
INTRODUCTION
Ambidextrous pitching, or “switch pitching”, is a rare phenomenon where a pitcher can effectively throw with both their dominant arm and nondominant arm. This ability can allow for a pitcher to change their throwing arm depending on the athlete up to bat, which can provide a strategic advantage, throw off the hitters timing, and create difficulties for opposing teams. This can also potentially allow for a pitcher to switch arms if needed due to physical limitations or injuries that have occurred on one side but not the other. However, ambidextrous pitchers may experience unique biomechanical injury risks compared to normal pitchers, which require special physical training and medical monitoring to ensure safety and decrease potential overuse injuries.1 Consequently, there is a significant gap in the literature regarding the mechanical and clinical profiles of ambidextrous pitchers, including how their bilateral throwing patterns influence musculoskeletal development, injury risk, and performance potential. Furthermore, the youth demographic presents added complexity due to ongoing physical maturation, making it critical to track changes over time. While switch pitching is still relatively new and uncommon in baseball, its potential implications for player development and injury prevention remain under-investigated, particularly in the youth demographic.2,3
The purpose of this case report is to describe key biomechanical and clinical differences between the dominant and nondominant throwing arms of a youth ambidextrous baseball pitcher across three timepoints using a multidisciplinary approach. By illuminating the key differences and similarities between dominant and non-dominant pitching mechanics, the authors aim to provide valuable insights into the biomechanical demands placed on a youth ambidextrous pitcher and identify changes in these quantifiable features over the course of time and development. It was hypothesized that both age-related changes and arm-to-arm differences would be observed in the athlete’s anthropometric and biomechanical measurements.
Subject Presentation and Training Background
The subject of this case report was an ambidextrous youth baseball pitcher who underwent evaluations at ages 11, 12, and 14. The following details regarding the subject’s history were provided by a parent. At the age of two, the athlete was introduced to a baseball glove for the right hand and initiated throwing with the left hand. Throughout subsequent years, the subject exclusively used the left hand for throwing whiffle balls and tennis balls. However, at the age of six, while playing catch with a football, it was observed by the parents that the athlete could achieve greater throwing distances with the right hand compared to the left. Although the athlete exhibited similar physical capabilities in both hands, it became evident to the parents that the right side was dominant. Nonetheless, the athlete maintained bilateral training to ensure uniformity between both left and right sides. During practice sessions, the athlete adhered to a regimen of alternating throws between the left and right hands, completing five throws with each hand in succession to achieve comparable repetition on both sides.
The athlete commenced speed and agility training at approximately 11 years of age, adhering to a regimen that emphasized bilateral development. Additionally, the incorporation of weighted balls into the warm-up routine commenced around the ages of 10 to 11, complemented by stretching exercises targeting both sides of the body. The athlete also initiated strength and conditioning training at approximately 12 to 13 years old. However, progress was interrupted by a non-baseball-related right arm injury sustained at the age of 13, which precluded the resumption of strength and conditioning activities up to the time of the beginning of this case report. During competitive engagements, the parent noted inconsistency in the athlete’s utilization of the dominant and non-dominant arms, contingent upon the circumstances of each scenario. For instance, while fielding in the outfield, the athlete predominantly employed the right hand for throwing, yet when assuming the role of pitcher, the athlete predominantly pitched with the left hand. Similarly, the athlete alternated between throwing left-handed while playing first base and pitching right-handed when called upon to pitch. This inconsistent throwing pattern at times resulted in insufficient warm-up before pitching, which the athlete reported as adversely affecting performance on the mound.
MATERIALS AND METHODS
The athlete was consented, and a human subject’s review board consent form (IRB Protocol #0524-21-EP) was signed by the participant’s guardian and reviewed by the athlete in accordance with standard policies. The athlete was evaluated on three separate occasions, when he was 11, 12, and 14 years of age, and the evaluations were completed in the Sports Medicine and Biomechanics Research Lab at the University of Nebraska-Omaha. The evaluation began with a clinical assessment carried out by a team of certified athletic trainers. The clinical assessment included passive ROM measurements for structures including shoulder external and internal rotation, hip internal rotation, and hamstring flexibility via the 90/90 straight leg raise test (SLR). All measurements were acquired with a goniometer and were recorded in degrees (°). The second part of this case report was conducted by a team of experienced sports biomechanists and focused on a detailed biomechanical assessment of the ambidextrous pitching motion, utilizing motion capture techniques to dissect the kinetic and kinematic aspects of pitching from both arms. Outcome measures for this section included: pelvis rotation at stride foot contact (SFC) (°), trunk rotation at SFC (°), shoulder horizontal abduction at SFC (°), shoulder rotation at SFC (°), max normalized shoulder force (% body weight - %BW), max non-normalized shoulder force (Newtons - N), max normalized elbow varus torque, and max non-normalized elbow varus torque (newton meter - Nm). Ball velocity (miles per hour - MPH) was also measured with a radar gun (Stalker Sport 2, Stalker Sport, Richardson, Texas, USA).
