

INTRODUCTION
Cervical radiculopathy is characterized by the compression or irritation of a spinal nerve root, often due to disc herniations, intraneural edema, arthritic bone spurs, spondylosis or degenerative disc disease and can lead to significant neck and/or arm pain and disability.1,2 It is a commonly encountered condition with an estimated annual incidence of 107.3 per 100,000 for men and 63.5 per 100,000 for women.3 Conservative management involves physical therapy (PT), oral medications, and epidural steroid injections, however, if symptoms do not improve or there is progressive neurological deficit, surgery is often the next recommended treatment choice.4–8 Anterior cervical discectomy and fusion (ACDF) has been shown to be effective for symptom relief of cervical radiculopathy; however, there is concern for loss of cervical range of motion (ROM) and adjacent segment disease (ASD).2,4–8 To address this limitation, cervical total disc replacement (CTDR) was developed to similarly decompress nervous structures while promoting normal spinal biomechanics and reducing postoperative complications such as ASD, pseudarthrosis, or fracture.2,4,6,9 Since initial approval for use by the Food and Drug Administration (FDA) in 2007, CTDR has demonstrated noninferiority to ACDF and has become a popular treatment option by spine surgeons.10 Despite the increased use of CTDR in the management of cervical radiculopathy, there is no published literature regarding postoperative management, specifically the optimal content, timing and duration of postoperative PT for CTDR.10–18 Therefore, the purpose of this case report is to describe the postoperative PT management and one-year outcomes of a Brazilian Jiu Jitsu (BJJ) athlete after CTDR as it relates to pain, function, return to play, and quality of life.
CASE DESCRIPTION
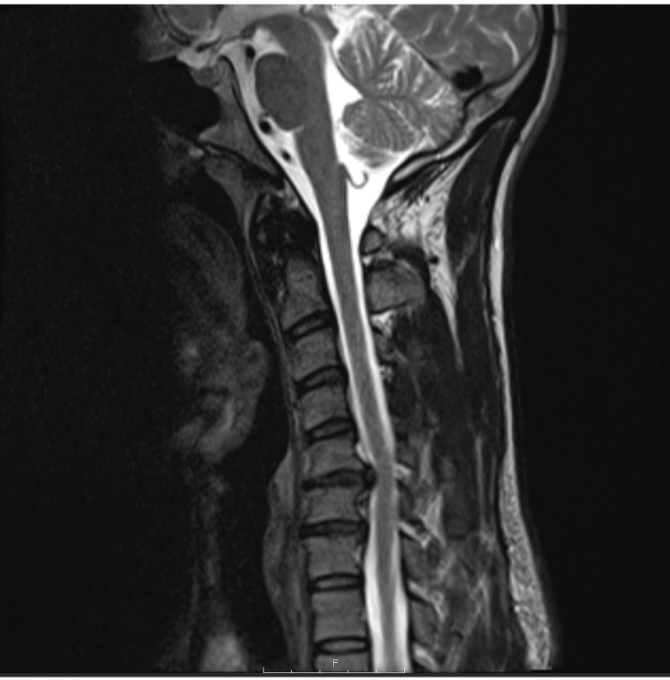
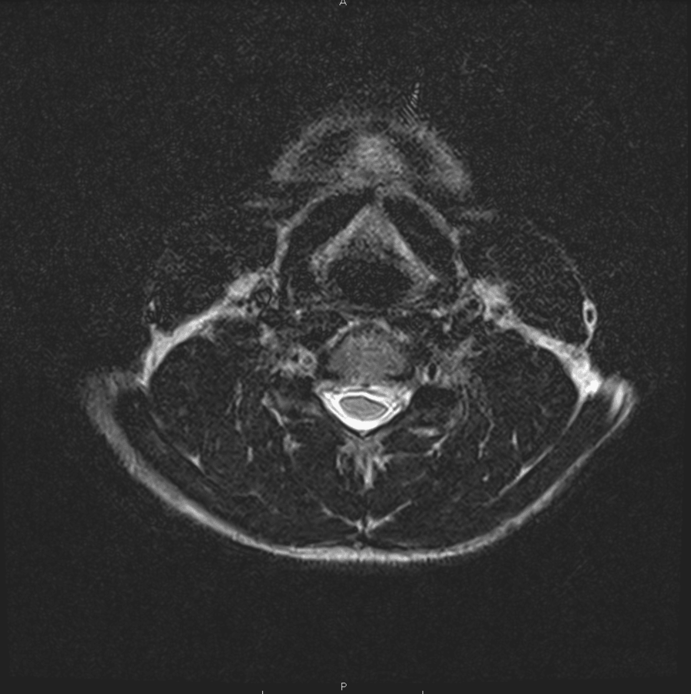
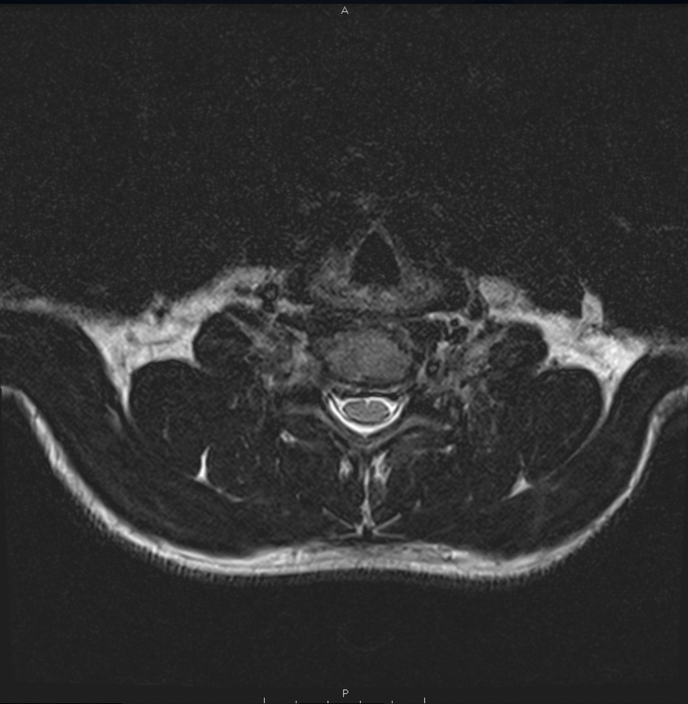
A 37-year-old male BJJ athlete developed left sided neck, shoulder and arm pain following a deadlifting injury five months prior. Initial management included physical therapy at an outside institution which yielded mild symptom improvement. One month later, the subject returned to BJJ, however, symptoms recurred more severely, and physical therapy interventions were no longer effective. Due to increased pain with limited symptom control, the subject sought consultation from an orthopedic spine surgeon. Magnetic resonance imaging (MRI) was performed noting C5-C6 herniated