

INTRODUCTION
Knee ligament injuries are one of the most common lower extremity injuries with a prevalence of 85 per 100,000 patients ranging from 16-39 years.1 While the preponderance of evidence suggests that knee ligament reconstructive surgeries are consistently successful, residual strength deficits exist from months to years after the procedures. For example, injured limb quadriceps strength has been measured at 70% of the uninjured limb six months after surgery,2 and persistent strength deficits have been observed at 24-months.3 Atrophy of the thigh musculature of the surgical limb has been reported to be present even longer, with some patients demonstrating persistent quadriceps LSI atrophy deficits at 28-months following anterior cruciate ligament (ACL) reconstruction.4 Continued quadriceps weakness has demonstrated an association with an increased fear of movement, reduced ACL-Return to Sport After Injury (ACL-RSI) scores, work absenteeism, and activity modification, among other health quality-of-life issues.5,6 To identify and mitigate strength deficits that may contribute to poor outcomes, rehabilitation professionals must perform appropriate testing and collect serial data throughout the post-operative rehabilitation process. Manual muscle testing, functional tests, one rep max (1RM), hand-held dynamometry (HHD), and isokinetic testing are potential methods to assess quadriceps strength.7 Isokinetic testing and HHD are highly correlated measures of strength and can demonstrate changes in strength over time.8 Other factors may also contribute to lingering weakness after knee surgery, including reduced central activation ratio (CAR),2,9 decreased muscle cross-sectional area (CSA),2,10 persistent pain, and the presence of joint effusion.2 Despite an understanding of these contributors, lingering performance deficits persist, so other influential components are worth examining.
Thigh circumference is a commonly gathered clinical data point intended to assess muscular atrophy.4,11,12 Utilizing a tape measure for circumferential measurements is easy, inexpensive, and widely accessible compared to alternatives like ultrasound or magnetic resonance imaging. However, protocols described in the literature for this measurement are highly variable regarding preferred patient positioning with testing (supine2,4 vs. standing9) and exact measurement location at the thigh relative to knee joint landmarks.12–15 Researchers continue to utilize thigh circumference measurements as an outcome of interest, citing a thigh bulk circumference difference of less than 0.5-1.0 cm as one indicator of adequate muscle recovery for return to prior activity level.16 To the authors’ knowledge, there is not a robust data set examining whether thigh bulk, as observed through circumferential limb measurement, is meaningfully associated with quadriceps muscle strength. This calls into question the clinical utility of gathering this data. Given that reduced CSA is related to weakness of the muscle group, it may be pertinent to examine if there is a relationship between thigh circumference and strength of the quadriceps muscle group.
The purpose of this study was to assess if a correlation exists between side-to-side difference of thigh bulk (SSD) and isometric quadriceps strength represented by limb symmetry index (LSI). The authors hypothesized that the reduction in thigh bulk SSD would mirror reductions in quadriceps LSI deficit throughout the post-operative recovery following complex knee ligament surgery.
METHODS
Participants and Procedures
Sixty-seven patients who underwent either single ligament knee reconstruction (SLKR) or multi-ligament knee reconstruction (MLKR) by one orthopedic surgeon were included in this study. Treated ligaments included the anterior cruciate ligament, posterior cruciate ligament, medial patellofemoral ligament, or fibular collateral ligament. A multi-ligament knee injury (MLKI) can be defined as tearing two or more major ligaments within the knee.17,18 Exclusion criteria included those having undergone contralateral ACL reconstruction, ACL revision surgery, graft harvest from the contralateral limb, and any previous knee surgeries on either limb. Each patient completed a testing session, which included clinical measurements and strength testing, at their six-month post-operative follow-up visit (6.47 +/- 0.79 months). The study was conducted under institutional review board approval (details blinded for submission). Testing procedures were explained to each patient and an informed consent document was signed prior to testing. Patient demographics and surgical details are presented in Tables 1 and 2.