Clinical Evaluation
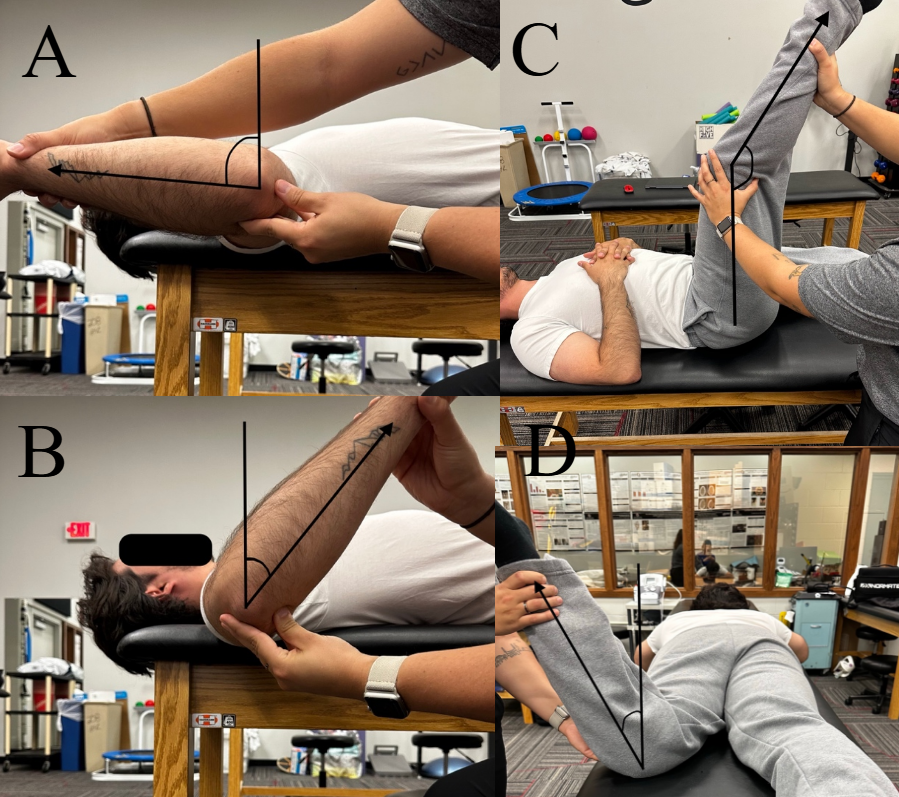
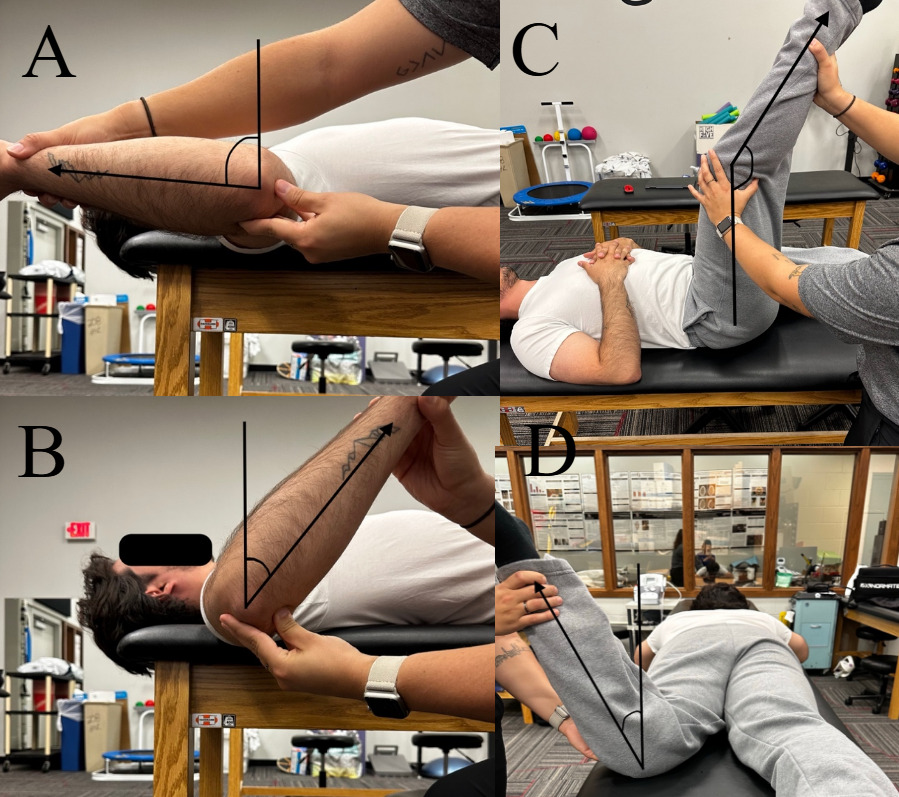
For shoulder external and internal rotation, the athlete was instructed to lie supine on the table with their body shifted towards the outside of the table of the arm being currently measured.4 The clinician passively took the arm and supported it in 90° of shoulder abduction and the wrist in supination and forearm facing upwards in the air with the elbow at 90° of flexion.5 From there the clinician then passively externally rotated the arm until the shoulder or scapula tried to lift off the table while maintaining the shoulder at 90° of shoulder abduction and elbow at 90° of flexion (Figure 1a). The same process was used for internal rotation in the opposite direction (Figure 1b). For the external rotation measurement, the anterior shoulder was stabilized to help isolate glenohumeral contribution. The goniometer was placed on the lateral aspect of the elbow at the olecranon process with the stationary arm straight up in the air perpendicular to the table and the moving arm along the forearm, aimed at the styloid process of the ulna. Once an end point was found, the goniometer measurement was recorded for both internal and external rotation for both arms. These measurements were used to calculate the total arc of motion of both arms and the difference between the dominant and nondominant arms (total arc difference).6
For hamstring range of motion, the 90/90 SLR test was used.7 While the patient is lying supine, the clinician passively flexed the hip to 90 degrees and then extended the knee as far as possible and placed the axis of the goniometer on the lateral aspect of the knee joint center (Figure 1c). The stationary arm was placed along the femoral shaft aimed at the greater trochanter and the moving arm along the fibular shaft aiming at the lateral malleolus. For hip internal rotation, the athlete was placed in a prone position on the table with their knee passively bent to 90° while hip remained neutral.8 The clinician then passively moved the lower leg outwards while the knee was bent at 90° and the pelvis still level with no contralateral lift off the table. Once the contralateral hip started to lift off the table, passive movement was stopped, and the hip internal rotation angle was measured (Figure 1d). The goniometer was placed inferior to the bent knee with the stationary arm parallel with the table and the moving arm along the tibial shaft, aiming at the bisection of the anterior tibiofibular joint.
Biomechanical Evaluation
At each testing session, the athlete was fitted with 41 retroreflective markers (Qualisys PAF Baseball Mac Marker Set, Appendix A) for motion capture analysis (Qualisys, Gothenburg, Sweden). Kinematic data were collected at 240 Hz at ages 11 and 12, and 320 Hz at age 14. The difference in capture rate was due to a change in equipment in the lab between separate evaluations. The laboratory pitching mound was instrumented with three force plates (Bertec, Columbus, Ohio, USA), one underneath the pitching rubber and two in the stride foot landing zone. Following a self-selected warm-up of the right arm, the athlete completed four pitches of each of the pitch types with the right arm. The athlete then completed a self-selected warm-up on the left arm before repeating the previously mentioned data collection process. The pitching lane was the league-appropriate length at 15 m,3 and consisted of throwing the ball into a 9-hole pitching net.
Data Processing
Markers were labeled using the Qualisys Track Manager (QTM) application. Gaps in position data were filled in QTM using a relational fill. Marker position data was exported to Visual3D (HAS Motion, Kingston, ON, Canada) to generate model-based data for each segment. Kinematic measurements of interest were shoulder horizontal abduction, shoulder internal/external rotation, pelvis rotation about the z-axis and trunk rotation about the z-axis. Kinetic measurements of interest were maximum shoulder distraction force and maximum elbow varus torque. Kinetic measurements were calculated both with and without normalization to the athlete’s bodyweight.
Biomechanical data were observed between the temporal parameters of setup and 100 milliseconds after ball release. Setup was an event defined automatically by Qualisys as the time when the front heel marker exceeded a vertical velocity of 0.02 m/s with an offset by -1 frame. Ball release was defined manually by observing 2-dimensional videos as the first frame where the ball was not in contact with the athlete’s hand. Measurements were taken for each pitch during the specified time frame and were interpolated into 101 data points. The evaluation at age 11 consisted of two fastballs for each arm and all subsequent evaluations took measurements from three fastballs. A representative data set was calculated for each evaluation by averaging the measurements for all pitches thrown with the same arm. Measurements during the pitching sequence at either stride foot contact (SFC) or the maximum value were obtained. The normalized shoulder force values are normalized by body weight (in N), while the normalized elbow varus torque values are normalized by body weight (in N) multiplied by height.
