INTRODUCTION
Anterior cruciate ligament (ACL) ruptures are one of the most devastating injuries for athletes participating in sports requiring pivoting and cutting movements. The current standard post rupture is reconstruction with subsequent rehabilitation post-surgery that requires 9+ months prior to return to play.1 There is little consensus on the best return to play testing to reduce the risk of future injuries, with most of the research focused on quadriceps and hamstring function, different types of functional testing, prevention strategies for subsequent ACL injuries, and returning to athletic performance.1–3 Despite the large amount of research in these areas, only 55-65% of athletes will return to pre-injury performance and 20% will suffer a second ACL injury.4–7
Current ACL rupture rehabilitation guidelines focus on normalizing knee impairments of strength, range of motion (ROM), balance, agility, sensorimotor function, and neurocognitive demands required for return to sport.8 These guidelines, however, provide little discussion on testing for calf muscle impairments during both the pre and postoperative phases despite their contributions to running, jumping, and cutting activities.8–11 Further, interventions targeting calf musculature are either not mentioned or vaguely described in injury prevention and postoperative ACL reconstruction (ACLR) studies.8,12 Impairments in calf muscle function and their contributions to knee pain in other conditions have been described in the literature highlighting their importance.13–16 These unclear guidelines for calf muscle testing may lead to insufficient rehabilitation and contribute to the risk of subsequent ACL rupture or secondary injuries in the kinetic chain. To the authors’ knowledge, there are no studies directly examining the assessment of calf impairments or interventions to address them in the ACL deficient (ACLD) or ACLR patient.
Despite a high proportion of individuals being unable to return to sport long term, up to 90% of individuals expect to return to a high level of sport following ACL reconstruction.17 Given the disconnect between perceptions and reality, it is important to investigate all contributing variables associated with injury risk. This clinical commentary aims to examine the potential mechanisms surrounding the contributions of the gastrocnemius and soleus musculature on tibial kinematics, the effects ACL injury has on the calf musculature, and the potential clinical implications for prevention of subsequent injuries in the post ACLR rehabilitation framework. Sex differences and rehab considerations across the pre- and post-surgical ACLR timeline are also addressed.
MUSCULAR CONTRIBUTIONS OF THE SOLEUS AND GASTROCNEMIUS IN THE HEALTHY KNEE
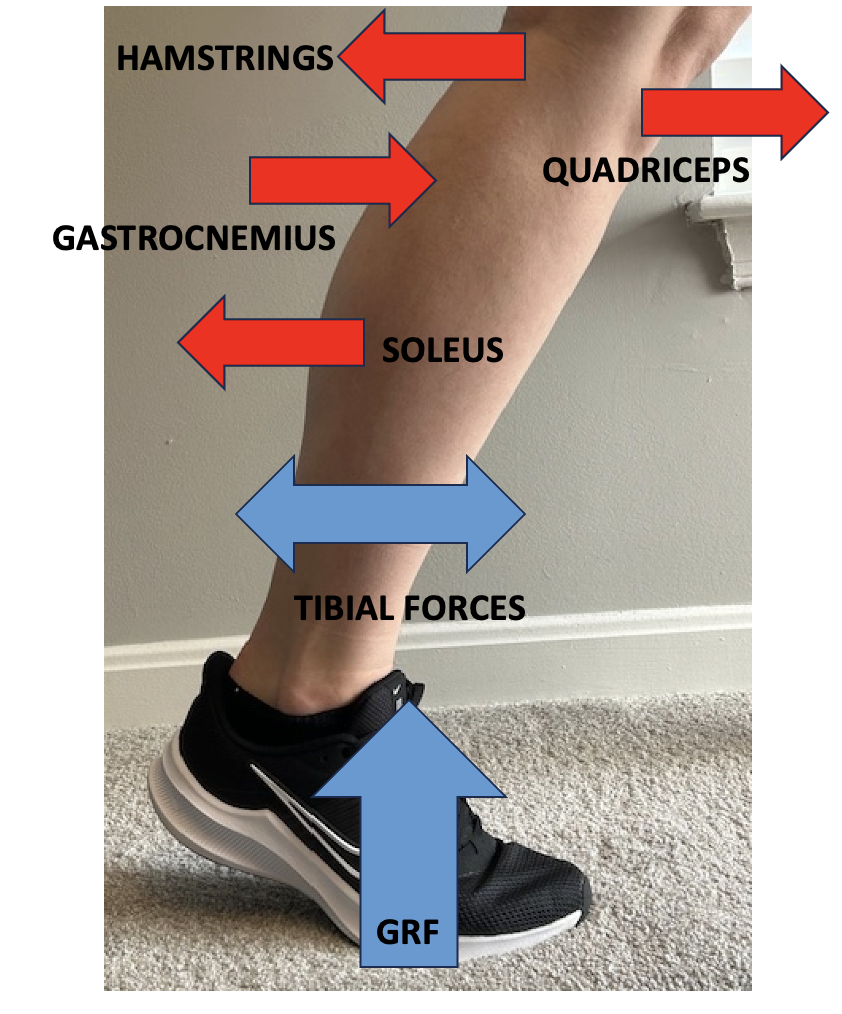
There is much discussion in the literature about the effects of the quadriceps and hamstring muscles on ACL strain.18,19 While both these muscles are the main contributors to tibial control and ACL strain, little is discussed about the effects that the soleus and gastrocnemius play as secondary restraints to tibial forces. The soleus and gastrocnemius musculature both have an effect on the ACL via control of tibial translation during movement.20,21
