INTRODUCTION
The glenohumeral joint is the most mobile and least constrained in the human body. Therefore, it is one of the most commonly traumatically dislocated joints, with incidences ranging from 11.2 to 23.9 per 100,000 injuries.1 A complex combination of static and dynamic stabilizers over the glenohumeral joint balances this inherent mobility with functional stability.2 The dislocation mechanism most frequently occurs when the arm is forced into abduction, external rotation, and hyper-extension, forcing the humeral head out of the glenohumeral joint.1
Suspension training is a promising method for injury prevention, rehabilitation, and return to play.3–5 The difficulty of the exercise and the number of motor units recruited depend on the instability caused by the suspension device and the body position.4 The use of vibration as an addition to exercise causes an increase in the activity of the shoulder girdle muscles.5 Exposure to vibrations also alters muscle recruitment, improving readiness for movement.6 Vibration training induces vibratory stimuli to the muscle to elicit the tonic vibration reflex. Adding mechanical vibration produces changes in the activation of motor units,7 reinforcing the potential benefits of using such devices in standard training methods.8 Whole-body vibration applied via platforms is the most-studied method for eliciting acute neuromuscular effects and long-term adaptations.9 Vibration superimposition may be a suitable strategy for improving muscular activity in suspended push-ups with frequencies of 25 Hz and 40 Hz, causing similar effects on overall activity assessed via surface electromyography, except for the triceps brachii and the anterior deltoid during the eccentric phase.6 However, the effects on the upper body muscles are still unclear.6
The purpose of this case series was to examine the effect of seven weeks of strength training using a novel vibration device (superimposed vibration with 40 Hz frequency) with an attached suspension strap on two subjects recovering from a shoulder subluxation.
METHODS
Two subjects were studied:
Subject 1 (25 years old, 181 cm, 74.8 kg) is right-hand dominant and sustained a left shoulder subluxation on 10/19/2022, after performing an exercise with a TRX in a session before basketball court training. He was immobilized for 15 days with a sling. He was diagnosed via MRI-Arthrogram on 10/27/22, with focal disinsertion of the anteroinferior glenoid labrum without apparent injury to the bone ridge or periosteum and acute Hill-Sachs trabecular contusion in the posterosuperior region of the humeral head.
The subject gradually returns to activity presenting limited mobility on 10/2/2023 in the last degrees of external rotation and shoulder abduction and performing 2-3 strength sessions per week; during this period, he had only performed exercises with elastic resistance and weights and had avoided any contact sports.
Subject 2 (19 years old, 188 cm, 79.3 kg) is left-hand dominant and sustained a right shoulder subluxation on 01/22/2022, after a collision during a basketball game. He was not immobilized, played with an adjustable shoulder brace 15 days later. He was diagnosed via MRI on 01/28/2022 with joint effusion and small Hill-Sachs and Bankart lesions. After continuing to play, he suffered several episodes of instability, subsequently undergoing a arthroscopic surgical procedure on 05/24/2022, where an anterior capsulolabral reinsertion was performed with FiberTack implants with good glenohumeral re-centering.
As of 10/2/2023, he did not present with any discomfort or instability and was performing three upper-body strength training sessions per week while competing in semi-professional basketball. During this period, he had carried out post-operative rehabilitation with one month of immobilization and four months of recovery through the use of Blood Flow Restriction (BFR), elastic resistance, weights, and dynamic stability exercises, returning to team training on 3/10/23 and competition on 10/29/23.
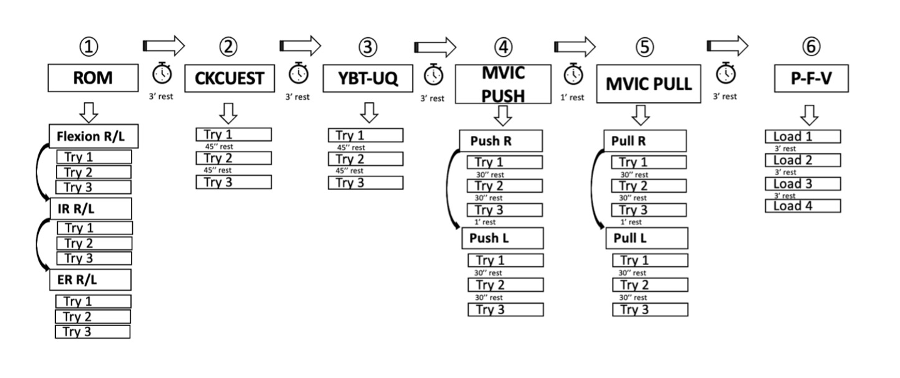
One week before the initial testing, both subjects attended a familiarization session with the entire testing procedure (Figure 1).