nucleus pulposus, with C5-C6, and C6-C7 cervical spondylitic radiculopathy (Figures 1-3). The subject was provided a tapered methylprednisolone pack for pain control and recommended to undergo C5-C6 and C6-C7 discectomy with Mobi-CTDR. Prior to surgery, the subject wanted to establish care with a spine physical therapist and underwent a preoperative physical therapy initial consultation.



Preoperative Physical Therapy
Initial Consultation
The subject presented to outpatient physical therapy with complaints of pain located on the left-sided cervical spine with left upper extremity weakness and paresthesia noted in the anterolateral shoulder. The subject presented with 2/10 neck and arm pain which ranged from 0/10 to 10/10 Numeric Pain Rating Scale (NPRS) intermittently with aggravating movements. Aggravating factors included cervical extension and rotation to the left with local pain and reproduction of paresthesia in left arm. Relieving factors included neutral spine posture and cervical flexion. The subject reported no stiffness or pain in the mornings, intermittently worse with activity, and pain at night that was relieved with position change during sleep. He denied right upper extremity paresthesia or weakness, bilateral lower extremity symptoms, bowel/bladder dysfunction, gait instability, fine motor hand coordination changes, fevers, chills, night sweats, nausea, vomiting, or personal history of cancer. Past medical and surgical history included right anterior cruciate ligament reconstruction, depression, anxiety, and bipolar disorder. The subject denied previous cervical pain, injections or surgeries to the spine. Medications included ibuprofen, mirtazapine, levothyroxine, fluvoxamine, quetiapine. The subject’s goals were to return to a prior level of activity including unrestricted BJJ, bouldering, and weightlifting, which were all activities that he was unable to participate in at the time. Physical examination included cardiopulmonary, integumentary, neurologic and musculoskeletal assessments (Table 1). Remarkable neurologic findings included left C6 myotome weakness, decreased deep tendon reflex (DTR), and diminished dermatomal static mechanical cutaneous sensation. Remarkable musculoskeletal findings included local left-sided neck pain and peripheralization to left upper extremity (LUE) with cervical extension, left lateral flexion, and left rotation, and positive cervical extension quadrant and Spurling’s tests with reproduction of local left-sided neck pain and LUE peripheralization.