In healthy participants, the soleus acts as an agonist to the ACL. It contributes posterior tibial translation that is 28-32% that of the hamstrings and is active throughout knee flexion ROM (Figure 1).22,23 These forces on the tibia are seen in studies evaluating single leg drop landings and side cutting motions indicative of many sporting activities.20–22 The soleus also provides a slight varus moment at the knee during single leg landing tasks.21 This contributes some protection to valgus moments at the knee, which is regarded as a potential mechanism of injury for the ACL.24
The gastrocnemius also produces significant force production on the tibia during movement (Figure 1). It acts as an ACL antagonist causing anterior tibial translation throughout knee flexion ROM.25,26 Gastrocnemius anterior tibial forces contribute 97% of the forces contributed by the quadriceps during single leg landing and drop lateral jumps (334 N Gastrocnemius vs. 342 N Quadriceps).20 During healthy conditions, these significant tibial forces couple with agonist muscles of the ACL (i.e. hamstrings) to cause a compressive force at the knee joint leading to decreased ACL strain.27
Each head of the gastrocnemius muscle also performs a role in the transverse plane of motion. The medial gastrocnemius opposes valgus and internal rotation moments at the knee while the lateral head can contribute to these motions.20 Balance of these transverse plane forces can assist with controlling excessive knee valgus during jump landings, particularly with single leg landings. Under healthy conditions, the hip and knee demonstrate a greater ability to dissipate energy during double leg landings, while the hip and ankle dissipate most of the energy during single leg landing.28 Understanding these differences in landing strategies along with the unique individual roles of the calf musculature can assist in injury prevention.

Sex differences in calf muscle anatomy and physiology should also be considered in the evaluation, management, and prevention of ACL injury. Female athletes participating in cutting and pivoting sports are two to eight times more likely to rupture the ACL compared to males.29–31 While many of the potential factors for this increased risk have been previously explored, there are also potential differences in the calf musculature of healthy female athletes compared to males that may also contribute.31 When interpreting cadaveric studies, females show a higher surface area of soleus attachment to the tibia compared to males.32,33 Muscular surface area attachment size has been found to be proportional to force exerted on bone in in vivo studies.34 Increased muscular attachment area of the soleus in females may contribute to greater reliance for posterior tibial translation (i.e. ACL protection) with jumping and cutting tasks.22,23,34 Lower extremity weakness may be a predictor of knee injuries in female athletes but not males.35 As a result, weakness or arthrogenic muscle inhibition (AMI) of the soleus post ACL injury may contribute to females higher risk of re-injury.
When comparing the gastrocnemius muscle between females and males, several mechanical differences can be found. The medial head of the gastrocnemius muscle in females has a reduced pennation angle, smaller muscular cross-sectional area, and reduced composition of Type IIa fibers compared to males.36 These differences lead to lower force production and contractile speed, potentially reducing the female athlete’s ability to resist tibial internal rotation forces at the knee with cutting movements.20 Gastrocnemius changes either via inactivity or AMI post ACL injury could further these mechanical differences in females and lead to higher risk of re-injury.
