
INTRODUCTION
Hamstring strain injury (HSI) is a common injury associated with various sports,1,2 with severe HSI often requiring greater than two months to return to play (RTP).3 Frequently, it occurs in activities involving explosive lower extremity movements, such as high-speed sprinting,4 and is a particularly significant problem in track and field events. The highest incidence of HSI is observed in international track and field competitions, excluding the long-distance events.5 Furthermore, a survey of track and field athletes competing in the European Athletics Championships reported that 48% of them have experienced HSIs throughout their careers.6 HSI is the leading acute injury among young and junior athletes.7 In addition, HSI is an injury with a high recurrence rate.8 In other words, HSI is highly prevalent within track and field, and young athletes should address the risk of HSI in their early competitive careers.
Several previous studies investigated various methods of reducing the risk of HSI. In recent years, the Nordic hamstring exercise (NHE) has been recommended as part of an HSI prevention program, along with warm-up, stretching, stability training, strengthening, and functional movements (sport-specific, agility, and high-speed running).4 The NHE is an exercise focused on eccentric contractions of the hamstrings,9 and strong evidence has been reported to reduce the risk of HSI.10 However, the NHE has the following disadvantages: 1) delayed-onset muscle soreness and knee joint pain after the NHE,11 2) decreased hamstring electromyography (EMG) amplitudes and eccentric torque after performing the NHE,12 and 3) declined sprinting performance after the NHE.13 These factors lead to low NHE compliance,14 and interventions with poor compliance do not reduce the HSI risk.15,16 In addition, youth athletes with long playing histories have lower compliance with prevention programs,17 so earlier intervention is required. However, injury prevention strategies for youth athletes have focused on passive strategies such as rule and environmental adjustments, and there is limited evidence for strategies that rely on behavioral change in athletes.18 Furthermore, youth athletes have low compliance with prevention programs that are athlete-led and do not have the support of coaches.19 With this background, methods other than the NHE should be considered to reduce the risk of HSI in youth track and field athletes.
Therefore, this study focused on the Single-leg Romanian Deadlift (SLRDL), a single-leg exercise that generates greater hamstring muscle activity than the double-leg deadlift20 and, like the NHE, promotes an eccentric hamstring contraction.21 Furthermore, the SLRDL is advantageous because it is easy to perform without requiring partners or equipment like NHE. Furthermore, unilateral exercise is an effective warm-up exercise because sprinting is a movement with repeated take-off for each leg.22
A previous study reported that the SLRDL performed during warm-up can counteract the increase in the stiffness of the hamstring muscle and decrease in eccentric muscle strength caused by sprint training.23 Furthermore, it is known as a common track and field warm-up exercise.24 For these reasons, the SLRDL could easily be implemented as a prevention program for HSI in the track and field. However, whether SLRDL can reduce the risk of HSI remains unclear. To address this question, this study aimed to examine the effect of the SLRDL on the risk of HSI. The hypothesis was that the SLRDL compliance would be high and that the SLRDL can reduce the risk of HSI.
MATERIALS AND METHODS
Study Design
This cohort study of high school track and field athletes was conducted by the same staff (coach and athletic trainer) over two seasons: the control season (January 1, 2022 to December 31, 2022) and the intervention season (January 1, 2023 to December 31, 2023). During the intervention season, the SLRDL was added to the warm-up, and the annual competition schedule did not differ from the control season. An athletic trainer who was a certified strength and conditioning specialist and physical therapist instructed the athletes in the SLRDL and recorded the incidence of HSI and time to RTP. At the end of the intervention season, the athletes were given a questionnaire regarding the SLRDL implementation (Figure 1).

Subjects
The participants were high school athletes on the track and field team. Athletes with a history of HSI were excluded. Daily training mainly comprised sprint training. The athletes had strength and conditioning sessions once or twice a week throughout the season. The sessions consisted of squats, bench presses, and Olympic weightlifting (snatch) at 70-90% of the one repetition maximum, and plyometric training. There were no major changes to the annual competition schedule or training program between the two seasons. This study was conducted in compliance with the Declaration of Helsinki and received approval from the ethics committee of the author’s affiliated institution. If the participant was under 18 years of age, the subject and parent received an explanation, including the risks of the study, before participating in the testing. Written informed consent was obtained and signed by all participants (and a parent if appropriate).