Operative Procedure
Preoperative impression was reported as C5-C6, C6-C7 cervical spondylitic radiculopathy, and C5-C6 herniated nucleus pulposus. Patient underwent C5-C6, C6-C7 anterior cervical radical discectomy and central spinal cord decompression, bilateral foraminotomies, and placement of an artificial disc replacement (Mobi-C), Orthofix M6 6x17x16 x2, utilizing microsurgical techniques. Fluoroscopy and multimodal neuromonitoring were utilized for interpretation of the procedure. Incisions were performed through platysma, superior edge of omohyoid fascia, reflecting medially with the strap muscles, trachea and esophagus and lateralized the neurovascular bundle and sternocleidomastoid. Findings included multi-fragmented, large, extruded nucleus pulposus sitting in the left lateral gutter of nerve root and spinal cord, with advanced degenerative changes of the disc space noted. The incised C5-C6 disc reached back to the posterior longitudinal ligament which had been grossly compromised with large left paracentral disc extrusion causing high-grade thecal sac and neural foraminal compression. Multiple fragments were removed as part of the decompression at C5-C6 and C6-C7 levels. Orthofix M6 implants were placed under direct visualization and radiographic confirmation. The patient experienced no intraoperative surgical or anesthetic complications.
Postoperative Physical Therapy
Initial Consultation
Two weeks following the C5-C6 and C6-C7 discectomy with Mobi-CTDR, the subject presented to postoperative physical therapy with significant pain relief, however, he still demonstrated cervical active range of motion (AROM) deficits and neck and arm weakness which limited him from performing daily activities and participating in BJJ. At initial consultation, he still had 2/10 neck pain, however, his arm pain was rated a 0/10. Aggravating factors included cervical lateral flexion bilaterally. Relieving factors included maintaining neutral head posture and supporting both arms in sitting. He denied right upper extremity paresthesia or weakness, bilateral lower extremity symptoms, bowel/bladder dysfunction, gait instability, fine motor hand coordination changes, fevers, chills, night sweats, nausea, vomiting, dysphagia, dysarthria, chest pain, shortness of breath, resting or night pain, or edema into bilateral extremities. The subject’s primary goal for recovery was to return to a prior level of function by participating in BJJ and weightlifting at the gym as soon as safely possible. Follow-up physical examination included cardiopulmonary, integumentary, neurologic and musculoskeletal assessments (Table 2). Integumentary screen revealed signs of well healing incisions non-tender to touch and without erythema, drainage, or foul odors present. Neurological examination revealed unchanged left C6 myotome weakness, however, he demonstrated improvements compared to preoperative status in light touch sensation in left C6 dermatomal pattern and DTR. Musculoskeletal examination revealed pain-free cervical extension and rotation, and with painful but improved cervical lateral flexion AROM bilaterally.
Postoperative Rehabilitation
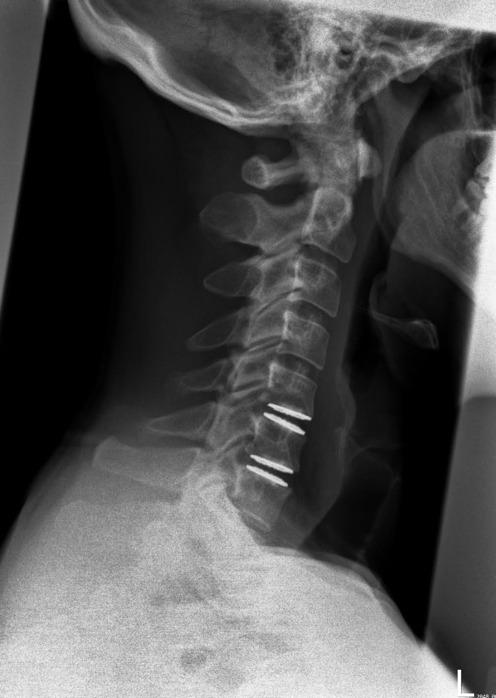
The subject was seen in PT for 14 sessions spanning 16 weeks. The initial evaluation session was one hour long and follow up sessions were 30 minutes in length. PT interventions included manual therapy (soft tissue and joint mobilization), therapeutic exercise (targeting cervical spine, thoracic spine and upper extremity to address mobility and strength), and weightlifting body mechanics education. Radiographic confirmation of prosthesis placement and healing was monitored at postoperative weeks six and 12 (Figures 4-5).