Under conditions that required reaction to a perturbation, Haddara et al. found differences between males and females in both soleus and gastrocnemius activation.37 When examining muscle activation during a perturbation while walking, the soleus generated about half the amount of force in females than males. Further, females also exhibited about 2.6 times more gastrocnemius force with perturbation in terminal stance phase of gait than males.37 These differences in combination with quadriceps and hamstring deficits in healthy females may be a factor in the higher incidence of non-contact ACL injuries.38
MUSCULAR CONTRIBUTIONS OF THE GASCTROCNEMIUS AND SOLEUS IN ACL DEFICIENT KNEES
After ACL rupture, there are adaptations of both the gastrocnemius and soleus muscles in the involved limb versus that of the uninjured side (Table 1). Adaptations often occur in conjunction with quadriceps and hamstring muscular activity changes in response to neuromuscular alterations in the ACL deficient (ACLD) knee. These changes should be thoroughly assessed and treated in those undergoing non-surgical rehabilitation as well as those participating in pre-surgical rehabilitation programs.
When examining the gastrocnemius specifically, there are changes seen in muscular activity with gait in the ACLD patient. The medial gastrocnemius demonstrates earlier onset at initial contact and prolonged activity in the gait cycle compared to healthy controls.39,40 Despite this earlier onset and prolonged activity period, there is decreased overall gastrocnemius electromyography (EMG) amplitude in the ACLD knee during the gait cycle compared to healthy controls.41,42 Using musculoskeletal modelling, Sharifi and colleagues examined changes in gastrocnemius activity and the effects on knee instability during the mid to late stance phases of gait in the ACLD knee.43 With this modeling, they also found prolonged gastrocnemius activity in the gait cycle, which led to increased anterior tibial translation and knee instability during the stance phase of the gait cycle.43 This further supports the gastrocnemius as an antagonist to the ACL during gait.
Gastrocnemius muscular changes are also seen with more dynamic activities. Increased EMG signaling of the medial gastrocnemius and decreased lateral gastrocnemius activity have been found in ACLD patients with single leg hops compared to healthy controls.44,45 The medial gastrocnemius contributes 15 Nm of varus force versus 32-38 Nm of force from the gluteus medius during single leg landings thus providing only a marginal protective compensation.21,46 With more horizontal decelerating tasks, such as pivoting, the gastrocnemius had higher peak activity and longer duration when completing the task in ACLD knees versus healthy controls.47 Steele et al. created a more complex environment by adding a ball catch to a single leg deceleration landing and found earlier onset medial gastrocnemius EMG activity in ACLD patients versus controls.48 Medial gastrocnemius EMG activity was also found to be earlier in onset than the quadriceps in the ACLD knee in this study.48 These studies show significant changes in medial gastrocnemius activity of the ACLD knee and may reflect a protective mechanism in the transverse plane. Further research is needed to confirm these findings.
Soleus EMG changes in the ACLD knee have also been documented in the literature, albeit with lower frequency compared to the gastrocnemius (Table 1). During the gait cycle, the soleus has been found to have lower EMG activity from weight acceptance through the midstance phase of gait in ACLD patients compared to their contralateral side.49 When assessing more dynamic tasks, conflicting results have been found. With single leg landing activities, increased soleus EMG activity has been found compared to healthy controls.50 This may be a compensation for controlling anterior tibial translation in the ACLD knee.
When assessing patients with an ACLD knee, it appears imperative to evaluate all structures that could improve knee stability and function, specifically the calf. The studies cited above demonstrate the need to restore calf muscular strength as it undergoes changes that alter dynamic knee stability patterns. Studies have recommended a Limb Symmetry Index (LSI) of at least 90% quadriceps strength prior to return to activity.67 An LSI of at least 90% of both the gastrocnemius and soleus musculature is also recommended to ensure sufficient force production patterns of the lower limb required for sports participation.
MUSCULAR CONTRIBUTIONS OF THE SOLEUS AND GASTROCNEMIUS IN THE POST-OPERATIVE ACLR KNEE
When assessing the postoperative ACLR knee, most research has been focused on AMI of the quadriceps muscle.68 While there is agreement about the effects that AMI has on long term outcomes for the patient, the potential ramifications of muscular alternations elsewhere in the kinetic chain are unclear. For example, in chronic ankle instability (CAI), alterations in hip and knee strength have been found.69 This highlights potential neuromuscular changes in the entire kinetic chain with a chronic injury. These muscular changes could lead to subsequent injuries upon return to sport, either as a secondary ACL rupture or other injuries not often grouped in the rates of re-injury with return to play.5,7,70 While the effects of the soleus and gastrocnemius on the intact ACL have been documented in previously discussed research, it is also important to focus on how these muscles are altered in the postoperative knee.