Strength Testing
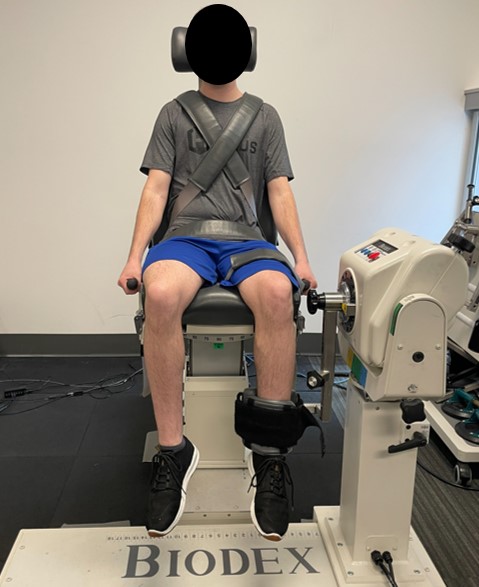
Prior to strength testing, each patient completed a standardized warm-up. An isokinetic dynamometer (Biodex Medical Systems, Inc., Shirly, NY) was utilized to perform 90-degree isometric strength testing. Patients were seated with their knee positioned with the lateral femoral epicondyle aligned with the dynamometer’s axis of rotation. Thigh, waist, and two chest straps were used to secure the patient to the chair. The dynamometer force arm was secured superior to the lateral malleolus of the ankle. Dynamometer setup is presented in Figure 1. Each patient completed a warm-up consisting of four knee extensions through their self-selected range of motion and one maximal voluntary isometric contraction (MVIC) with the force arm locked at 90 degrees of flexion to mimic the test. For assessment of isometric quadriceps limb symmetry index (LSI, %), the knee was positioned at 90 degrees of flexion. Patients were instructed to kick out with as much force as possible against the fixed arm of the dynamometer. Three maximal five-second knee extensor MVICs were executed with 30 seconds of rest between contractions. The non-surgical limb was tested first, followed by the surgical limb for all patients. The quadriceps LSI was calculated using the standard equation (LSI = surgical average peak torque / non-surgical average peak torque x 100%).

Thigh Circumference Measurement
To assess thigh circumference, patients were asked to lie supine with both lower extremities relaxed in full knee extension. The medial joint line was palpated, and a mark was placed at this location (Figure 2). A flexible, non-elastic tape measure was utilized to measure 15 cm proximal to the medial joint line where an additional mark was placed (Figure 2). At this location, the tape measure encompassed the limb with the tape measure lightly pulled taut without indenting the soft tissue (Figure 3). Thigh circumference was recorded to the nearest 0.5 cm at this point.
.png)

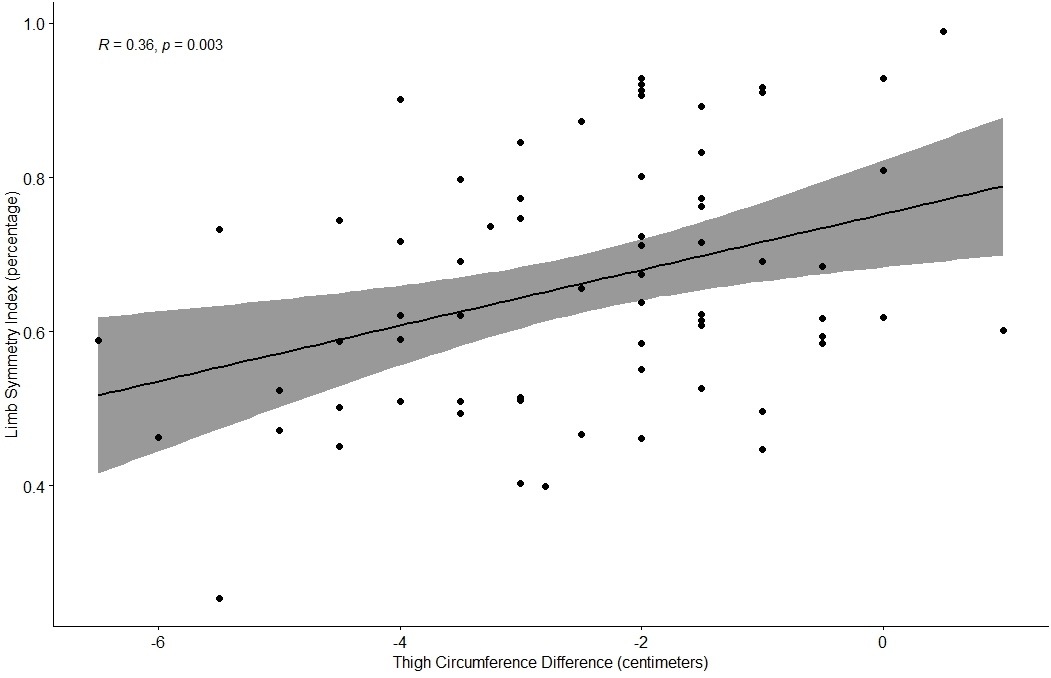
Statistical analysis was performed using R software (version 3.6.2). Pearson’s correlation coefficients were used to evaluate the relationship between thigh circumference difference and quadriceps LSI (r > 0.7 excellent; r = 0.61-0.7 strong; r = 0.31-0.6 moderate; r < 0.3 poor).Significance was set at α = 0.05 (p < 0.05) and power of 0.80 which required a minimum sample size of 36 subjects for the dataset to be adequately powered. Normality was tested using the Shapiro-Wilk Test, and a single outlier was removed from the data set.
RESULTS
This study evaluated sixty-seven patients at an average of six months status post-operatively from knee ligament surgery with a variety of demographics (Table1) and surgical characteristics (Table 2).