The PT program was designed, progressed, and tailored to the individual according to patient related factors, surgical related factors, and the available evidence for rehabilitation after cervical spine surgery.1,6,8,11–18 Patient-specific factors included past medical history, social history, body structure and function impairments, activity limitations, participation restrictions, personal goals and sport-specific demands. Surgical factors included the surgery date, multi-level involvement, type of implant utilization, timeline of symptoms, bone, implant and soft tissue healing timelines, and postoperative cervical spinal restrictions.1,6,8,11–19 Intervention selection was influenced by limited evidence on PT postoperative management of cervical spine surgery and extrapolated from studies demonstrating safe and effective rehabilitation after other types of cervical spine surgery.1,6,8,11–18

The program was separated into four phases based on tissue healing timelines: inflammatory, proliferative, remodeling and maturation phases. Clinical and objective milestones were utilized as guides for the subject’s progression through each phase (Appendix A).
The goal of the inflammatory phase (Weeks 0-2) was to promote tissue healing, preserve the integrity of the operation, aid in subject’s symptom control and prevent postoperative complications. While there are no established evidence-based postoperative restrictions after CTDR, the operating surgeon recommended the subject to wear a cervical soft collar 24 hours a day (except to shower) for the first week and to avoid driving on pain medication (narcotics), aggressive activities such as high-level exercise, swimming, sexual intercourse, and work activity (depending on occupation) for two weeks after surgery. Furthermore, the surgeon recommended no pushing/pulling/lifting/overhead reaching more than 25 lbs for the first six weeks to limit complications to the surgical site. AROM of the head was allowed in all planes of cervical motion with pain as a guide, however, he was advised to avoid aggressive extension as not to disrupt surgical wound healing on anterior cervical musculature. PT education and counseling was given regarding inflammation, infection and wound care management. The subject was also counseled on posture training and how to wean from the cervical collar to avoid exacerbation of symptoms. Therapeutic exercise included a graded aerobic exercise program consisting of walking at self-selected pace up to 30 minutes per day to increase cardiovascular health and avoid postoperative complications such as venous thromboembolism. Manual therapy included gentle soft tissue mobilization (STM) to bilateral levator scapulae and upper trapezius musculature as well as scar tissue mobilization for pain relief and complaints of scar tension. Scar tissue mobilization was initiated 14 days postoperatively to allow for primary wound closure and was initiated only when there were no signs of infection, bleeding, wound dehiscence, graft failure or discomfort.20 No cervical spine ROM or strengthening was performed in this phase aside from activities of daily living (ADLs) due to implant-bone healing.