Due to this being a case report, comparisons were made between the athlete and literature-based normative kinematic and kinetic values.9 Diffendaffer et al. completed a clinical review of the literature related to baseball pitching biomechanics and compiled the results into a set of normative values that are used to evaluate the health and safety of a pitcher’s biomechanics. The literature used in their review included data from high school, collegiate, and professional pitchers. Though the subject of this case report is a youth pitcher, Fleisig et al.10 found no significant differences between the kinematic measurements of pitchers of all ages (youth, high school, college and professional). Therefore, recommendations can reasonably be made for a youth pitcher based on normative values collected on higher-level pitchers for kinematic measurements. Despite no significant differences in kinematics between increasing levels of competition, Fleisig et al. did find significant differences in non-normalized kinetic measurements.10 Therefore, comparisons to normative kinetic values must be made to the player’s age group (Table 1).
OUTCOMES
Clinical Outcomes
Over the duration of this case report the athlete grew approximately 20 cm and gained 16 kg across the three evaluations at age 11 (height=157.5 cm, mass=54.4 kg), 12 (height=160.0 cm, mass=55.8 kg), and 14 (height=177.8 cm, mass=70.3 kg). Shoulder external rotation passive ROM measurements varied throughout the three evaluations, with the most recent evaluation the right shoulder with greater shoulder external rotation than the left (11° difference). Both left and right shoulder internal rotation consistently decreased across the three evaluations with the left side decreasing 23° and the right side 24°. The total arc difference between sides was larger at the 11- (12°) and 12-year-old (19°) evaluations, while at the 14-year-old evaluation was close to negligible (2°). The hamstring and hip internal rotation measurements were consistently greater in the right leg compared to the left leg and were variable between the three evaluation sessions (Table 2).
Biomechanical Outcomes
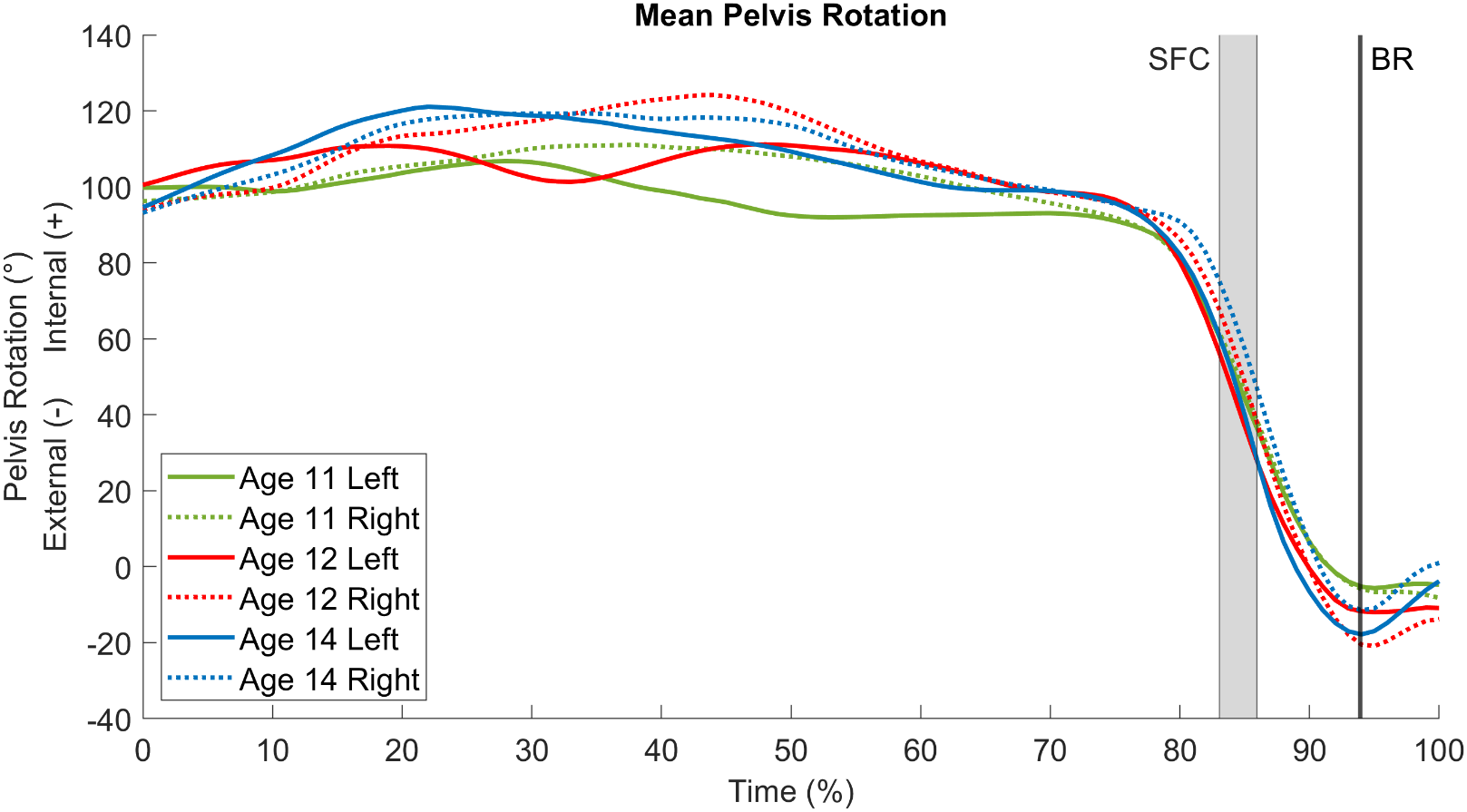
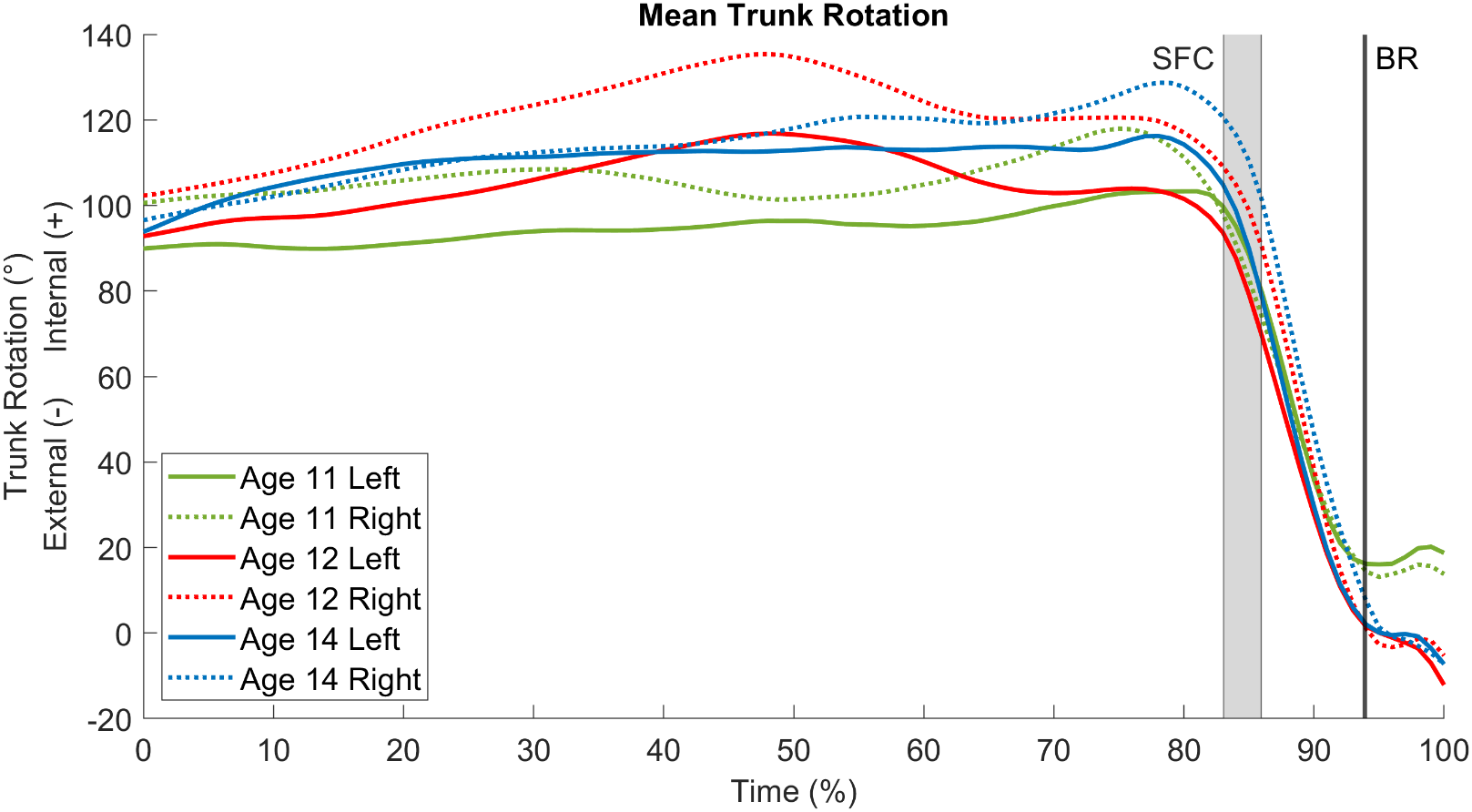
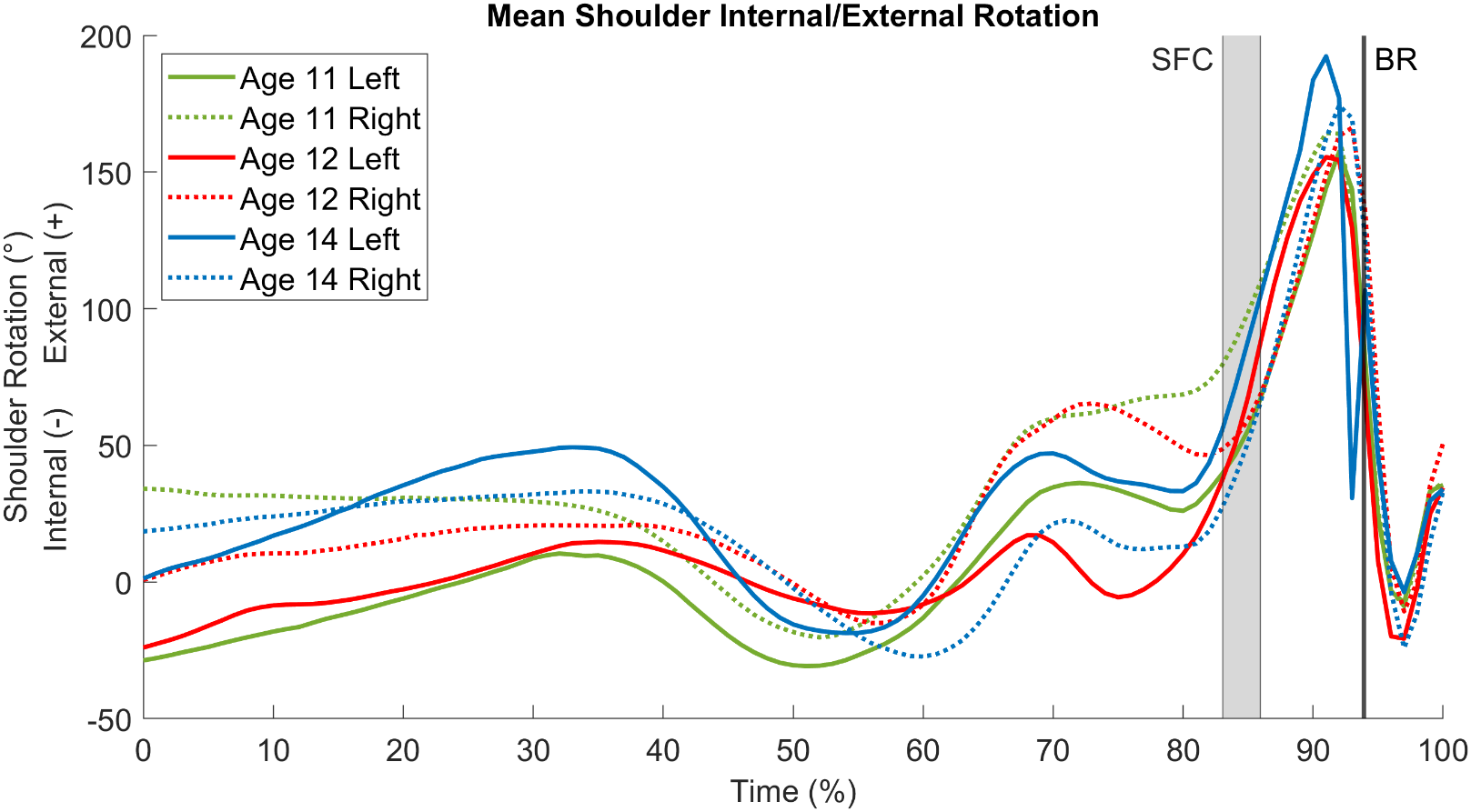
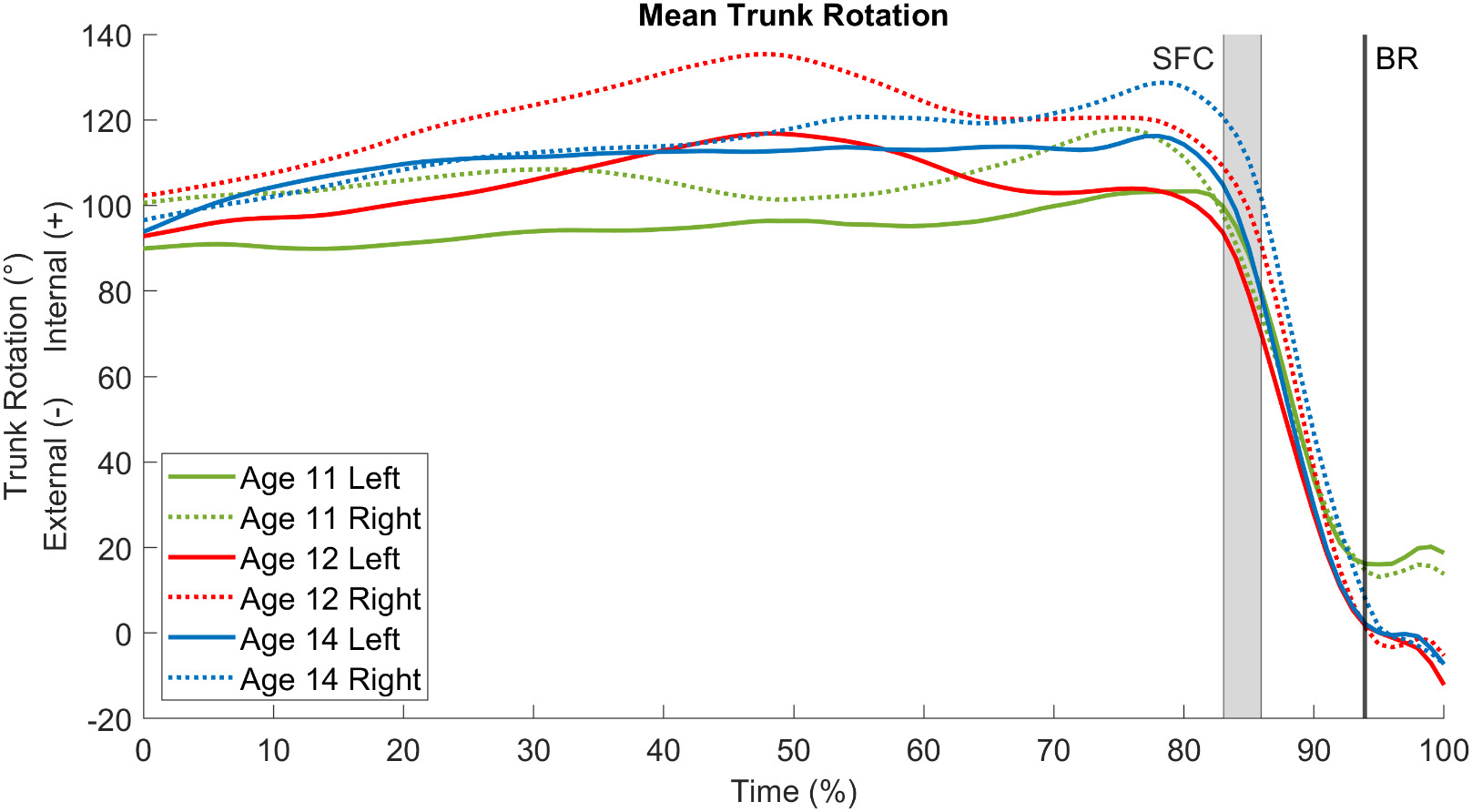
