in an ACL injury population23,24 The scale consists of 11 levels grading perceived physical activity level based on work, sport and recreational exercise. Level 0 is “on sick leave/disability” and level 10 is “participation in competitive sports such as soccer at a national or international elite level.” For reliability the Danish translation of the TAS showed acceptable reliability. The intra-class correlation coefficient was 0.7, the standard error of measurement was 0.7 and the smallest detectable change was 2.1.17 These three patient-reported outcome measures were used for several reasons; they are validated for Danish patients, they have acceptable reliability and responsiveness, they are not too time consuming for patients to complete, and they were used in a previous study investigating patient-reported one- and two-years follow-up in the same patient cohorte.10 Importantly, the IKDC, the KOOS and the TAS were found to be capable of capturing the symptoms and disabilities of greatest importance to ACL injury patients treated surgically.25 Patients in this study are not the same as ACL reconstruction patients. However, despite the PCL’s ability to heal, many studies on non-operative treatment have found there to be some degree of residual knee laxity.2,4,26,27 The risk of symptomatic knee instability as well as the risk of developing articular degeneration is present in both ACL reconstruction patients and non-operatively treated PCL injury patients. The isolated PCL injury patients typically report higher patient-reported scores than those of multiligament PCL injury patients having sustained more extensive injuries. Hence, it is reasonable to assume that one single patient-reported outcome measure would not be capable of capturing the symptoms and dissabilities in a group of isolated PCL injury and multiligament PCL injury patients. The authors reported that the IKDC overall outperformed the KOOS regarding patient perceived importance. However, the KOOS subscales Function in Sport and Recreation and knee-related QoL outperformed the IKDC.
SECONDARY OUTCOME
Patients that were converted to surgical PCL reconstruction were identified by medical records as a secondary outcome.
STATISTICAL ANALYSIS
Continuous data were reported as mean with standard deviation (SD) if they were normally distributed, otherwise they were reported as median with interquartile range. A paired t-test was used to compare the normally distributed data from baseline to five-year follow up. Wilcoxon rank sum was used for non-normally distributed data. Categorical data were reported as numbers and percentages. Changes from diagnosis to follow-up were analysed using a mixed-effects model with patients as a random factor and time as a fixed factor. The STATA 18.0 software package (StataCorp, College Station, TX, USA) was used for data analysis, and results were considered statistically significant if p < 0.05. The aim of this study was to investigate changes in patient-reported outcomes (IKDC, KOOS and TAS ) from baseline to five-year follow-up. The sample size was based on an initial inclusion of 50 prospectively included patients. Patient-reported outcome data were reported as one cohort (including both isolated PCL injuries and multiligament PCL injuries), as the study population was considered representative of the distribution of isolated PCL injuries and multiligament PCL injuries at Aarhus University Hospital. Additionally, a subgroup analysis was performed with the cohort divided into isolated PCL injuries and multiligament PCL injuries. The subgroup power analysis revealed that it was not possible to demonstrate a potential clinically relevant difference of 10 points in the IKDC score with 28 and 22 patients in the isolated PCL injury and multiligament PCL injury groups respectively.
RESULTS
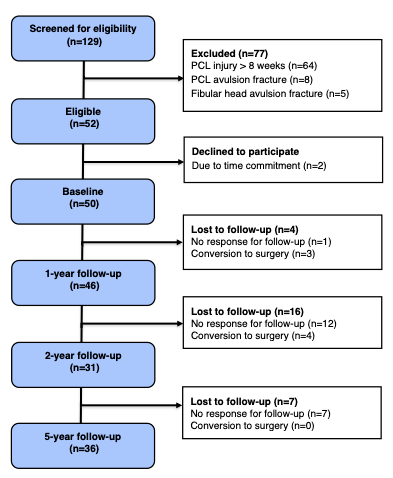
During the initial study period, 50 out of 52 eligible patients were included (Figure 1).

The characteristics of the included patients are reported in Table 1.
