Introduction
Glenohumeral joint instability related to repetitive throwing is a common issue in overhead sports such as baseball.1,2 These conditions typically arise from overuse and lead to significant stress on the glenohumeral joint.3 The glenohumeral joint is structurally unstable and even minor deviations or rotational abnormalities can result in severe dysfunction.4 This instability can lead to significant functional impairment, progressing to rotator cuff tears or labral injuries, and further compromising joint dynamic stability.5 In subjects with anterior shoulder instability who are not candidates for surgery, the effectiveness of conservative treatments remains unclear.6
The rotator cuff muscles play a crucial role in dynamically stabilizing the shoulder and ensuring smooth glenohumeral joint motion.7 When these muscles become dysfunctional, the axis of shoulder rotation is disrupted, often leading to chronic inflammation, pain, and structural failure.6 Clinically, patients with shoulder instability often experience symptom relief when the anterior shoulder is manually stabilized. The relocation test, which involves anterior stabilization of the shoulder of a patient with anterior instability or apprehension, is a representative physical examination test for assessing shoulder stability.8 This manual intervention serves to enhance joint centration and reduce rotational axis deviation, thereby alleviating symptoms. However, it is not feasible to provide continuous manual support during dynamic shoulder movements. In response, the authors developed a novel figure-eight taping technique to protect vulnerable structures in the anterosuperior shoulder, specifically the rotator cuff interval, while improving alignment and stabilizing the rotational axis of the glenohumeral joint.