The results of the biomechanical analysis for each evaluation are presented in Table 3 and Figures 2 –7. The black line in each of the figures denotes when ball release occurred during the pitch which occurred at an average time of 94% of the time between setup and 100ms after ball release. The relevant temporal parameter was SFC and the maximum values for the kinetics were collected. SFC varied between pitches and evaluations, so SFC was reported as a range of values. This range was found to be between 83% and 86% of the time between setup and 100 ms after ball release and was shown in the figures by a gray shading. The biomechanical results demonstrated notable variations in the parameters across the three evaluations. Pelvic rotation at SFC increased approximately 23° on both the left and right sides, along with an increased in trunk rotation at SFC of 40° on the right side and 28° on the left. At the initial evaluation, shoulder rotation at SFC was greater on the right side (112.4°) compared to the left side (76.5°) but by the third evaluation, the left side (68.2°) was greater than the right (46.5°). From the initial to the last evaluation, max normalized shoulder force increased by 507.4 N on the right arm and 225.5 N on the left, max non-normalized elbow varus torque increased by 30.7 Nm on the right arm and 12.7 Nm on the left, and average ball velocity increased by 12 MPH when pitching right-handed and 11 MPH when pitching left-handed.
DISCUSSION
Clinical Measurements Discussion
This case report examines a unique case of a youth ambidextrous baseball pitcher who underwent three separate biomechanical and clinical evaluations spanning across four years. Longitudinal evaluation of this ambidextrous pitcher revealed side-to-side differences and developmental adaptations, reflecting how mechanics may change as an athlete matures and refines their pitching technique over time. There is a study that evaluated and measured youth and adolescent baseball players ROM to provide normative values through the aging process.11 Meister et al. evaluated shoulder internal rotation and external rotation, along with total arc ROM in youth athletes ranging between the ages of 8 and 16.11 Comparison with normative values from Meister et al. revealed notable differences and trends in the subject’s measurements (Table 4). Although similar measurement techniques were used, the subject demonstrated greater shoulder internal rotation and reduced external rotation compared to reported normative values. This pattern may be due to the athlete’s bilateral throwing exposure, which likely reduced the repetitive overload typically seen in unilateral pitchers that contributes to increased external rotation and decreased internal rotation. Developmental factors such as growth stage, bony anatomy, or limited throwing volume may have also played a role.