Studies looking directly at effects on the soleus muscle post ACLR are sparse. At up to 12-24 months post-op, decreased peak soleus EMG activity has been found with landing from a single leg forward hop versus healthy controls.51 This is important as the soleus provides positive support and braking forces through landing and stabilization phases of a forward hop, and for reducing anterior tibial forces and performance of change of direction movements.51 Despite decreased peak EMG activity, other studies have shown faster reaction times of the soleus compared to healthy controls from six months to one year postoperative.52,53 Combining decreased peak force with earlier EMG onset in the movement pattern provides a potential mechanism for secondary ACL injury and/or Achilles tendon rupture. When looking at patients with quadriceps inhibition, Kuenze et al. found increased volitional soleus EMG activity with exercise and at rest post exercise in patients who underwent ACLR with hamstring and patellar tendon grafts.54 Increased muscular EMG response at rest is in contrast to healthy subjects in response to exercise activity.71 These changes are most likely due to compensatory neural changes in patients with quadriceps AMI and provide another potential mechanism for secondary injuries to the calf region if not corrected prior to return to sport.54
The gastrocnemius muscle has shown alterations in muscle activity post ACLR (Table 1). Several studies have shown a decrease in both medial and lateral gastrocnemius EMG activity with single leg landing tasks.55,56 This may be an adaptive protective mechanism to reduce anterior tibial forces. This adaptation, however, places increased reliance on passive restraint mechanisms (i.e. tendons, ligaments, cartilage) to absorb forces and the decrease in co-contraction can cause increased knee joint strain.18 Dashti Rostami et al. found that when medial and lateral gastrocnemius muscular activity was decreased, there was an increase in posterior and vertical ground reaction forces in ACLR patients, which is often associated with an increased ligamentous strain.18,57 Further, decreased preparatory and reactive EMG activity to landing tasks of the gastrocnemius has been found in ACLR patients.58 This delay in activation further increases passive restraint required to complete jump landings. Though studies have shown a decrease and delay in EMG activity of the gastrocnemius with landing tasks after initial contact from landing, there appears to be a prolonged EMG activation.59 This prolonged activation may place increased anterior tibial tension that places the patient at risk of injury with immediate subsequent movements often required in cutting sports and can lead to other injuries in the kinetic chain (i.e. Achilles tendon rupture). In studies attempting to replicate more reactive tasks indicative of sporting demands, changes in gastrocnemius EMG activity continue to be present.56,60,61 These gastrocnemius EMG alterations do not appear to correct over time. ACLR subjects at least one year and up to ten years postoperatively have been found to have continued deficits in gastrocnemius activation with jump landing tasks.56,60,61 This is significant as most athletes post ACLR are returning to play during the 9-12 month postoperative time period with ongoing deficits.
When examining straight line running, decreased peak EMG activity of the medial gastrocnemius has been found during the late stance phase of gait in ACLR patients versus healthy controls.62 EMG activity of the medial gastrocnemius was unchanged regardless of foot strike pattern in patients 6-10 months postoperative.62 Decreased medial gastrocnemius activity at late stance phase may limit propulsion forward of the athlete effecting performance and potentially causing compensations within the kinetic chain. In contrast, Forelli et al. found a significant increase in EMG activity at the gastrocnemius muscle with running in ACLR patients at six months post-op.63 The EMG results are based on the summation of the muscle activity throughout the gait cycle versus individual time frames in the previously mentioned study, however, which may explain some of the differences found.