The goal of the proliferative phase (Weeks 3-6) was to promote thoracic spine and shoulder flexibility, initiate thoracic spine and arm strengthening, and continue to aid in subject’s symptom control. Previous interventions were utilized as needed. Manual therapy consisted of STM, scar tissue mobilization and accessory joint mobilization. STM was performed to the upper trapezius and levator scapulae and the subject was instructed how to perform this at home using a Theracane (Theracane, Theracane®, Denver, CO) to aid in resolution of pain and tightness. Scar tissue mobilization was utilized as needed. Accessory joint mobilization consisted of non-thrust central posterior-anterior (CPA) mobilization to the thoracic spine (T1-12). Therapeutic exercise consisted of shoulder mobility, thoracic mobility and thoracic spine and arm strengthening. Shoulder mobility was initiated in supine with active assisted range of motion (AAROM) in shoulder flexion, abduction, ER, IR and progressed as tolerated to standing AROM in all the same planes if there was no reproduction of pain or symptoms in the arm. Thoracic mobility was achieved with pectoralis stretching, active thoracic extension using a foam roll or chair/towel roll, active quadruped thoracic flexion/extension (cat/cow) and sidelying thoracic rotation on the floor. Thoracic spine and arm strengthening were achieved with scapular retractions, mid trapezius and low trapezius rows using elastic resistance bands. No cervical spine ROM or strengthening was performed in this phase aside from ADLs due to implant-bone healing.19,21–24
The goal of the remodeling phase (Weeks 6-10) was to restore full cervical ROM and initiate and progress cervical, thoracic spine and shoulder muscle strength for general fitness and daily function. Previous interventions were utilized as needed. Cervical ROM and strengthening were initiated when radiographs demonstrated no evidence of prosthesis malpositioning, displacement, subsidence or heterotopic ossification at six weeks.19,22–24 Therapeutic exercise consisted of cervical muscle strengthening, thoracic spine, shoulder, and arm strengthening. Initial cervical muscle strengthening was accomplished with deep cervical flexor (progressed supine to sitting) and extensor (progressed supine to quadruped) strengthening and cervical isometrics in all planes. Once these were performed without reproduction of pain or symptoms in neck or arm, strengthening was then progressed to incline and supine head lifts recruiting deep and superficial musculature as well as seated cervical isometrics using elastic resistance bands. If tolerated, cervical strengthening was advanced to use the Neckslevel (Neckslevel GlidePro NecksLevel, Inc. North Wales, PA) device at various angles, movements and intensities. Cervical ROM was accomplished in quadruped or flexion, extension and rotation bilaterally. Thoracic spine, shoulder and arm strengthening were accomplished with shoulder isometrics, resistance exercise using elastic resistance band for shoulder external rotation, internal rotation, and scapular plane abduction. Body weight exercises were incorporated with assisted pull-ups and push up progression (progressed from wall to table to knees to feet). Manual therapy consisted of STM to upper trapezius and levator scapulae and non-thrust accessory joint mobilization consisting of CPA and left and right unilateral posterior-anterior (UPA) grade IV mobilization to C4 and T1 for symptom control and improved rotation.
The goal of the maturation phase (Weeks 12+) was to progress overall fitness, strength, and endurance for gradual return to sport (RTS) without pain, symptoms, or consequence post-surgery. Previous interventions were utilized as needed. Therapeutic exercise consisted of cervical, thoracic spine, arm, and leg strengthening. Cervical strengthening was progressed to maximum resistance for cervical rotation and flexion as this was important to the subject for BJJ sparring and protection of his neck. At this time, the subject began to gradually return to BJJ practice with non-contact exercise and noted full body deficits in strength and conditioning. To improve overall strength and conditioning for practice, a weight training program was created that incorporated full body single and multi-joint movements, as well as body weight exercise such as pull-ups and push-ups without assist. As the subject tolerated the program, he was progressed into full contact BJJ.
OUTCOME
Outcome measures included the Neck Disability Index (NDI), Patient Specific Functional Scale (PSFS), NPRS, and Short Form-12 Physical Score (SF-12 PCS) and Mental Score (SF-12 MCS). Additionally, cervical AROM and deep neck flexor (DNF) endurance values were recorded each visit (Table 3). Outcomes were administered at initial evaluation and postoperative weeks 6, 9, 12, 18, 24 and 52 (Table 4). The NDI is a 10-item measure investigating disability in patients with neck pain, validated in patients with neck and arm pain and is used as a standard outcome measure after cervical spine surgery; it has a minimally clinically important difference (MCID) of 7.5 points.25 The PSFS assesses functional status change with meaningful patient-specific goals, with an MCID range between 2.0 and 3.0 points.26 The subject identified the following PSFS activities: looking over his shoulder while driving, performing left arm bicep curls equivalent to the right, getting a crossface in BJJ, defending darce choke in BJJ, and performing sexual activities. The NPRS is a valid and reliable measure of patient reported pain levels, with an MCID of 2.2 points.27 The SF-12 PCS assesses physical function and health, with an MCID of 8.1; the SF-12 MCS evaluates mental health with an MCID of 4.7 and an average score of 50/100, with higher scores indicating better function.28,29 Cervical ROM was measured using a dual-arm goniometer which has demonstrated reliability and validity in patients with neck pain.30
Improvements were noted with NDI (14% to 0%), PSFS (3.4/10 to 10/10), SF-12 PCS (+5.4) and SF-12 MCS (+25.7), and NPRS (2/10 to 0/10). Cervical AROM improved in extension 55-60 degrees, total rotation 60-75 degrees, total lateral flexion 20-45 degrees, and DNF endurance 5-35 seconds. Postoperative radiographs at week 6-12 no evidence of prosthesis malpositioning, displacement, subsidence or heterotopic ossification.