The total arc measurements showed similar trends to the values from Meister et al. demonstrating a decrease in total arc over the course of the three evaluation sessions.11 In baseball players, shoulder external rotation is typically greater than internal rotation, with the total arc of motion typically measuring near 180°.12 Pitchers with limited total arc ROM has been noted as a risk factors for shoulder injury, including those with total arc below 160°.5 During the athlete’s last evaluation, the total arc measurement for the left arm decreased compared to the second evaluation, diminishing by 28°, putting the athlete closer to the 160° injury risk threshold.5 But when compared to the right arm that same evaluation, the total arc difference between arms was only 2º compared to the last two evaluations, where the arc difference was 12° and 19°. In healthy pitchers, the total arc of motion between shoulders is generally not significantly different.5 However, external rotation in the throwing shoulder is greater than the non-throwing shoulder, while internal rotation in the throwing shoulder is significantly less than in the nonthrowing shoulder.13 Thus, the next question may be, since the athlete is ambidextrous, which is more important or influential on performance and injury risk, total arc for each arm or total arc difference between arms? Further research is needed investigate the intricacies of total arc ROM and total arc differences between shoulders in ambidextrous pitchers and its influence on or correlation with biomechanical performance and injury risk.
Meister et al. suggested that the decrease in total arc may be due to the consequences of bone and soft tissue adaptation with age, but it has not been discerned whether these changes occur due to adaptive or developmental origins.11 Crocket et al. suggested that there are specific bony adaptations that can be capable of change in skeletally immature athletes like increased humeral head retroversion that can cause alterations in internal and external rotation range of motion of the shoulder, decreasing and increasing respectively.14 Other authors have suggested that alterations in ROM in the shoulder may result in increased risk of shoulder impingement of the rotator cuff and labrum-involved pathologies.15 Other authors suggest that changes in shoulder ROM can be adaptive due to training and exercise.16 In adults, shoulder adaptive changes in response to overhand throwing have been observed, but the age of onset has not been established.17 Overall, the explanation as to why there is a trend of decreasing total arc of ROM has not been made clear. The subject of this case report did not mention any symptoms of shoulder pain, thus it is possible that the changes in total arc could be due to adaptations during aging or from strength training.