When examining biomechanical alterations of joint forces after ACLR, several patterns develop at the ankle. With a forward hop motion, decreased peak ankle dorsiflexion range of motion has been found at initial contact versus healthy controls.51,53,64 Decreased ankle dorsiflexion ROM is most likely a compensation for decreased knee flexion active ROM during the eccentric stopping phase of the landing and likely increases use of calf musculature to complete the activity.65 Coupling this increase in ankle joint strategy with plantarflexion power deficits of up to 34% at the injured limb, leaves the reconstructed limb with insufficient capacity to dissipate forces properly.72 Increasing reliance on calf musculature may increase the risk of injury to not only the knee joint, but also calf musculature. With more vertical landing motions, similar biomechanical changes are found. With single leg vertical drop landings, increased plantarflexion ROM at landing had been found versus healthy controls at 6 months that did not significantly reduce until after 18 months.66 Similar findings have been found with double leg vertical landings at one year post surgery with increased energy absorption from the knee and ankle compared to healthy controls.73 Further, up to 37% more eccentric work has been found at the ankle versus healthy controls when landing from a vertical jump.73 These are concerning biomechanical changes that persist into athletes return to play time frames. In contrast to these alterations in jumping tasks, running mechanics appear to be unchanged at the ankle in long term studies.74,75 Changes with joint kinematics have been documented at the knee with running, however, at up to 12 months post-surgery.76
REHAB IMPLICATIONS FOR THE SOLEUS AND GASTROCNEMIUS POST ACLR
Early Postoperative Period (Weeks 1 – 6)
Considering the numerous alterations to calf function seen in the ACL population presented thus far, further attention may need to be directed to the gastrocnemius and soleus musculature in individuals recovering from ACL injury. Table 2 presents example interventions to address muscle performance deficits through the rehabilitation timeline post ACLR. In the early stages of rehabilitation post ACLR, there are several factors to consider that may affect the gastrocnemius and soleus musculature. One such factor is gait mechanics. Most patients post ACLR are allowed weightbearing in a locked brace with crutches or non-weightbearing (NWB) if a concomitant meniscus repair was performed.77 This locked brace pattern often causes a foot flat gait and limited ankle plantarflexion at toe off phase of gait. This can limit gastrocnemius and soleus contraction. NWB status in those also undergoing meniscus repair with ACLR can affect muscle atrophy. While there is no known study on muscle atrophy post ACLR in humans, a study performed on rats that had a NWB status post ACLR found that the gastrocnemius and rectus femoris were both found to have atrophy at as early as 7-10 days post-op.78 The gastrocnemius was also found to have significantly more atrophy, downregulation of insulin-like growth factor-1, and increased expression of atrogin-1 compared to the rectus femoris during the NWB time period post ACLR.78 In human studies, atrophy of the quadriceps muscle in healthy individuals undergoing NWB of the lower extremity was seen at as early as five days.79 Interventions targeting gastrocnemius and soleus activation in NWB positions are important to facilitate muscle activation and offset the effects of these gait abnormalities.
Another consideration in the early ACLR post-operative period is the presence of gastrocnemius and soleus AMI in post ACLR patients. While there is no known research looking directly at AMI of the gastrocnemius and soleus post ACLR, AMI of these muscles have been found in individuals with other lower extremity injuries.80–82 In studies artificially causing AMI at the knee joint via simulated effusion, however, increased activation of the gastrocnemius and soleus have been found.83 The authors of this study relate these changes as compensations for inhibition of the quadriceps found as a result of these alterations in knee status.83 It is still unclear whether these artificial joint alterations are sufficient to simulate the post ACLR state.
Each postoperative ACLR patient should be individually assessed for gastrocnemius and soleus muscle function looking for muscle weakness, activation difficulty, and significant muscle atrophy, which may be indicative of AMI.68 Ito et al. found that American football players two years post-ACLR demonstrated significant gastrocnemius muscle cross-sectional area deficits compared to their contralateral limb.93 While muscular cross-sectional atrophy is only one component of AMI, these findings do highlight the ongoing long-term deficits in calf muscle function. As a result, interventions directed at the calf musculature to combat atrophy or AMI should be started in the immediate post-operative period. Interventions of neuromuscular electrical stimulation, blood flow restriction therapy (BFR), biofeedback, joint cooling, and neurocognitive interventions have all been shown to have a positive effect on the symptoms of AMI in the early phases of rehabilitation.68,84–86,94 Progressive resisted exercise should also be introduced early in the postoperative protocol within weightbearing restrictions. Type II muscle fiber recruitment should be emphasized through moderate to high intensity loads (70-85% 1RM) for 3-5 sets of 6-12 repetitions.87 In patients that are NWB or are unable to achieve higher intensity loads on their own, BFR can be used to reach sufficient recruitment of Type II muscle fibers with otherwise low intensity exercises (i.e. seated heel raises).88
Middle to Late-Stage Postoperative Period (Weeks 7+)
In the middle to late stages of rehabilitation post ACLR, there is a shift towards more specific interventions directed toward functional and sports specific movements (Table 2). Once sufficient muscle activation is achieved, emphasis should be placed on strengthening the gastrocnemius and soleus musculature in addition to the quadriceps, hamstring, and gluteal muscles to the demands required for daily functional activities and sport specific tasks. Emphasis should be on muscle strength and hypertrophy with resistances at 67-85% 1RM for 3-5 sets of 6-12 repetitions.87 Exercises should begin in neutral ankle positions and progress to various angles to simulate the demands of cutting sports. Positioning the foot in more outward positions has been shown to stimulate more of the medial gastrocnemius and inward positioning of the foot has been shown to stimulate more of the lateral gastrocnemius.89–92 Different knee angles should also be included to bias the soleus musculature as the knee flexed position is readily performed in sports.