Herein, this case report describes the immediate and sustained effects of a novel figure-eight taping technique for a recreational baseball player with shoulder instability.
CASE DESCRIPTION
The subject of this case was a 41-year-old right-hand-dominant male former semi-professional baseball pitcher who competed at a national level. The subject had been unable to pitch for six years because of progressive shoulder pain that had worsened significantly over the prior month, interfering with his activities of daily living.
Examination
Clinical Findings
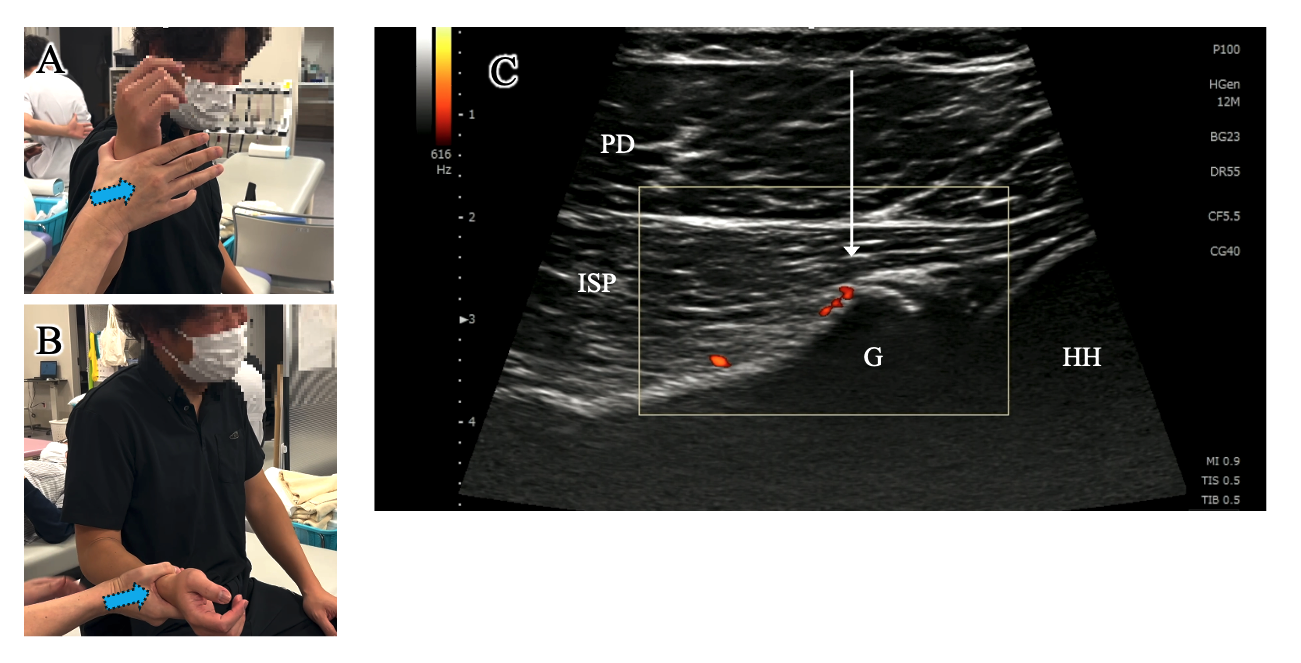
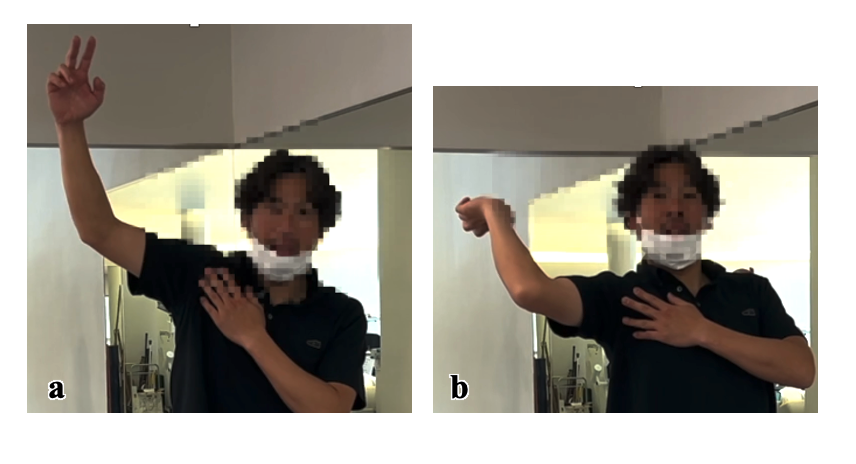
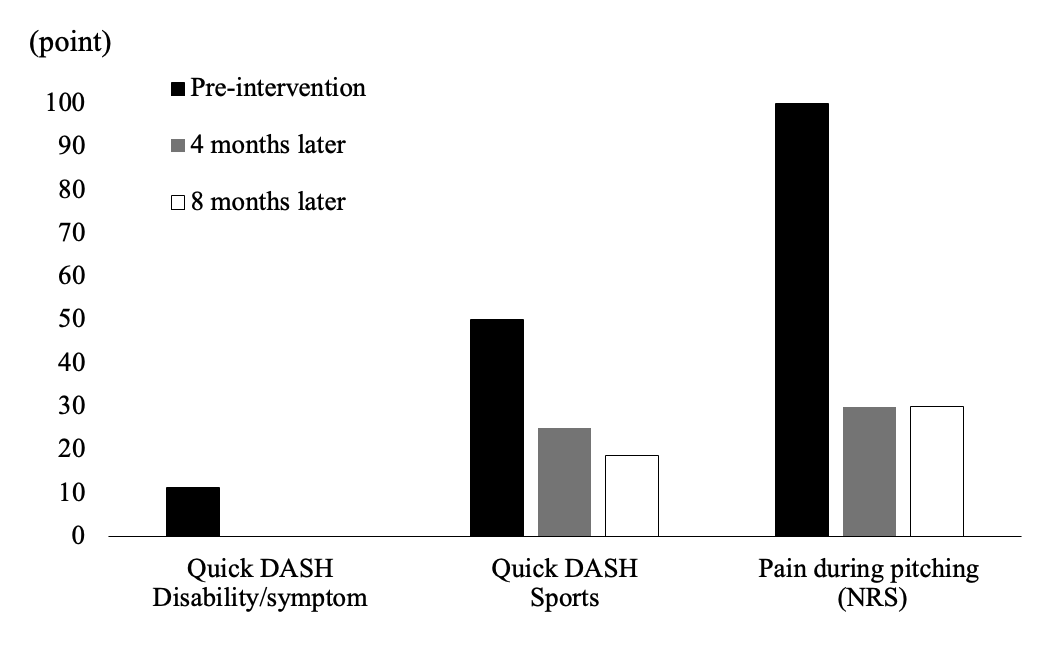
The initial examination revealed severe pain localized to the rotator cuff interval and posterior shoulder, elicited with palpation and during motion. Despite corticosteroid and local anesthetic injections into the rotator cuff interval, the pain during movement persisted. The subject’s active range of motion (ROM) was significantly restricted by pain, with abduction of 160°, external rotation of 30° in the neutral position, and external and internal rotations of 90° and 30°, respectively, at 90° abduction. Manual muscle testing (MMT), based on the Kendall scale (graded from 0 to 5), showed marked weakness across various shoulder movements, with muscle strength graded as 2/5 for external rotation in both the neutral and abducted positions, primarily limited by pain during the assessment (Figures 1A and B). The subject’s Quick-DASH scores were 11.4 for the disability/symptom, 0 for work, and 50/100 for sports, with a Numeric Rating Scale (NRS) pain score of 10/10 during pitching, 8–9/10 during external rotation, and 0/10 at rest.