Limited hamstring flexibility can disrupt the efficiency of the kinetic chain, reducing force transfer from the lower extremity to the upper body. This compensation may increase reliance on the shoulder and elevate stress on the throwing arm, potentially raising injury risk.12 One important factor in pitching is stride position, which refers to the stance taken by the pitcher as they step forward with their lead leg during the pitching motion. This is a crucial component in pitching mechanics as it contributes to generating power aimed towards the plate and can affect pitch velocity.9 When hamstring flexibility is limited, it can reduce the transfer energy from the lower body to the upper body, affecting the ability to generate velocity when pitching. Phrathep et al. reported average hamstring measurements for the right and left legs of this age group to be approximately 140° and 139.7° respectively.6 The subject’s values were consistently above this average on the right leg, and above average on the left leg at two of the three time points. The reason for this discrepancy between limbs is unclear, but it may reflect asymmetries in lower extremity use or mobility focus during training. Alternatively, it may simply represent natural variation, as side-to-side differences in flexibility are not uncommon in youth athletes.
Lastly, passive internal rotation ROM of the hip is important for pitching because it assists in rotational force generation from the lower body, which affects pitching velocity. Internal hip rotation enables the pitcher to engage muscles like the glutes, hip adductors, and hip rotators, which contributes to the overall stride length and facilitates the efficient transfer of energy from the lower body to the upper body.18 The athlete’s hip IR was observably higher on the right side compared to the left side during the first evaluation but got within 6° by the final evaluation. This may or may not be a training adaptation over time, imbalanced pitch counts bilaterally, or a soft tissue/bony adaptation from aging. Tajika et al. noted the average hip internal rotation for their study of adolescent baseball pitchers showed a dominant leg average of 49.8°±10.8°, which puts our athlete right within the average for latest measurements.19
Biomechanics Discussion
Pelvic rotation at SFC plays a critical role in generating momentum and enabling effective trunk and arm sequencing during the pitching motion.9,10 In this case, pelvic rotation values worsened over time, as the subject’s pelvis became more closed off from the first evaluation to the last evaluation for both the right (by 23.7°) and left (by 23.4°) sides (Figure 2). Limited pelvic opening at SFC, particularly on the right side, may reflect delays in segmental timing or mechanical inefficiencies, which can alter energy transfer up the kinetic chain. This may place additional stress on the upper extremity to compensate for lost power from the lower body and thus increase the risk of injury.9 Given the bilateral nature of this athlete’s workload, asymmetries in pelvic rotation could also suggest uneven development of trunk and hip control between arms. These findings highlight the importance of monitoring rotational mechanics as part of a comprehensive assessment.

Trunk axial rotation at SFC is essential for effective energy transfer through the kinetic chain and helps to optimize timing between the pelvis, trunk, and throwing arm. Inadequate trunk rotation disrupts kinematic sequencing, reduces performance, and increases stress on the shoulder and elbow joints.9 The athlete displayed inadequate trunk rotation for both arms at the first evaluation, was informed about the deficits and given drills to generate more rotation. Following targeted training recommendations after the first evaluation, the athlete displayed improvements in trunk rotation for both of their arms (Figure 3). These changes likely reflect both improved motor control and increased core strength, contributing to more efficient mechanics. The observed improvements highlight the importance of trunk timing in youth pitchers, particularly for those with bilateral workloads where asymmetries may emerge or be exaggerated without focused intervention.
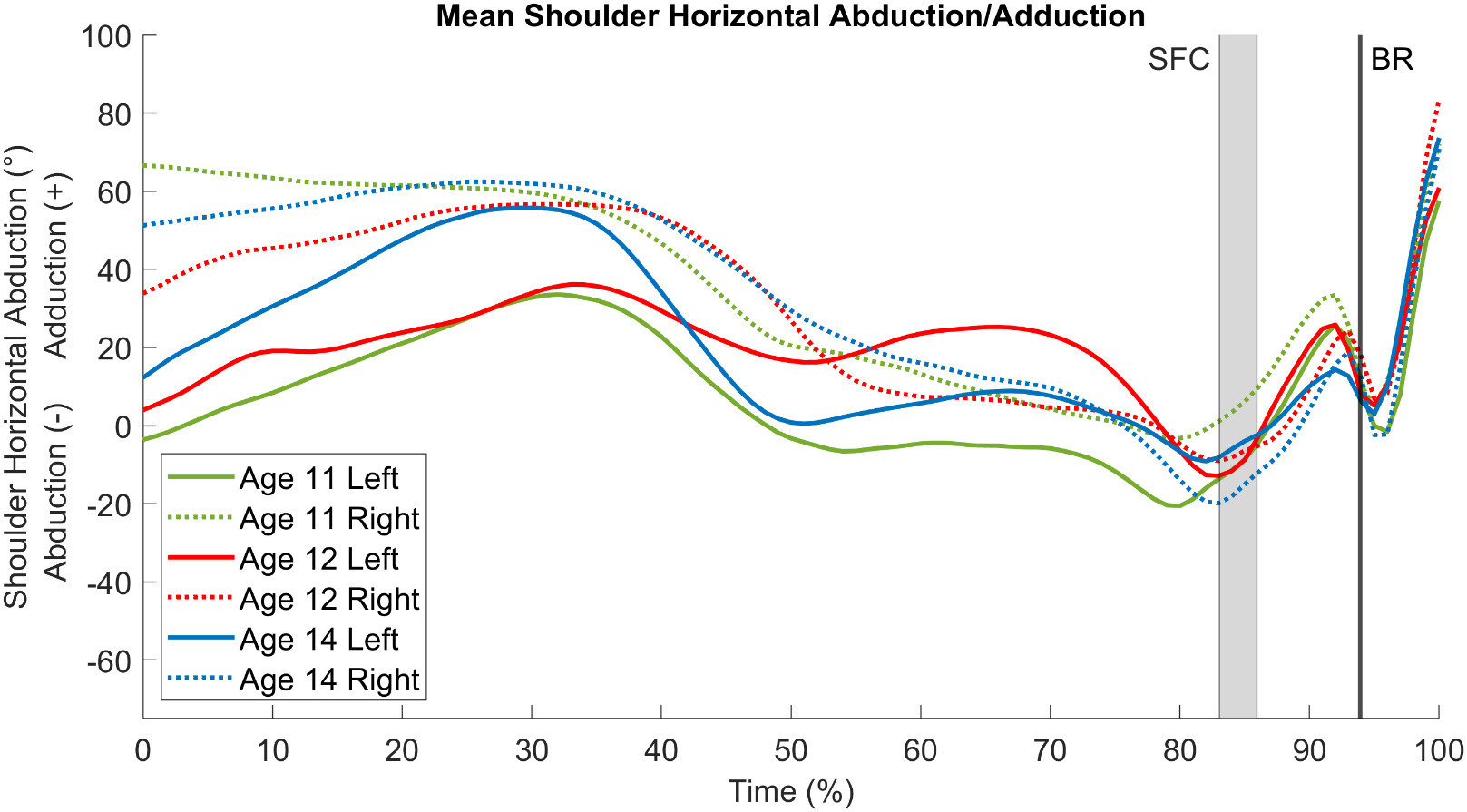
It is recommended that pitchers make SFC with shoulder horizontal abduction of -20°.9 Excessive horizontal abduction can lead to tensile tears in the anterior glenohumeral capsular ligament,9,20 and lack of horizontal abduction is associated with decreased velocity.21 In this case, early evaluations revealed inadequate horizontal abduction in both arms, with the right arm particularly lacking due to adduction at SFC (Figure 4). The athlete’s left arm displayed better abduction than the right side but was still below the recommended value and showed high amounts of variance. Over time, the right arm showed notable improvement, suggesting better mechanical timing or flexibility gains. Conversely, the left arm failed to improve and even showed slight regression, despite being closer to the recommended range initially. This highlights the importance of tracking each arm separately, as improvements may not occur equally in ambidextrous pitchers.