PRIMARY OUTCOME
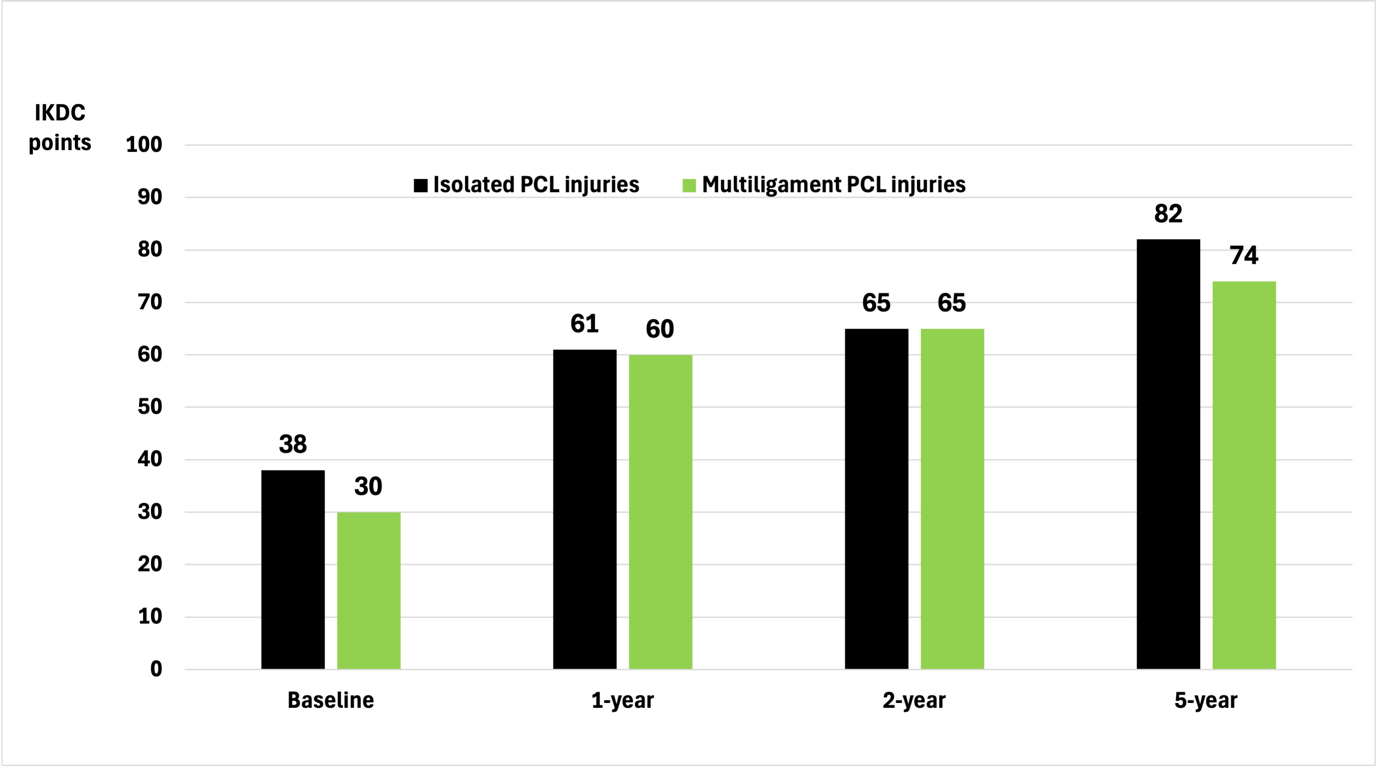
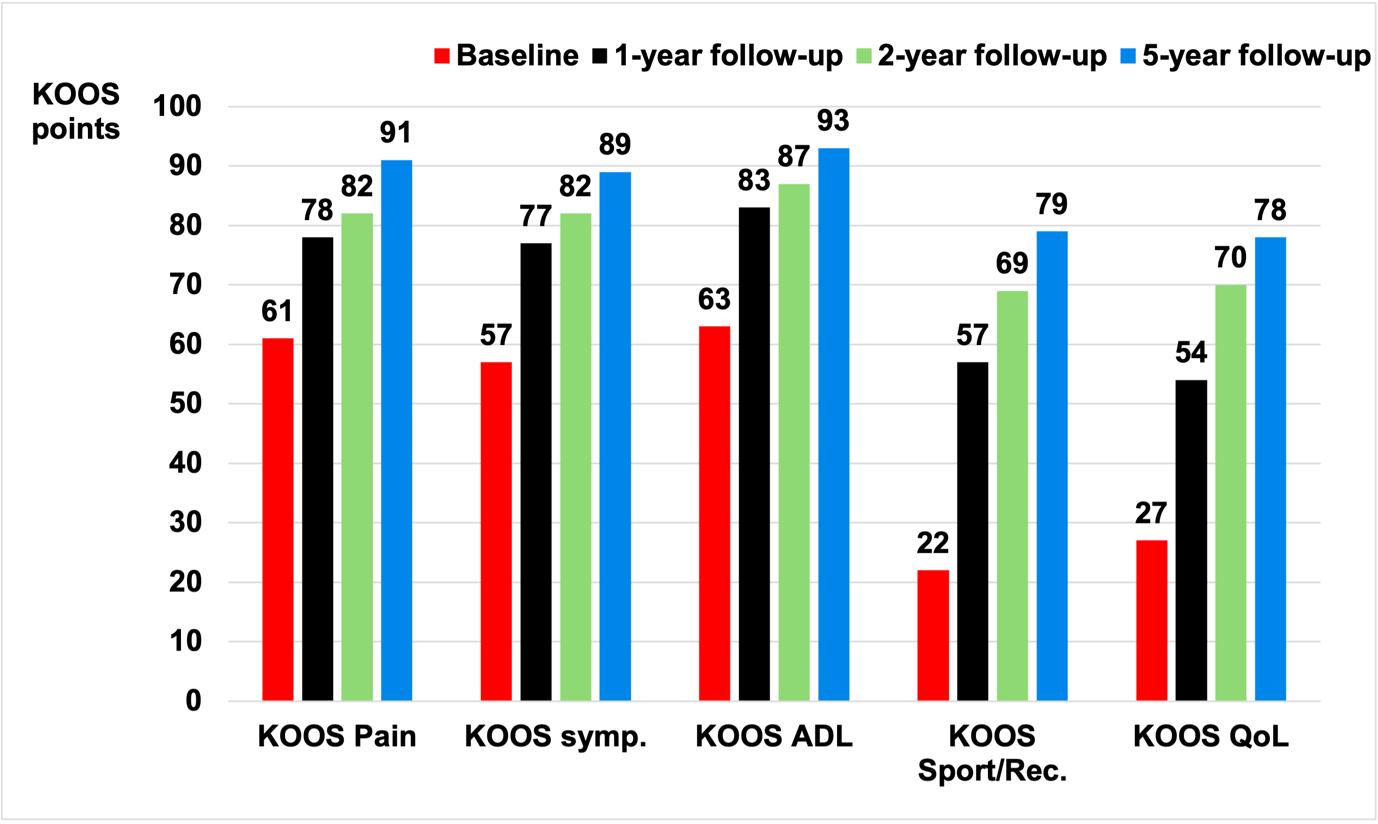
The mean IKDC score for the full cohort improved by a statistically significant amount from 36 points at baseline to 79 points five years after injury (p < 0.001). Furthermore, the IKDC score improved by a statistically significant amount from two- to five-years follow-up from 65 points to 79 points (p < 0.001). There was a statistically significant score improvement for all five KOOS subscales between baseline and the five year follow-up. However, there was no statistically significant change in the five KOOS subscale scores from two-year follow-up to five years after injury, as shown in Figure 2.