Procedures
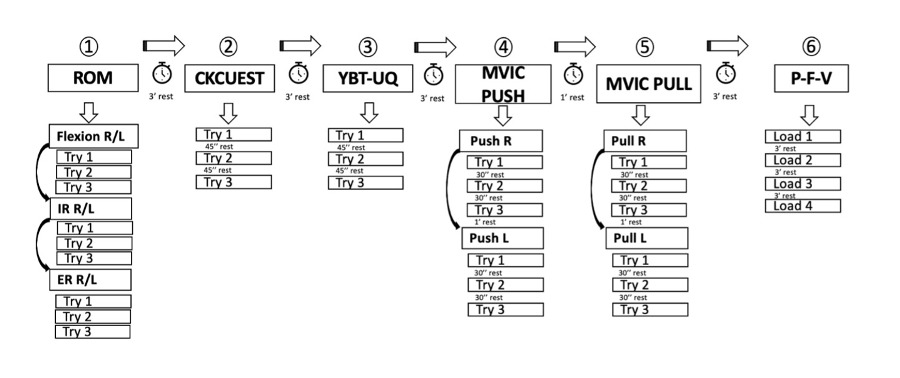
The initial evaluation session took place one week later at the same time. After a standardized warm-up (500-m rowing using an ergometer, five-minute active stretching, and upper body mobility; two submaximal isometric pulls and isometric pushes and two submaximal medicine ball throws), participants performed different tests to assess mobility, stability, strength, and power.
For the range of motion (ROM) analysis, the initial extremity was selected at random, and active flexion, internal and external rotation were assessed three times using the mean angle (º) for each ROM.10 Shoulder flexion ROM was measured with a standard goniometer displaying the participants in a supine position. Internal and external shoulder rotation ROMs were measured using a goniometer in the same supine position, and the shoulder abducted at 90° and elbow flexed at 90°.10
To assess glenohumeral stability, the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) was used. Participants assumed a push-up position with their hands 91.4 cm apart and with both shoulders’ perpendicular to the hands. From this position, the dominant hand crosses the body, touches the non-dominant hand and returns to the starting position. The same movement was then performed with the non-dominant hand. The participant was instructed to perform as many alternate touches as possible in 15 seconds while maintaining the correct flexion position.11 The Y-Balance Test-Upper Quarter (YBT-UQ), a closed kinetic chain functional screening tool using the Y-Balance Test Kit (Move2Perform, Evansville, IN, USA), was performed.11 Subjects stand with the tested shoulder perpendicular to the hand and their feet shoulder-width apart. The test hand is placed on the platform with the thumb behind the red line. From this position, the free hand should push the reach indicator as far as possible in the medial (M), inferolateral (IL) and superolateral (SL) directions and then return to the starting position in a controlled manner.11 For the analysis, the average number of touches of the three attempts (CKCUEST) and the mean distance (cm) for each direction range (YBT-UQ) were used.