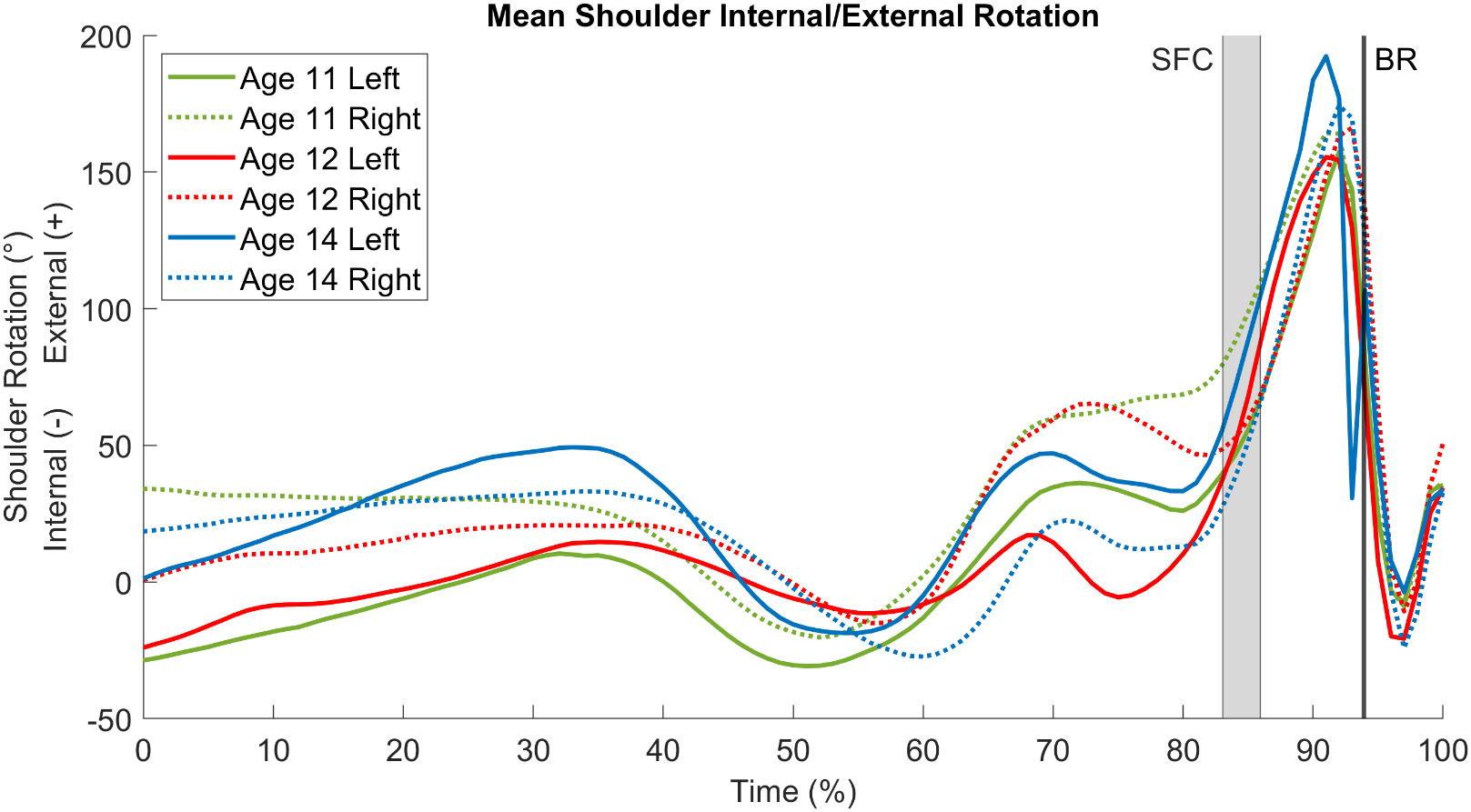
One of the primary movements of a pitcher’s arm during the pitching sequence is shoulder external rotation.9 A certain amount of external rotation is required at SFC, as insufficient shoulder external rotation, or a “late arm action”, has been correlated with elevated elbow stress.9 Early evaluations showed excessive external rotation in the right arm, possibly due to early arm positioning or poor trunk-arm sequencing. Over time, external rotation in the right shoulder decreased toward the recommended range but showed variability that could suggest timing inconsistencies (Figure 5). The left shoulder initially showed insufficient rotation, consistent with a late arm action, but improved by the final evaluation. These patterns reflect asymmetrical adaptation, a common challenge in ambidextrous pitchers.