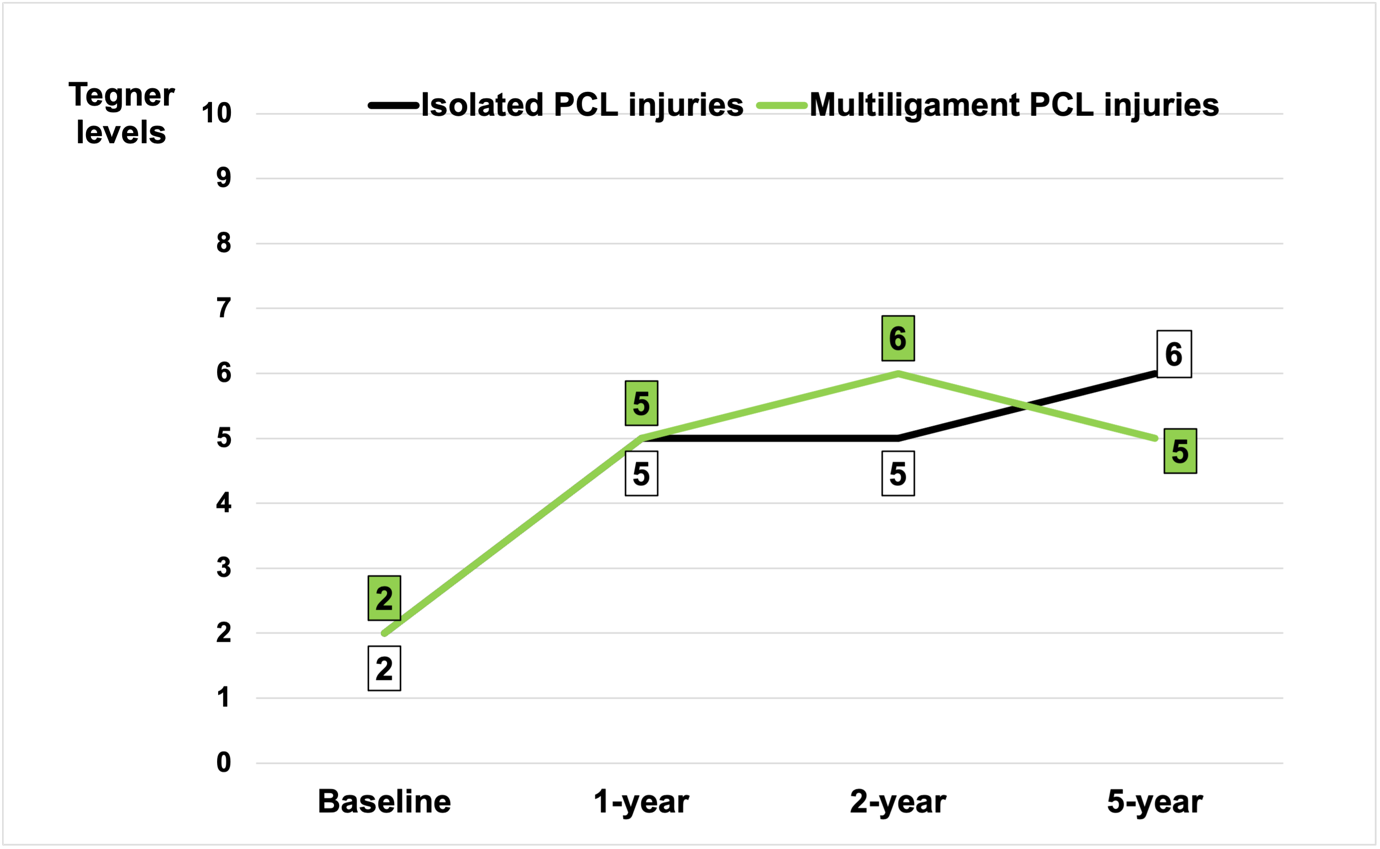
For the separate isolated PCL injury and multiligament PCL injury cohort’s patient-reported scores demonstrated that multiligament PCL injured patients had lower initial patient-reported scores than isolated PCL injured patients which also was present at five years follow-up. (Figures 3-6).




The mean TAS improved by a statistically significant amount from 2 at baseline to 5 at final follow-up five years after injury (p < 0.001).
SECONDARY OUTCOME
No patients underwent PCL surgery between two and five years of follow-up. During the period from baseline to two years of follow-up, seven patients (14%) underwent PCL surgical reconstruction. Of the seven surgically treated patients, two had an isolated PCL injury (7.1% conversion rate) and five had multiligament PCL injury and were classified according to the Schenck Knee Dislocation Classification28 as total knee dislocation injuries (22.7% conversion rate). The median time from initiation of non-operative intervention to PCL surgery was 13 months (range 10-14 months).