Preparatory lecture
Lectures were given to athletes and coaches on the effectiveness of eccentric exercises in reducing the risk of HSI and how to perform SLRDL before starting the SLRDL intervention.
Warm-up protocol
During the control season, athletes performed a warm-up routine before practices and competitions with the following activities: 1) jog, 2) static stretch, 3) dynamic stretch, 4) sprint drill, and 5) short dash. The detailed menu within each session was adjusted for each athlete. The athletes spent about 30 min during the warm-up before moving on to practice and competitions in specialized events. In the intervention season, the same warm-up program was implemented, but the SLRDL was additionally implemented at any time during the dynamic stretch.
Single-leg Romanian Deadlift
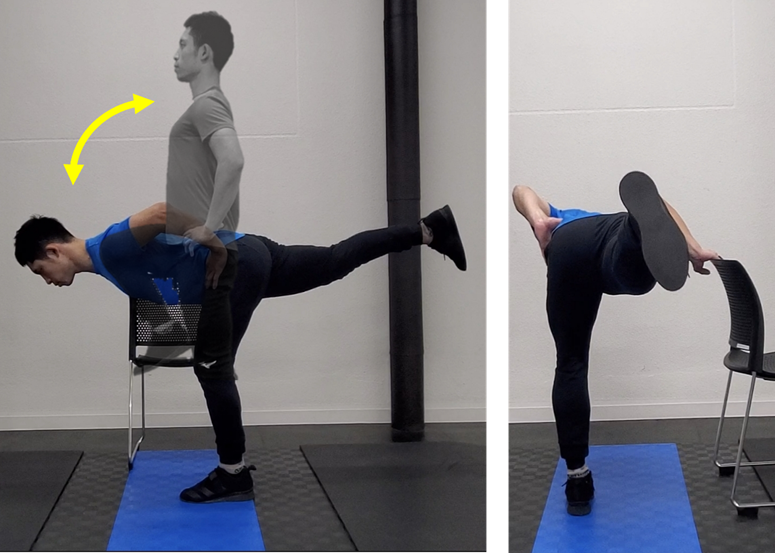
The SLRDL was performed following the methods of Weaver and Kerksick25 and McCunn et al.26 To begin, the athlete stood on one leg with the core stabilized. In the descending phase, the knee joint of the loaded leg was slightly flexed, and the hip joint flexed while keeping the spine neutral. The hip and knee joints of the unloaded leg are maintained in extension, and the body is tilted so that the spine is parallel to the floor as much as possible. The distance of the athlete’s movement depends on the athlete’s flexibility of the hamstrings. Once the lowest point of the movement was reached, the athlete returned to the start position while contracting the hamstrings and gluteus maximus muscles. The athlete maintained balance by placing the hand opposite of the load leg on a wall or handrail to stabilize the movement (Figure 2). The athletic trainer instructed the athletes to avoid spinal movement, hip rotation, and abduction of the loading leg during the SLRDL. With reference to previous research,23 The athletes were instructed to perform SLRDL for three sets of three repetitions on each leg per warm-up session. The coaches and athletic trainers checked to ensure that the athletes were performing the SLRDL, but did not check or record how many repetitions they performed.
.png)
HSI surveillance
The athletic trainer recorded the instances of HSI that occurred throughout the seasons. The trainer recorded the athlete hours (AH) to determine the athlete’s activity. AH were calculated as the number of practice or competition days multiplied by the number of athletes participating on that day and the number of activity hours. Based on the study by Chebbi et al.,27 HSI was defined as acute (sudden-onset injury) pain in the posterior thigh that occurred during practice or competition and resulted in immediate termination of play and inability to participate in the next practice or competition. Injured athletes underwent clinical examination by an orthopedic surgeon and, if necessary, magnetic resonance imaging or ultrasonography was performed. Furthermore, the time to RTP following HSI injury was recorded. The RTP criterion was defined as the time to return to full training (TRFT), i.e., the time that confirmed the ability to complete in unrestricted training sprint efforts at full pace in spikes.3 Rehabilitation after HSI was based on a report from British Athletics.28 In this protocol, the average TRFT for severe HSI with intratendinous injury was 48 days. However, this previous study did not find any significant differences in TRFT for other HSI types. Therefore, this study combined mild and moderate HSI. Based on the above, HSI with a TRFT of 1–47 days was classified as mild to moderate, and those with a TRFT of ≥48 days were classified as severe.