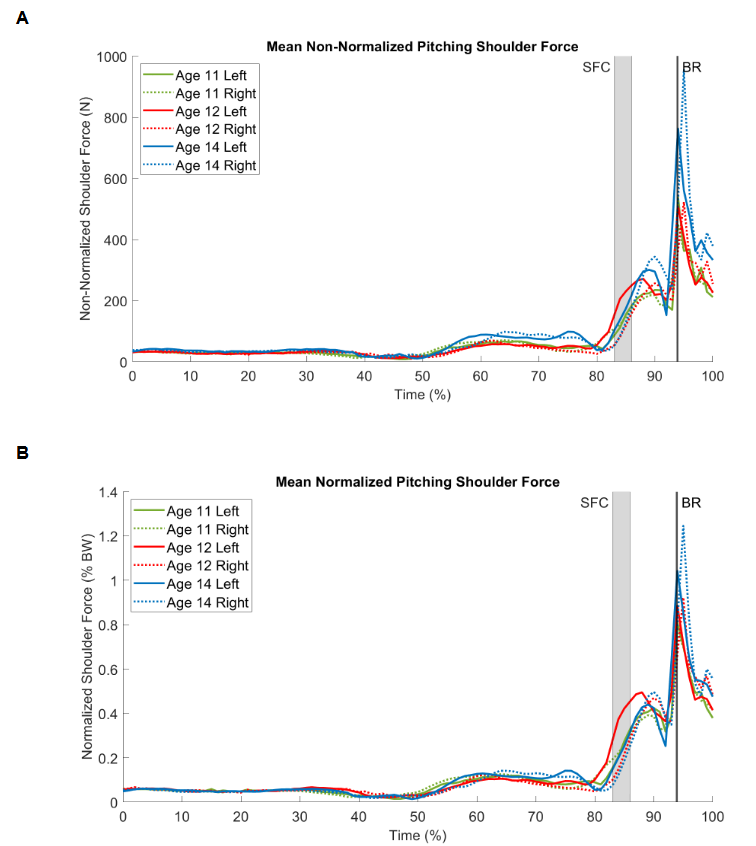
To the authors’ knowledge, there have been no peer-reviewed studies that establish normative values for the forces experienced by the shoulder and elbow. Therefore, only the trends for shoulder distraction force and elbow valgus torque will be reported, in addition to the values reported in Table 3. As the athlete matured from the first evaluation to the last, the distraction force experienced by the right shoulder increased by 507.4 N (Figure 6A), which is a percent change of 113%. When normalizing by body weight, right shoulder distraction force increased by 48.4% BW (Figure 6B). For the left shoulder, distraction force increased by 225.5 N, corresponding to a 24.2% BW increase. The implications of these values are unknown due to the lack of literature on normalized values. These increases in shoulder distraction force with ageing is consistent with previous research.3 It is speculated that these increases in shoulder distraction force may be a result of the athlete’s enhanced ability to generate power and transfer energy through the kinetic chain due to improvements in overall strength and body composition. However, if these increases are not accompanied by proportional improvements in shoulder strength, mobility, and recovery capacity, they may elevate the risk of overuse injury.3,10
_and_normalized_(b).png)
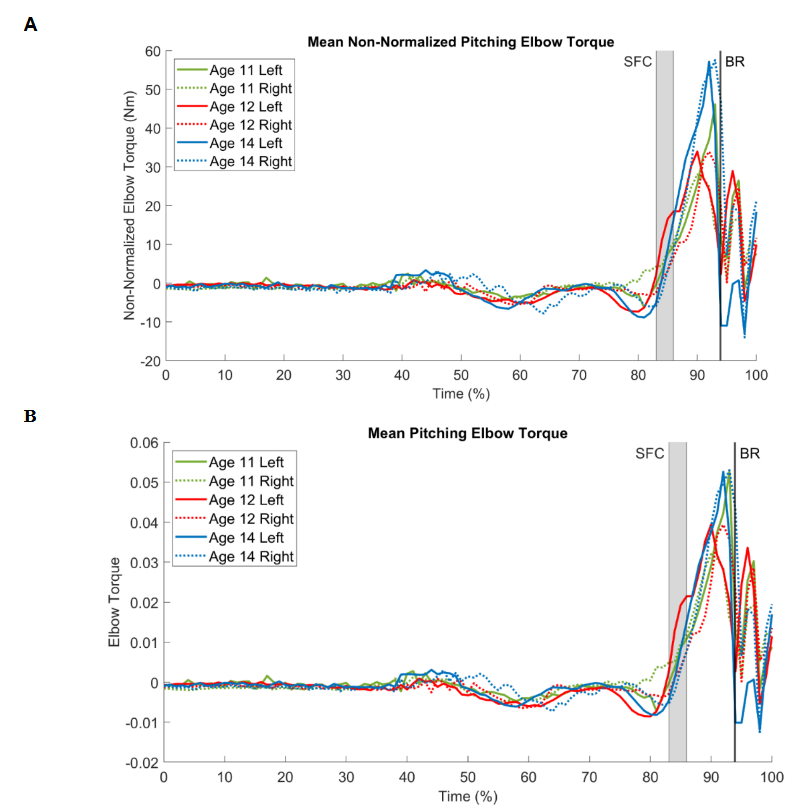
In this case, elbow valgus torque increased over time in both arms, with peak values observed at the third evaluation (Figure 7A). While raw (non-normalized) torque values rose steadily, normalized values remained stable between the first and second time points, likely due to proportional gains in body mass, as normalization accounts for height and weight (Figure 7B). A modest increase in normalized torque by the third evaluation may indicate that mechanical loading began to outpace physical growth. Although the clinical significance remains unclear due to the lack of normative data in youth pitchers, the continued rise in torque warrants attention. In the absence of symptoms, these changes may represent normal adaptation; however, they underscore the importance of monitoring kinetic trends over time, particularly in ambidextrous athletes managing bilateral workloads.
Lastly, inspection of average fastball velocity revealed that the pitcher consistently threw faster with the right arm compared to the left. Overall, pitch velocity increased with age, apart from the left arm at age 12, which remained similar to the velocity recorded at age 11. The increase in velocity over time is likely attributable to a combination of factors, including physical growth, increased strength, improved neuromuscular coordination, and refinement of pitching mechanics, all of which contribute to more efficient energy transfer through the kinetic chain.
_and_normalized_(b).png)
As a single-subject case report, these findings are not generalizable to all ambidextrous or youth pitchers and it is not possible to draw any cause-and-effect conclusions. Changes in clinical and biomechanical measures may reflect a combination of biological maturation, training exposure, and inconsistent arm use that were not fully controlled. Normative comparisons were based on data from unilateral pitchers, which may not accurately represent the demands of bilateral throwing. Additionally, the absence of detailed workload tracking and the potential for minor measurement variability may have influenced results. Given the rarity of ambidextrous athletes, especially in youth populations, future research should aim to establish normative biomechanical benchmarks, investigate side-to-side adaptations in greater depth, and evaluate how bilateral throwing impacts injury risk and performance outcomes over time. Longitudinal studies with larger cohorts and structured workload monitoring are especially needed to inform best practices for training and injury prevention in this unique population.
CONCLUSION
This case provides a rare longitudinal perspective on a youth ambidextrous pitcher, offering insight into bilateral development and adaptations not typically captured in existing literature. Ambidextrous pitchers are uncommon, and limited research compares biomechanical and clinical differences between arms. This athlete demonstrated both improvements and regressions in the assessed variables over time, with some measures aligning more closely with recommended performance and safety benchmarks, while others deviated. Given the bilateral demands of ambidextrous pitching, these athletes may be at increased risk of biomechanical fatigue due to cumulative stress placed on both the upper and lower extremities. The observed changes reflect developmental adaptations that may influence performance capacity and injury susceptibility. Regular clinical and biomechanical assessments are essential to monitor asymmetries and guide individualized strategies that support long-term health and performance in this unique population.
Corresponding author
Adam B. Rosen PhD, ATC
arosen@unomaha.edu
6001 Dodge St
H&K207Y
Omaha, NE, USA. 68182
Conflict of Interest Statement
The authors report no conflict of interest.
ACKNOWLEDGEMENTS
The authors want to thank several people who contributed to the data collection and interpretation over the course of the three evaluations. We want to thank: Tyler Hamer, Ph.D, Tomohiro Ide, MA, LAT, ATC, Colleen Vogel, MS, ATC., and Takato Ogasawara, MS.