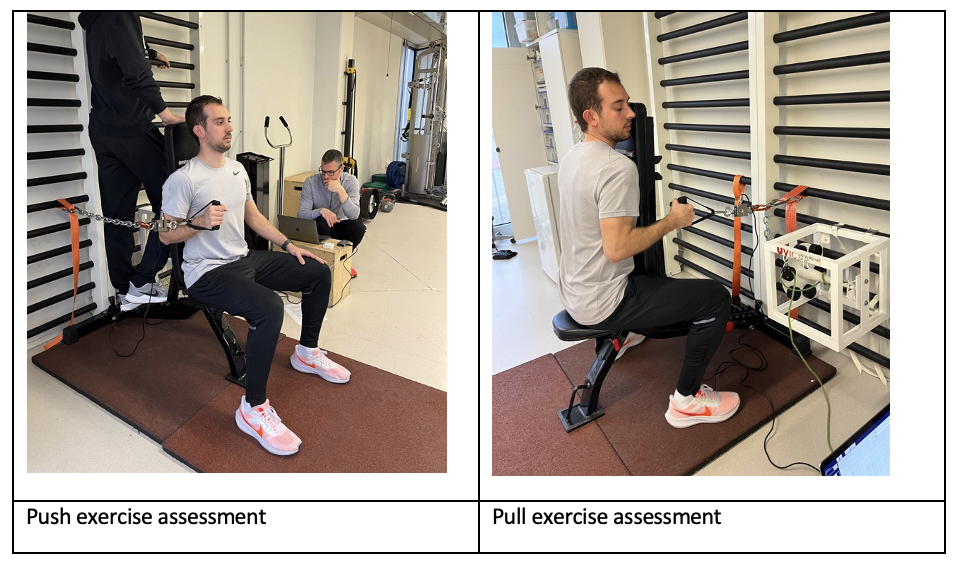
The strength assessment was carried out next, using a strain gauge (Chronojump, Boscosystem®, Barcelona, Spain) to perform unilateral maximal voluntary isometric contraction (MVIC) (push and pull, in this order, Figure 2). The initial extremity was assigned at random. The MVIC exercises were performed in a seated position, with the chest (pull) or back (push) maintaining contact with the base of the bench back, positioned in line with the vertical. Participants maintained 90º elbow flexion during MVIC push-pull exercises, with a neutral shoulder position in the frontal and sagittal planes. A handle and a steel chain were anchored to the back support. Participants were encouraged to hold the MVIC for five seconds in each exercise. The MVIC (N) was measured at a sampling frequency of 80 Hz (Chronojump, Boscosystem®, Barcelona, Spain). The mean peak force (in newtons) was calculated from three repetitions and used for the analysis.
.png)
Finally, the load-velocity or force-velocity profile of the bench press at rest was determined using an Olympic bar (20 kg) and plates, using a linear encoder (Vitruve, Spain) to measure the mean propulsive velocity (MPV, measured in m.s-1).12 Before initiating the concentric phase (push) with maximal speed, participants were instructed to hold a brief one second pause with the bar stabilized on the chest. Four to five loads were used to find a load-velocity range of 1.3 m.s-1 (40% of 1RM) to 0.5 (80% of 1RM), performing two to three repetitions at the highest velocities and one repetition at the higher loads.13
The familiarization session approached the loads used during the initial assessment session. During the final assessment, the same absolute loads were used to compare the velocities with the same loads. The maximum velocity of each load was used for the analysis. A complete repetition load (1RMtest, kg) was estimated using linear regression of each participant’s data, using a standardized MPV of 17m.s-1 at 1RMtest.14
Interventions
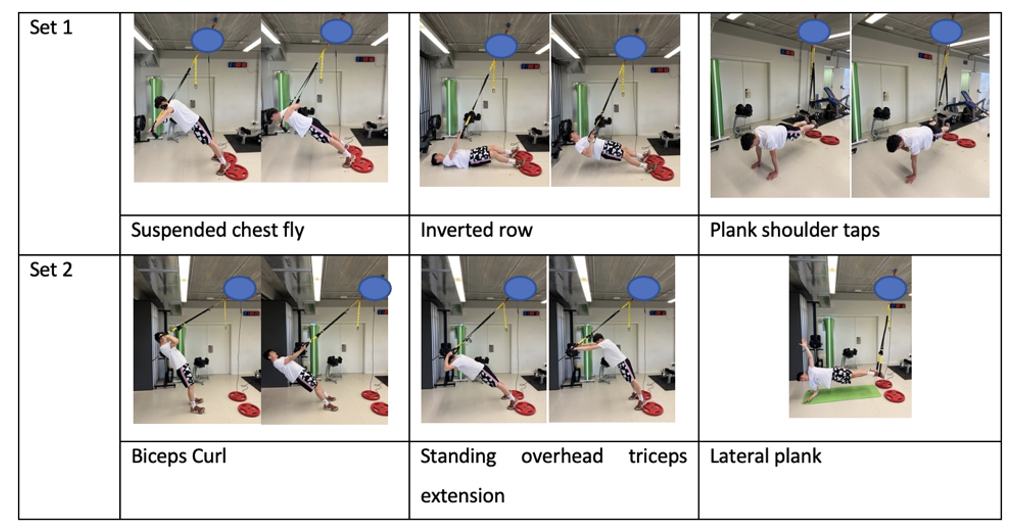
The training intervention was performed twice per week for seven weeks and consisted of six exercises divided into two blocks of three exercises (Figure 3). These exercises were chosen because unstable resistance training stresses the neuromuscular system and can promote higher strength gains and increases in cross-sectional area. Additionally, suspension training elicits higher activation, measured via electromyography (EMG), in most of the primary muscle groups engaged during these exercises, compared to their traditional resistance training equivalents.3
_were_.png)
Three sets of eight repetitions of each block were performed, resting 30 seconds between exercises and three minutes between blocks, following established protocols found in the literature serving similar purposes.15–17 Eight touches were performed per arm during the shoulder taps exercise, and the side plank was held for 25 seconds on each side. Participants performed the superimposed vibration intervention using a custom vibration device with the frequency set at 40 Hz. The vibration instrument used is a patent-pending device placed between the suspension strap and the ceiling anchorage to superimpose vibrations on the suspension straps. This device includes a rotating electric motor that transfers movement to a connecting rod, generating a vertical displacement of 8 mm (peak-to-peak). The intensity of the exercises, except the shoulder plank and side plank, was individualized for each participant at a rate of perceived exertion (RPE) intensity of 7-8 or 2-3 repetitions in reserve (RIR).18 The distance between the suspension strap and the feet was also recorded for each participant and set as a reference for subsequent exercise training, except for the shoulder and side plank. The suspension straps were standardized at 65 cm height from the floor for each exercise and training session. Participants performed the entire intervention under the supervision of the research team.