The subject met the MCID of NDI from preoperative to 12 weeks onward, and the minimal detectable change (MDC) from six weeks to 12 weeks onward.25 They also met the MCID of the PSFS preoperatively and postoperatively to 12 weeks onward.26 At one-year follow-up, the subject demonstrated carryover of no disability according to NDI, no limitations on PSFS; however, no notable significant improvement in SF-12 physical score, and rather a decline below average in SF-12 mental score.
After 14 visits across 16 weeks of PT, based on the subject’s subjective reports of improvement and having met their goals of gradual RTS after week 12, the subject was discharged from outpatient PT with a home exercise program, and continued monitoring outcome measures electronically up to one year. No adverse events including revisions, re-herniations, infections, or other healing complications arose during PT course or during follow up period.
DISCUSSION
This case report highlights the one-year outcomes of a successful postoperative PT program for a subject that underwent a two-level CTDR following symptomatic cervical disc herniation with associated radiculopathy. Being that literature regarding postoperative rehabilitation after cervical spine surgery is grossly limited, this case report attempts to add preliminary information regarding a multimodal postoperative PT program for CTDR.11,12,31
The subject demonstrated improvements in NDI, PSFS, NPRS and SF-12 PCS and SF-12 MCS. The subject’s improvements may be due to good prognostic factors including his preoperative cervical spine ROM, young age, prior level of activity, motivation, and self-reported adherence to home exercise program. In addition, the subject possessed no known risk factors or comorbidities such as poor bone quality, smoking history, obesity, diabetes, or advanced age that would increase risk for adverse events, hardware failure or delayed tissue healing timeline.12,32–34 The subject did report depression and anxiety preoperatively, which is described in the literature to have a strong correlation with chronic pain and negative prognosis post-CTDR, and as risk factors for failure to achieve MCID of NDI and Visual Analog Scale arm and neck.32–34 To mitigate these psychosocial factors as a potential barrier to recovery, the PT and surgical team recognized and addressed these early with a preoperative initial evaluation to set expectations and elaborate on the subject’s prognosis with and without surgical intervention, routinely reassessed outcome measures and highlighted progress with objective measures, and reinforced signs of good healing on radiographs. This enhanced expectations for therapeutic interventions which are associated with clinically meaningful improvements in function.35 In addition, early postoperatively the subject was encouraged to participate in a gradual walking program for safe aerobic exercise to help with inflammation, mood, and pain management. The physical therapist also discussed with the subject whether or not they feel their depression/anxiety is well-managed with their current psychology services and medication.35
It was noted that the subject’s SF-12 MCS scores peaked at six months and demonstrated a decline at one-year follow-up, though it still met the MCID for improvements from the initial visit.29 As the one-year updated survey was not obtained in person, no further reason or follow up on this decline was established, however it can be inferred the score being impacted due to multiple lifestyle factors such as personal or work-related stressors at the time impacting his overall quality of life, which could be independent of neck pain or disability.28,29
To the authors’ knowledge, this is the first case report documenting the postoperative PT in the successful management of a subject after CTDR. While there has been published literature regarding RTS, literature is lacking the content, timing and duration of postoperative PT and the rehabilitation process in general after CTDR.9,36–38 One published study looked at 50 male and female patients between 18-60 years following one-level CTDR and their respective return to physical activity levels; revealing all patients showed a significant improvement in premorbid status of radicular symptoms and improvement in NDI levels.36 Although the study showed 100% of these previously active individuals returning to activities at various competitive levels following CTDR, including two professional athletes returning to football, there was an 8% decline in returning to specifically ball and contact sports.36 The study did not describe any physical therapy postoperative management. The subjects were advised to resume any kind of physical activity slowly at their own discretion and to withdraw if they experienced stress or minor pain. Results showed median RTS ranges between 4-12 weeks, with follow up averaging 53 months.36 Conversely, this case report outlines a detailed postoperative physical therapy management that can be utilized by clinicians as a framework to guide patients towards RTS and activities, utilizing clinical reasoning to progress individuals according to their clinical presentation and personal factors.