Subjects demonstrated a decreased mean thigh circumference of 2.53 + 1.54 cm compared to the uninvolved limb and a mean quadriceps LSI at the time of testing of 66.88 + 16.93% (Figure 4). A positive moderate relationship was found between thigh circumference difference and quadriceps LSI (r = 0.36, r2= 0.13, p = 0.003).

DISCUSSION
The most important finding of this study was that there was a moderate, positive correlation between thigh girth measurements and quadriceps LSI, with thigh circumference accounting for 13% of quadriceps LSI deficit. Quadriceps weakness and side-to-side thigh bulk asymmetry persist following ACL reconstruction despite an emphasis on focused post-operative quadriceps strengthening after knee ligament surgery.2–4
Thigh circumference has been used as one of multiple criteria for assessment of adequate muscle strength and an athlete’s readiness for return to unrestricted sports participation following ACL reconstruction. Barber-Westin and Noyes16 performed a systematic review of 264 studies in which 25 utilized muscular strength and three incorporated thigh circumference (girth) assessment as return to sport criteria.2 While thigh circumference has historically been accepted as an indirect measurement of muscle atrophy and/or hypertrophy, no studies have established a direct relationship between thigh circumference and muscle size.15
This study was focused on the relationship between thigh circumference SSD and quadriceps LSI. However, quadriceps muscle girth only accounts for 13% of thigh bulk, with CSA of other large muscles of the thigh, adipose tissue, and limb edema being other potential contributors to circumferential bulk. Multiple authors have reported that thigh circumference underestimates muscle atrophy and does not adequately represent muscular strength.9,10 Hamstring muscular atrophy is often overlooked as a contributing factor to thigh girth SSD4; however, the existing literature continues to report mixed results regarding the influence of hamstring atrophy in association with thigh circumferential measurement.4,19,20 To the authors’ knowledge, no previous studies have assessed the effect of other muscle groups on thigh circumferential measurements.
Graft type, sex and concomitant injuries, i.e. meniscal injury, are other potential influential factors on thigh circumference, strength, and muscular atrophy. Within the current study, those factors were not grouped or analyzed separately. Hamstring strength deficits of 2% to 10% have been observed at six-and-twelve- months following ACLR with a patellar tendon autograft.19 Patients undergoing ACLR with a hamstring tendon autograft demonstrate persistent thigh atrophy an average of 28-months post-operative likely correlated to both hamstring and quadriceps atrophy.4 Based on the findings above, thigh circumferential measurement assesses the volume of multiple tissues, not just the thigh extensor mechanism. When measuring quadriceps strength, thigh circumference also considers CSA differences in other musculatures.
The current study utilized isometric dynamometry testing to assess muscular strength. Isometric strength testing has demonstrated good reliability21 and a reduced ACL strain when testing at angles of 60 degrees or greater.22 In comparison, previous studies have utilized isokinetic testing at multiple knee flexion angles and speeds10,23 to assess muscular strength, therefore methodological inconsistencies throughout research continue to be present.9,24
There are several limitations to this research. First, thigh circumference was measured supine with the quadriceps muscle relaxed. When the muscle is relaxed, this could result in a difference compared to when the muscle is contracted. Otzel et al.9 measured thigh circumference in standing with the quadriceps muscle contracted. Additionally, the locations where thigh circumference were measured may not demonstrate valid circumference measurements. In the current study thigh circumference was measured 15 cm proximal to the medial joint line. Previous studies used the superior pole of the patella as a starting point. Measuring from the proximal patella presents its own limitations because patellar position may be altered by surgery type, post-surgical stiffness or scarring, and quadriceps contraction.
Measuring circumference 15 cm proximal to the medial joint line may not be proximal enough to look at true thigh bulk, while 20 cm proximal to medial joint line is often too high for patients with shorter limbs. Other factors that may contribute to the loss of thigh circumference and/or strength such as decreased neural input, fat/muscle mass differences, and/or arthrogenic muscle inhibition (AMI) were not assessed during this study. Future studies may benefit from determining how other factors account for the loss of thigh circumference, and/or strength, i.e. assessing hamstring bulk, NWB vs. WB patients, as well as if there is a difference threshold required to determine if a relationship between quadriceps LSI and thigh circumference exists.
CONCLUSION
The results of this study indicate that a moderate positive correlation exists between thigh girth SSD and LSI, therefore consistently measuring thigh girth may assist clinicians in monitoring strength differences side to side. Thigh circumference only accounts for approximately ~13% of all factors that influence quadriceps LSI, therefore it is important to consider use of a battery of different tests and measures to properly assess muscular strength following knee surgery.
Conflicts of interest
The authors certify that there are no conflicts of interest or financial disclosures in relation to this paper.
Acknowledgements
We would like to take the time to thank Twin Cities Orthopedics doctors, surgeons, and patients, as well as Becky Stone, JW Matheson, and Jake Foley for their involvement with this research project.