Eccentric strength training should also be emphasized during this period. An inability to eccentrically control the calf musculature can lead to rapid elongation of the Achilles tendon, which is often the mechanism of acute Achilles tendon ruptures.95 Eccentric strength can assist in controlling this elongation during deceleration and change of direction tasks during later stages of rehab and return to play.96,97 Achieving an overall goal of at least 90% limb symmetry index of the calf musculature with isokinetic or hand-held dynamometry testing prior to return to sport.98,99
In addition to strength training, emphasis should be made on individualized plyometric and power training of the calf musculature with progressions to explosive whole-body movements as the athlete moves through the rehabilitation process. Tensile forces on the Achilles tendon can be as high as 12 times body weight with running and jumping activities and must be trained to at least match these demands.100,101 Exercises challenging the stretch shortening cycle (SSC) of the calf musculature should be employed in various ankle and knee positions to gradually restore the explosive properties required for these activities within the demands of each individual’s sport. Exercises challenging the SSC of the calf should be performed in isolation and then combined with movements using the entire kinetic chain to re-develop tendon energy storage and release as well as mechanical stiffness.102 An inability of the neuromuscular system to absorb load can increase the requirements of passive structures (i.e. tendons, ligaments, cartilage) to dissipate forces and potentially lead to injury.18 As is described in quadriceps rehab post ACLR,103 rate of force development (RFD) is an important measurement to consider in the calf musculature in addition to maximum force output. RFD is vital for sports performance as it allows for explosive movements in short periods of time. Once 90% LSI of calf musculature of the uninvolved leg is achieved, an increased focus on these power movements should be made.104,105 While no study has directly measured calf deficits in RFD post ACLR, other studies have shown decreased RFD of the calf musculature in other lower extremity pathologies.106,107 An emphasis on individualized quadriceps, hamstring, and triceps surae RFD restoration should be made post ACLR in addition to whole body movements (i.e. Drop jumps) to reduce functional compensation patterns.
Another important part of late stage ACLR rehabilitation is addressing kinematic impairments across various sports movements. Much is discussed about athletes changing to a hip dominant strategy for both concentric and eccentric movements post ACLR. Less discussion is available on the potential for an ankle dominant strategy to develop in these patients. Based on the research discussed previously,51,53,64,73 there is a potential for some post-op ACLR patients to develop this strategy in compensation for proximal lower extremity deficits. It is important to address these deficits prior to beginning high speed agility and plyometric training. If all requirements have been met, then a movement assessment should be performed. At the minimum, visual assessment with video playback should be used to assess and instruct athletes into more balanced strategies for movement. Use of force plates and 3D kinematic analysis should be considered when available. The use of external focus strategies when retraining these movement patterns has been found to be superior to a more internal approach.108 As the athlete progresses, the addition of complex environments should be used. The progression from simple to complex athletic situations to challenge the neurocognitive systems and to meet the demands of sport should be made with the athlete maintaining the correct movement strategies.
FUTURE DIRECTIONS
Since there is limited research on the effects on the gastrocnemius and soleus musculature post ACLR, larger well-designed studies are needed to confirm the above findings. Additional studies examining the effects of graft types, weightbearing status after ACLR, sex differences, and concomitant meniscus/ligament injuries should be performed to further examine the effects on the triceps surae musculature. Studies examining ACL injury prevention and ACLR rehab programs with increased emphasis on calf muscle training should be performed to assess additional effects on reducing injury rates and with return to sports performance secondary to gastrocnemius and soleus involvement in tibial kinematics. Similarly, studies examining strength ratios between the triceps surae musculature and the hamstring and quadriceps should be performed to address the minimal requirements for injury prevention and performance.
CONCLUSION
ACL injuries remain a common injury in cutting and pivoting sports. Return to sport and performance rates remain below patient expectations following ACLR, requiring further exploration of contributing variables for full participation. The role of the triceps surae musculature in the ACLD and ACLR knee is often not discussed in pre- and post-surgical protocols. Further research looking at the effects of triceps surae interventions in the prevention and management of ACL injuries is warranted to assess for improvements in return to sport and performance for athletes.