Another case report highlighted a 23-year-old Division I football player returning to play eight weeks after 1-level CTDR without adverse events or complications at a nine-month follow up.9 No specific guidelines for progression or clearance to play were described other than the patient had four weeks of rest postoperatively and gradually returned to lifting, running and agility drills. No postoperative physical therapy was described, and no patient reported outcome measures were collected.9 The current case report similarly highlights clinically meaningful improvement after CTDR, however, it also supports this outcome with objective measures utilized to demonstrate patient progress.
A 2021 systematic review discussed a growing body of literature that supports that RTS is likely safe following ACDF, with minimal evidence studying CTDR.5 The general consensus is that athletes should be managed on a case-by-case basis depending on injury patterns and symptomatology, with most authors advocating for returning only once the athlete is asymptomatic with return of strength and ROM.5 RTS is to be approached very carefully especially in martial arts, where the cervical spine undergoes significant mechanical stresses; it has been shown to be safe to return to martial arts within one year following one-level ACDF, pending solid arthrodesis and absence of neurologic deficits.39,40 This case report demonstrates a possibility for similar outcomes for RTS with CTDR as compared to ACDF due to no adverse effects following one-year outcomes with RTS after week 12.
This case report is unique for several reasons. Foremost, it describes a framework utilizing clinical and objective milestones with respect to patient-related factors, surgical related factors and the available evidence for rehabilitation after cervical spine surgery to initiate and progress rehabilitation for CTDR. Interdisciplinary collaboration and communication with the surgical team was important for successful management. Clinical reasoning is ultimately what determined intervention selection and progression based on patient-specific factors utilizing both subjective and objective findings to guide patient care. Additionally, this is the first case report specific to CTDR with suggested postoperative guidelines that outline a comprehensive and detailed physical therapy rehabilitation program including manual therapy, therapeutic exercise, and patient education. To the authors’ knowledge, there is little published literature regarding therapeutic exercise to the cervical or thoracic spine after CTDR and no literature on the use of STM, scar tissue mobilization or accessory joint mobilization in the management of the postoperative patient with CTDR.41 This case report demonstrates that a multimodal PT program following CTDR based on tissue healing timelines and clinical reasoning improved pain, function and quality of life up to one year postoperatively without adverse effects in this athlete.
Limitations to this case report include limited generalizability of the results to any other populations due to including only one subject. As with all case studies, this study is based on one subject as a descriptive study design, and the effect of specific interventions on overall subject outcomes beyond the natural course of healing cannot be estimated as there was no control available. In addition, there is potential for selection bias, as there is strict criteria according to the Food and Drug Administration (FDA) for indications to receive a two-level Mobi-C implant prosthesis: must be a skeletally mature individual within the ages 18-69 years old, with radiographic confirmation and a diagnosis of radiculopathy, with neck and/or arm pain, and have trialed conservative management prior for at least six weeks without symptom resolve.42 He presented with no contraindications including infection, known allergy to the implant materials, no compromised vertebral bodies with previous trauma or deformity, no cervical instability or osteoporosis.42 Adherence to these strict criteria, and therefore the likelihood that the subject would likely be a young and healthy individual, may influence why the subject demonstrated a good response to surgical management and subsequent rehabilitation. Further research is warranted to support the utilization of safe, effective, progressively guided PT rehabilitation following CTDR to optimize patient outcomes, particularly with return to higher level function sports such as BJJ. Finally, this case report lacked a patient perspective as the report was written after the patient was discharged.
CONCLUSION
A multimodal PT program based on tissue healing timelines and clinical reasoning demonstrated significant improvements in pain, function and quality of life in a male athlete up to one-year after two-level CTDR with RTS to BJJ without adverse effects. This case report provides a framework for management of an athlete post CTDR to aid clinicians in practice and promotes a direction for future research to include controlled studies or case series.
Conflicts of Interest
JML: Consulting: SI-Bone Inc, Clinical Pattern Recognition LLC, GDS: Consulting: ZimVie Spine. The other authors report no potential conflicts of interest.
Corresponding Author:
Leana Mosesian, DPT
355 East Erie St
Chicago, IL 60611
Email: leana.mosesian@gmail.com
Phone: 312-238-1000