Ultrasound Imaging
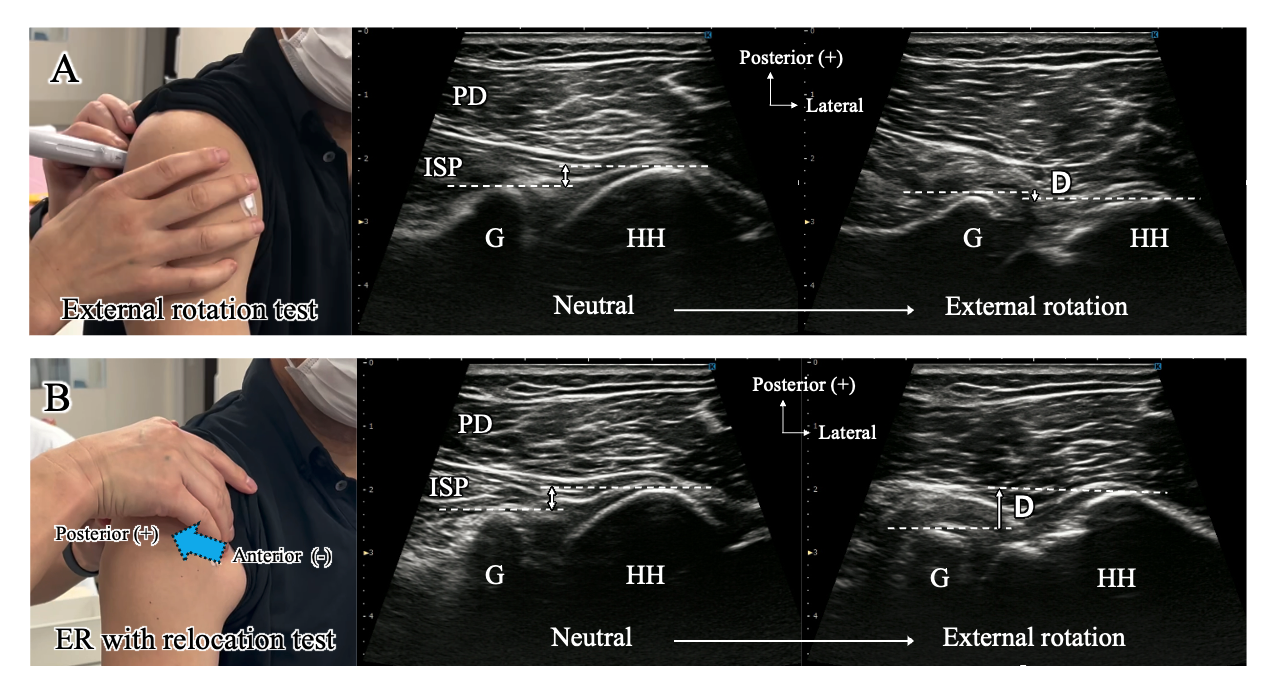
Musculoskeletal ultrasound imaging (SONIMAGE MX1 SNiBLE yb, KONICA MINOLTA, INC., Tokyo, Japan) confirmed a positive Doppler signal, indicating significant inflammation around Bennett’s lesion (Figure 1C). Ultrasound-guided palpation revealed tenderness, and dynamic ultrasound examination showed notable anterior subluxation of the humeral head at the end of external rotation, correlating with pain onset (Figure 2A). The relocation test reduced anterior translation, resulting in complete pain relief during external rotation (Figure 2B). Measurement using Image J software (NIH, Maryland, USA) indicated a 4.43-mm anterior shift of the humeral head from neutral to the end of external rotation, contrasted with a 2.31-mm posterior shift during the relocation test.