The study followed the Declaration of Helsinki principles, and participants were informed about the procedures, agreed to participate, and provided their written consent. The study was approved by the University of Vic-Central University of Catalonia Research Ethics Committee (registration number: 204/2022). The study followed the CARE guidelines.
STATISTICAL METHODS
Data are presented as mean values. To assess changes at the individual level, the coefficient of variation (CV, %) was measured from the average value of the test and the between-repetitions SD (CV=SD/average value *100). The CV % is better interpreted than the SD when different scales are used.
OUTCOMES
Table 1 shows the reliability of the data expressed as the Coefficient of Variation (%).
The pre and posttest values for each subject are presented in Table 2, presenting the percentage change (%). The coefficient of variation (CV%) was used to determine the likelihood of the change to be real (1*CV=likely; 2*CV=very likely). For the ROM assessments, the greatest improvements were found in the IR (around 50% improvement), compared to a 5% in flexion and 20% in ER. At the group level, significant improvements were observed in the range of motion for internal rotation (IR) in both the injured and non-injured arms, as well as in external rotation (ER) of the injured arm. In the glenohumeral stability tests, notable enhancements were recorded in all the positions of the Y Balance Test - Upper Quarter (YBT-UQ) for the injured arm (between 5% and 33% improvements depending on the position), and the CKUEST (10-20%). Additionally, significant gains were seen in the injured arm during isometric push and pull tests (around 10%), but no differences in the dynamic strength in the bench press exercise force velocity profile.
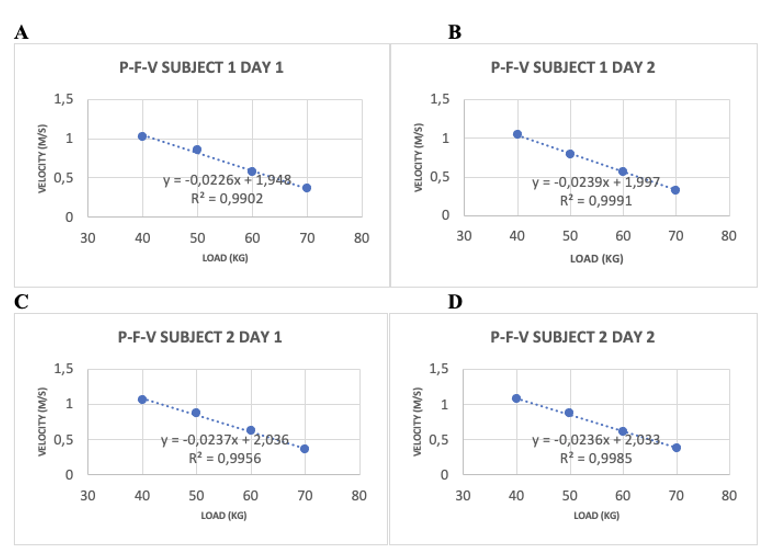
The theoretical 1RM was estimated after an incremental four-load test of 40, 50, 60, and 70 kg to analyze the improvement of the force-velocity profile (FVP). Subject one went from a theoretical 1RM at 0.17 m.s-1, ranging from 78.67 to 76.44 kg, and subject two went from a theoretical 1RM at 0.17 m.s-1, ranging from 78.73 to 78.94 kg (Figure 4).