Questionnaire
After completing the intervention season, questionnaires were sent to the athletes to gather their feedback. The questionnaire was administered after explaining that it was not related to the selection of athletes for competitions. The athletes were then asked to indicate their compliance with the SLRDL exercise during practices and competitions throughout the year and to indicate the frequency of SLRDL performance from 0 to 7 days per week.
Statistical Analyses
Data were analyzed using SPSS version 22.0 (IBM Corporation, New York, NY). The initial analysis of injury incidence was calculated by dividing the total number of HSIs by the exposure time and reported as injury rates per 1,000 AHs. An unpaired t-test and a chi-square test were conducted for the comparison of the athletes at baseline. In addition, pre- and post-intervention risk ratios (RR) were obtained for each severity of HSI (mild to moderate, severe, total). To control for the overall Type I error rate, data were tested in a prespecified hierarchical order, with a significance level of 5%. After the survey, a post-hoc power analysis was conducted using G*Power version 3.1.9.6 (Heinrich Heine University Düsseldorf, Germany).
RESULTS
In total, 77 athletes from one high school track and field team participated in the study: 40 from the control season (21 men; 19 women, aged 16.8 ± 0.9 years) and 37 from the intervention season (16 men; 21 women, aged 17.0 ± 0.7 years). Twenty-eight athletes (14 men; 14 women, aged 17.3 ± 0.5 years) were carried over from the control season to the intervention season, with 12 graduating and nine enrolling. These athletes specialized in short-distance running, jumping, and combined events (excluding long-distance running), and the percentages of each were 75.0%, 17.5%, and 7.5% in the control season and 70.3%, 21.6%, and 8.1% in the intervention season, respectively.
No significant differences were found in the baseline information. In the control season, 15 HSIs occurred in 25,011 AH, and in the intervention season, eight HSIs occurred in 26,445 AH; the risk of HSI per 1,000 AHs was 0.60 and 0.30 in the control and intervention seasons, respectively. Data for each season are shown in Table 1. The results demonstrated that the risk of mild to moderate HSI severity was significantly reduced postintervention, with a RR of 0.34 (95% confidence interval [CI]: 0.12–0.94). However, change in the risk of severe HIS in the intervention was not statistically significant, with a risk ratio of 2.84 (95% CI: 0.30–27.28) (Table 2). The post-hoc power analysis indicated power of 0.903. The questionnaire revealed that the frequency of the SLRDL was 5.92 exercise sessions (± 0.28) per week. Compliance was 98.67%, given that practice or competition sessions were six times/week.
DISCUSSION
This study investigated whether adding the SLRDL exercise to the warm-up routine could reduce the risk of HSI incidence in high school track and field athletes. The findings revealed that the addition of the SLRDL could reduce the risk of mild to moderate HSI, despite the absence of a significant effect for reducing the risk of severe HSI. Furthermore, SLRDL showed high compliance. To the best of the authors’ knowledge, this is the first study that examines the efficacy and compliance of the SLRDL as an intervention in reducing the risk of HSI.
The mechanism of HSI risk reduction using the SLRDL must be considered. Low hamstring eccentric force and short muscle fiber length have been associated with a high risk of HSI.29 Eccentric training of the hamstrings has been shown to increase the hamstring eccentric muscle strength and muscle fiber length,30 a mechanism by which eccentric training can reduce the risk of HSI. SLRDL is an exercise that generates eccentric contractions in the hamstrings21 and may reduce the risk of HSI for the same reason. In addition, Schuermans et al.31 measured EMG during sprinting at the beginning of the season in soccer players and reported that players who suffered an HSI during the season had less EMG activity in the gluteus maximus muscle than those who did not. Therefore, increasing the activity of the gluteus maximus may reduce the risk of HSI. The SLRDL is an exercise that promotes high muscle activity in the gluteus maximus muscle in addition to the hamstrings.32 Considering a physiological response called “resistance priming,” a temporary increase in muscle strength following resistance training,33 use of the SLRDL during warm-up may increase the activity of the gluteus maximus muscle and reduce the risk of HSI. Furthermore, it has been reported that the SLRDL during warm-up can inhibit the decline in hamstring muscle strength caused by repetitive sprints23; thus, the SLRDL may also activate the hamstrings. In conclusion, the SLRDL was able to reduce the risk of mild HSI. Possible long-term mechanisms may include structural changes and improvement in eccentric strength in the hamstrings, and short-term mechanisms may be activation of the hamstrings and gluteus maximus during sprint. However, none of these specific outcomes were not investigated in this study.