Therapeutic Intervention
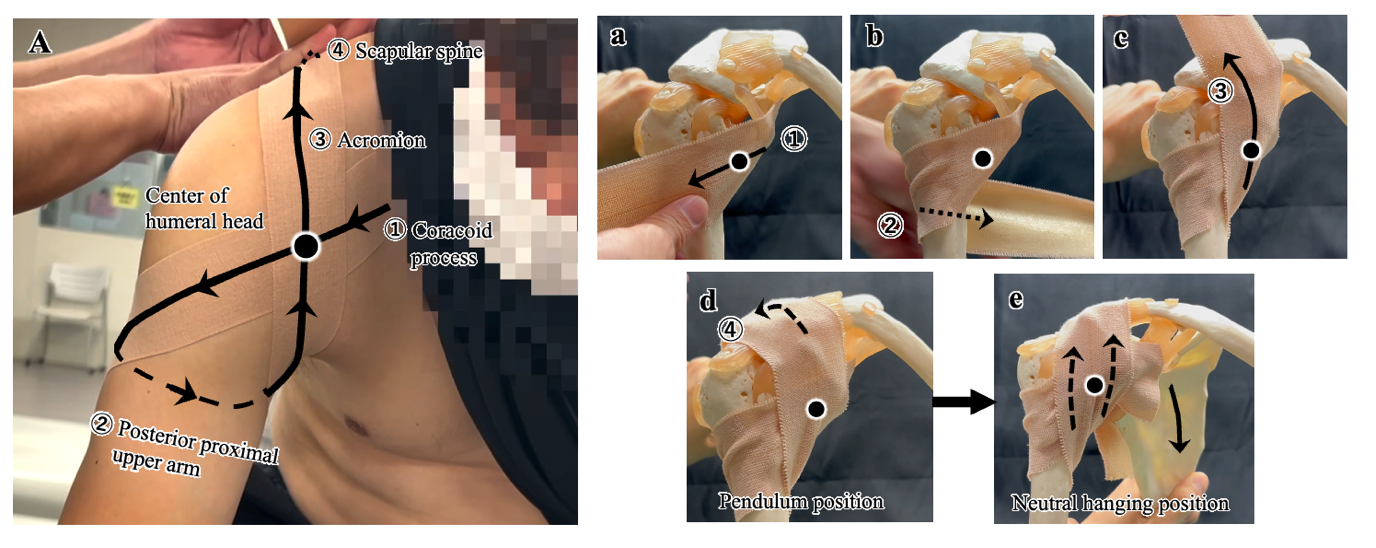
A novel figure-eight anterior stabilizing taping technique was applied using kinesiology tape (KILO TAPE, 5cm×5m KPB500, KG Inc, Tokyo, Japan) to control shoulder instability and maintain centripetal alignment (Figure 3A, supplementary video). The tape was stretched to 1.1–1.3 times its original length to achieve the desired tension. Two strips of tape were applied in an overlapping manner with a slight offset between them, while the subject maintains a forward-leaning trunk position with the arm hanging naturally downward. Specifically, the tape was first anchored at the coracoid process and applied over the anterior humeral head (Figure 3a). It was then directed horizontally across the posterior aspect of the humerus (Figure 3b), followed by cranial traction toward the anterior acromion (Figure 3c), and finally secured over the scapular spine (Figure 3d). Returning the arm from the pendulum position to the neutral position increased the tension of the cranially directed tape, thereby enhancing anterior stabilization of the glenohumeral joint (Figure 3e).
Additionally, a home exercise program was prescribed to promote stabilization of the glenohumeral joint and facilitate functional recovery. The exercises included unloaded active rotational movements in three planes, focusing on maintaining central positioning of the humeral head throughout the motion. Corrective movement patterns for throwing mechanics were also instructed to prevent excessive anterior translation of the shoulder. Continued adherence to these exercises as part of the home program was strongly recommended.