DISCUSSION
The primary finding of the present study was the improvements in patient-reported outcomes observed from baseline to five-year follow-up in patients with acute PCL injury initially treated with a standardized brace and exercise intervention. The secondary finding was that none of the patients required PCL surgery from two- to five-year follow-up. These results are novel because previous studies investigating patient-reported outcomes with long-term follow-up were based on mean scores from various time points without a baseline score. Consequently, those prior studies were not able to report the changes in the patient-reported outcomes over time. However, as there was no control group included in the study design, the authors do acknowledge that the statistically significant changes in this study from baseline to the final five-year follow-up may be due to causal interference between the non-operative intervention and the measured outcomes. On the contrary, the authors believe that it would have been unethical not to offer treatment to all patients. Furthermore, rehabilitation adherence cannot be documented as no health technologies or training diary was included in the intervention. In addition, this study investigated and reported the number of patients who converted to surgical treatment. This was not the aim of previous studies investigating outcomes of non-operative management and therefore the number of patients who converted to PCL surgery was not fully reported in detail.
In the present study patient-reported outcome scores are slightly lower than in previous studies of non-operative treatment with long-term follow-up. Patel et al.27 reported an IKDC score of 84 points and a mean TAS score of 7 seven years after injury in 57 patients with isolated PCL injury. In addition, Shelbourne et al.26 found a mean IKDC score of 83 and the mean TAS score of 8 after eight years of follow-up. In another study with 14 years follow-up Shelbourne et al.4 reported a mean IKDC score of 73 and a mean TAS level of 6. The slightly lower patient-reported scores in the present study may partly be explained by the shorter follow-up time compared to the above-mentioned studies. Also, these previous studies were investigating outcomes after non-operative management of acute isolated PCL injuries, whereas the present study represented 28 isolated PCL injuries and 22 PCL injuries in multiligament injuries. It is therefore plausible to assume that patients with multiligament PCL injuries have a longer and probably more limited recovery. This assumption is supported by the patient reported outcomes. These data suggest that the group of patients with multiligament PCL injuries have lower scores at baseline and do not achieve the same level of scores as the group of patients with isolated PCL injuries five years after non-operative management. No further conversion to PCL reconstruction was required from two to five years follow-up for both isolated and multiligament PCL injuries. These data support the importance of non-operative management (as described in Additional File 1) as a first-line treatment for acute PCL injuries in the sense that successful early outcome with the non-operative management results in continued good outcome up to five years. In addition, the present results show that multiligament PCL injuries do not always result in pain and chronic instability without surgery but can be managed with a brace and an appropriate physiotherapy strategy. However, in the case of knee dislocation, surgical treatment could be considered as the first line of treatment as there is a 23% conversion rate from non-operative treatment to PCL reconstruction found in the study. The authors acknowledge that further research is needed to develop a stronger evidence-based foundation for the management of both isolated PCL injuries and multiligament PCL injuries.
There are some limitations that must be considered when interpreting the results of this study: First, selection bias may exist but has been minimized as the present case series represents the distribution of isolated PCL injuries and multiligament PCL injuries at Aarhus University Hospital. Patients who met the inclusion criteria were included consecutively because they had an acute PCL injury and not because they presented to the clinic with symptoms related to chronic PCL laxity. Finally, this study reported seven patients who underwent PCL reconstruction before the five-year follow-up. This left 43 patients in the case series available for this final follow-up. However, only 36 completed the five-year follow-up and there is a risk of underpowering the final follow-up. However, the authors believe that the results of the present study add relevant information for clinicians and may help to optimize PCL injury management.
CONCLUSION
Patients with acute PCL injury showed significant long-term improvements in patient-reported outcomes after five-year follow-up with non-operative treatment with a standardized brace and exercise intervention. The need for PCL reconstruction remained low and only occurred within the first two years of non-operative management. However, surgical management could be considered as first line treatment in case of knee dislocation (multiligament) injury.