Clearly, higher compliance with preventive interventions increases the effectiveness of HSI risk reduction. Ripley et al.,16 in a systematic review of studies on the reduction of HSI risk with hamstring eccentric exercises, reported a reduced risk of HSI when exercises were performed with a compliance >50.1%. The compliance rate in this study was 98.67%, which is sufficiently high for an intervention to be effective. Regarding compliance with interventions to reduce the risk of HSI, van der Horst et al.14 reported the importance of factors such as athletes’ knowledge and consensus among the team staff as necessary factors to increase adherence. In this study, the athletes and coaches were provided information about hamstring eccentric training in reducing the risk of HSI, and consensus was obtained before the intervention was implemented. Therefore, the SLRDL intervention in this study is believed to maintain high compliance. According to van der Horst et al.14 time consumption was also identified as a factor influencing compliance. Compared with NHE, which requires a partner and equipment, the SLRDL is an exercise that can be easily performed by the athlete alone. Furthermore, the volume of SLRDL per session in this study was small, with only three sets of three repetitions. Therefore, the compliance with the SLRDL in this study is considered high, likely because of its low time consumption.
Although NHE has been shown to reduce the risk of HSI regardless of severity,34 the current study revealed no preventive effect of the SLRDL on HSI of higher severity. A study reported that the NHE has the capacity to increase eccentric muscle strength and muscle fiber length, regardless of training volume.35 Moreover, a significant increase in muscle strength and fiber length was observed with increased intensity of the NHE.36 Thus, the intensity of eccentric training may be important in reducing the risk of HSI. Compared with the NHE, the SLRDL has lesser intensity with less generated muscle force in the hamstrings.21 Furthermore, this study investigated the SLRDL performed using a body weight load, and the intensity was therefore inconsistent among athletes. Consequently, the SLRDL intervention in this study may not have been effective in reducing the risk of severe HSI because of its low intensity.
This study has some limitations. The present study design is the similar design used in previous studies.27,37 However, this research design is an observational study, and the athletes were not randomly selected for the study. While this approach reflects the reality of athletes in a clinical setting, it is essential to note that various factors that could affect the results of the study have not been considered. Some athletes underwent a control season and an intervention season consecutively, but separating athletes with and without intervention within the same team at the same time could create a sense of inequality, making it an unrealistic approach. Furthermore, it is important to mention that at the end of any season, some senior athletes leave the team, while new athletes join. Thus, it seems that there are no substantial changes in the overall age range or training history of the team. In the future, the authors would like to increase the number of subjects and conduct analyses with the intervention period matched. Second, further research is needed to verify whether the SLRDL causes structural and strength changes in the hamstrings to validate the mechanisms discussed. Third, the effect of resistance priming in the warm-up routine is influenced by the strength level and training history.38,39 However, this study could not examine the strength level and training history of each athlete. Furthermore, HSI is an injury that more frequently occurs in senior athletes than in junior athletes6,7; future research should be conducted on various categories of athletes to examine the effects of muscle strength level and training history. Finally, there are potential concerns about the results because this the training volume of the SLRDL was not strictly controlled. It is possible that the SLRDL may also have a risk reducing effect on HSI, just like NHE,35 regardless of the training volume. A future study could investigate the relationship between the training volume of the SLRDL and the risk reducing effect on HSI.
CONCLUSION
In this study, introducing SLRDL to warm-up for high school track and field athletes reduced the risk of mild to moderate HIS, and compliance was high. Despite its advantages in compliance, the lower intensity of SLRDL compared with NHE might limit its effectiveness in reducing the risk of severe HSI. However, further research is recommended to optimize HSI prevention programs, using SLRDL as an introductory measure rather than a complete alternative to NHE.
Corresponding Author
Ryo Otani
Department of Rehabilitation Medicine, Nishikawa Orthopedic Clinic, 2171-5 Mikatsukicho-chokanda, Ogi, Saga, 845-0021, Japan
Telephone: +81-90-5688-4468
E-mail: otani.mail@gmail.com
Disclosure of interest
The authors report no conflicts of interest.