.png)
Outcome
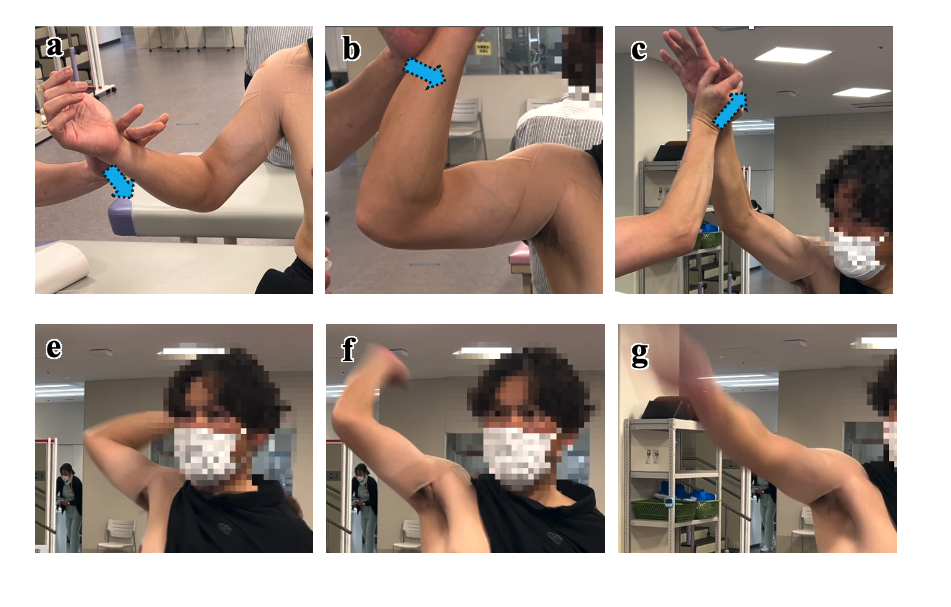
The subject demonstrated immediate improvement in neuromuscular control, allowing more effective activation of the shoulder muscles, particularly the rotator cuff. MMT showed improvements in external rotator strength from grade 2 to nearly grade 5 following the taping intervention, which was accompanied by a substantial reduction in pain, as reflected by a decrease in NRS scores to 1–3/10 during external rotation exertion and a pushing motion at the release position (Figures 4a–c). Notably, the subject regained functional movement patterns, and was able to perform shadow pitching without pain (Figures 4e–g) and to throw a tennis ball smoothly without any pain. Subjectively, the subject noted that taping provided critical anterior stabilization, which allowed the subject to regain the sensation of finger acceleration at the release point, which was an important aspect of his pitch mechanics (Figure 5a). The subject also became aware that prior to taping, anterior shoulder instability caused delays in the elbow and hand reaching the release point, which the taping positively affected (Figure 5b). With the tape in place, the subject reported restoration of unconscious fluid arm movement and a marked reduction in apprehension, which had previously hindered performance. Although the attached tape disrupted the ability to perform ultrasound imaging, making it difficult to confirm the reduction in anterior subluxation of the humeral head, marked functional improvements strongly suggest that taping effectively stabilized the shoulder joint. After returning home, the subject self-reported the ability to pitch from 18.44 meters at approximately 85% intensity while still wearing the tape, although this was not directly observed.


Follow-Up
Due to the subject’s geographical distance from the clinic, the intervention was limited to a single session. Four months later, via email, the subject reported a successful return to competitive pitching, achieving a maximum pitch speed of 115 km/h with minimal pain (NRS of 3/10 during pitching), based on self-reported measurements taken at the game venue (Figure 6). At that time, Quick-DASH scores were 0 for the disability/symptom, 0 for work, and 25/100 for sports. These changes reflect the disability/symptom and work components became completely asymptomatic, and the sports component decreased by 25 points from the initial examination, demonstrating significant improvement and surpassing the minimal clinically important difference (MCID: 19 for Quick-DASH score).9 The subject continued the prescribed home exercises, based on glenohumeral joint movements learned during the taping intervention, to maintain shoulder alignment and prevent pain recurrence. The subject also focused on correcting throwing mechanics, particularly by preventing excessive forward movement of the shoulder during the cocking phase, which facilitates smooth joint motion and reduces strain. The subject was confirmed to have received only the single session of taping treatment and exercise instruction, with no additional taping or clinical therapeutic interventions administered, although the home exercise program was continued independently by the subject.