DISCUSSION
The primary objective of this case series was to evaluate the impact of superimposed vibration on suspension strength training in subjects recovering from shoulder subluxation. The results indicate improvements in range of motion, particularly in internal rotation of both the affected and unaffected arms, as well as external rotation of the injured arm. Moreover, improvements were noted in glenohumeral stability assessments, specifically in the medial and superolateral positions of the Y-Balance Test for the upper quadrant. Notably, the affected limb had a marked increase in isometric pull and push strength.
These findings align with previous research highlighting the benefits of incorporating instability and body weight resistance into upper-body strength training, resulting in heightened neuromuscular demand.19 Nevertheless, it is worth noting that the two subjects’ improvements were not uniform across all tests. This variation can be attributable to the fact that while vibration training can increase muscle activation,20 significant chronic improvements in maximal strength measures, such as 1RM elbow flexion, may not be evident in every individual.21
No improvements were seen in bench press 1RM values either, as assessed using the load-velocity profile test (described in the Methods section). It is worth emphasizing that there are limited observational or experimental studies assessing the chronic effects of vibration in the upper body, as numerous studies primarily focus on muscle activity measured through EMG or concentrate on the lower body.6 It is still unclear whether vibration training is better than traditional upper-body strength training methods in improving maximal strength values. Some studies have shown that instability can restrict the execution of maximal strength demands, making it a less optimal mechanism for intervention.
The effects of vibration training using a suspension device on shoulder stability measured via CKCUEST and YBT-UQ tests in this case series highlight new possibilities in shoulder injury rehabilitation. The stability of the shoulder relies heavily on the rotator cuff. Therefore, combining suspension training with vibration may affect the muscles in this group. Given the prevalence of rotator cuff injuries, improved stability in the glenohumeral joint may be helpful for athletic populations participating in overhead sports (throwers, swimmers, and tennis players). This improvement may be attributed to the increased neuromuscular activation brought about by the superimposed vibrations. This activation facilitates the coordinated and controlled engagement of the shoulder muscles, ultimately strengthening the joint.22 Moreover, vibration training using a suspension device can be tailored to target specific rotator cuff muscles since there is evidence that some specific positions recruit the electromyographic activity of these muscles more than others. More motor units and muscle fibers would be recruited theoretically with increased muscle preactivation, which may reduce myofibrillar stress during repeated muscle contractions.23 Potentially, vibration may influence the activation of afferent input from sensory units in muscle fibers and provide attenuated pain sensation associated with exercise or increased lymphatic blood flow and the removal of metabolic wastes (H+).23
A notable gap in the existing literature concerning integrating vibration training with other exercises and implements was explored in this case series, particularly in the context of shoulder subluxation rehabilitation. However, further investigation is necessary to understand the long-term effects of vibration training and its potential as a therapeutic tool for shoulder rehabilitation in different phases of the therapeutic process. This lack of evidence may make it difficult to determine if this technology can replace or be utilized alongsid traditional resistance training in rehabilitating injuries in this anatomical region.24
It is essential to acknowledge the limitations of a case series approach. Only having two subjects with different types of injuries and different previous therapeutic approaches that were included strongly limits implications for other subjects. The training period consisted of only seven weeks, limiting the observation of longer-term effects. Future studies should consider other experimental designs, incorporating experimental and control groups, and varying vibration frequencies or adjusting sets and repetitions. Furthermore, the specific device used, vibration program settings, and exercise selection differed from prior investigations, limiting outcome comparisons.
CONCLUSIONS
In summary, this case series highlights the potential advantages of incorporating superimposed vibration during suspension strength training for subjects recovering from shoulder subluxation. However, further research is necessary, utilizing diverse designs and varying experimental conditions, to fully comprehend the magnitude of these benefits and to ascertain whether this technology can be effectively integrated with traditional resistance training to enhance shoulder stability and overall health.
Declaration of Conflict of Interest
Javier Peña, Bernat Buscà, and Joan Aguilera-Castells have submitted a patent application (number 202430119) to the Spanish Patent and Trademark Office (OEPM) for a specialized vibration device designed for athletic, fitness, and health applications. Currently, no companies hold the rights to this device, and it is neither being commercialized by the authors nor by any third parties. The other authors have declared that they have no commercial or financial relationships that could pose a potential conflict of interest.