The subject emphasized that the stabilization provided by the tape was instrumental in assisting him with correcting his pitching form. This sensation of stability reportedly helped with relearning a natural takeback motion, ultimately restored the original pitching technique. Notably, the positive effects of taping have persisted even eight months after the intervention, underscoring that a single intervention, combined with proper education, can lead to sustained recovery and enable long-term sports participation. The subject continued to practice recreational pitching and maintained a consistent exercise regimen, further enhancing overall quality of life. Quick-DASH scores were 0 for the disability/symptom, 0 for work, and 18.8/100 for sports.
DISCUSSION
This case demonstrates that a novel figure-eight taping technique provided immediate and sustained pain relief in an individual with anterior shoulder instability. Rapid improvement in dynamic shoulder stability facilitated the ability to relearn pain-free throwing mechanics, which was crucial for successful return to competitive sports.
The key strength of this approach is its non-invasive and straightforward application, which offers an effective method to provide feedback and likely enhance neuromuscular control, thereby potentially influencing anterior shoulder instability and simultaneously reducing pain. This is particularly valuable for overhead athletes where conservative treatments often fail to fully address shoulder instability, particularly in advanced cases of rotator cuff dysfunction.1 While labral repair and rotator cuff interval closures are considered definitive treatments, they require extended recovery periods and carry risks such as complications or a limiting the ROM required for athletic activities such as pitching.6 Although the use of adjunctive taping to enhance glenohumeral joint stability and reduce pain has been demonstrated in some studies, its efficacy is limited.10 In this case, the taping intervention did not restrict ROM but rather facilitated comfortable movement for the subject. Although the primary target of the taping was the glenohumeral joint, it may have exerted secondarily effects on scapular positioning. Given the established link between scapular alignment and humeral head centering,4 such indirect effects could have further contributed to overall shoulder stability. This mechanism likely supported the subject’s improved hand velocity up to the point of ball release. Moreover, the single intervention had a significant educational impact, enabling the subject to develop an awareness of proper joint mechanics without direct coaching on pitching motion.11 This experience may have served as a catalyst for long-term motor learning, facilitating the subject to naturally internalize and adopt physiological joint movements.
Conventional physical therapy interventions—such as rotator cuff strengthening exercises and joint range-of-motion training—often reported to be less effective in subjects with significant joint instability compared to individuals without structural instability.2 While this taping intervention may not be suitable for cases clearly indicated for surgery, it could offer a valuable treatment option for subjects on the borderline between surgical and conservative therapies, or for those who have not responded to standard conservative treatments. Therefore, this taping technique has the potential to serve as a novel intervention to bridge the gap between conservative and surgical interventions.
Limitation
This case report has limitations, notably, the follow-up results were based on self-reported outcomes rather than ongoing clinical assessments, which may introduce potential bias. Additionally, the absence of a control group or comparison with other conservative treatments limits the generalizability of these findings. The taping technique described may also be applicable only to individuals with characteristics similar to the athlete in this case. As the case report methodology does not establish cause-and-effect relationships, these results should be interpreted with caution. Future studies should evaluate the long-term efficacy and broader applicability of this taping method in larger, more diverse populations through randomized controlled trials or comparative studies.
CONCLUSION
The figure-eight taping technique provided a viable, non-invasive option for managing anterior shoulder instability in this subject, offering immediate pain relief and supporting the recovery of functional throwing mechanics. In this case, a single taping intervention combined with education enabled the subject’s long-term return to throwing and significantly improved the quality of life of this subject.
Corresponding author
Masashi Kawabata, PT, PhD
ORCID: 0000-0001-8722-7117
Department of Rehabilitation, Kitasato University School of Allied Health Sciences.
1-15-1 Kitazato, Minami-ku, Sagamihara-shi, Kanagawa 252-0373, Japan
Phone: +81 42-778-9968
Fax: +81 42-778-9968
E-mail: mkawaba@kitasato-u.ac.jp
Conflict of Interest
The authors report no conflicts of interest.