INTRODUCTION
The glenohumeral joint is a complex ball and socket joint made to provide maximum mobility with minimum stability.1,2 This unique anatomical configuration makes it particularly susceptible to injury. Shoulder-related issues affect a significant portion of the general population, with reported rates reaching as high as 26%.3,4 In fact, the shoulder is known to be the third most commonly injured joint in overhead sports, including but not limited to baseball, handball, badminton, and volleyball.5–7 Shoulder injuries have also been classified as the second most common overuse injury.8,9
While previous studies have largely focused on shoulder asymmetry in baseball players, the biomechanics and kinematics shared between baseball and volleyball provide valuable insights into potential injury factors for volleyball athletes.8,9 One aspect that all overhead sports have in common is that they require repetitive, high-velocity movements that place stresses on the shoulder joint leading to adaptive changes.10 These repetitive motions especially seen during spiking and serving are known to develop a decrease in shoulder internal rotation, known as glenohumeral internal rotation deficit (GIRD) and an increase in external rotation, known as external rotation gain (ERG).11–14 The concept of loss in internal rotation and gain in external rotation is seen as a necessary adaptation for the sport, it only becomes problematic when the loss is not proportional to the gain leading to a loss of total motion arc.15–17
In their clinical commentary, Manske et al. divide GIRD into anatomical and pathological subtypes by defining standards for Anatomical Glenohumeral Internal Rotation Deficit (aGIRD) as a loss of internal rotation between 18 and 20 degrees while maintaining symmetrical total range of motion (TROM) in both arms.18 Pathologic Glenohumeral Internal Rotation Deficit (pGIRD), on the other hand, is characterized by a significant loss of glenohumeral internal rotation, surpassing 18-20 degrees, and a concomitant deficit of more than 5 degrees in TROM when comparing both arms. Within the same commentary, Manske et al. also mentioned that GIRD may also be classified as pathological regardless of the amount of internal rotation deficit if the TROM difference of the shoulder shows asymmetry larger than 5°.18
Presently, pGIRD is recognized as a contributing factor to injury risk and has been associated with conditions such as rotator cuff tears, internal impingement, and glenohumeral joint instability.19 Recent research by Manske et al. has identified distinct sub-types of GIRD, classifying it as either aGIRD, a normal adaptation in overhead athletes, or pGIRD, which is associated with increased injury risk and shoulder dysfunction.18 Given that not all cases of GIRD contribute to pathology, distinguishing between these sub-types is necessary to better understand its implications for volleyball players and to develop targeted prevention and treatment strategies. There are several proposed theories stipulating the reason for this change in range of motion including posterior capsule tightness, humeral retroversion and mixed theories.20–24 Among these existing theories, posterior capsule tightness is the most widely accepted of all. Many players suffering from injuries resulting from GIRD, initially complain of pain without the presence of injury, shoulder stiffness, reduced movement velocity and increased warm-up time.25,26 Later, these complaints often lead to missed practice.6,27
Given the prevalence of GIRD and its implications for shoulder health in overhead athletes, this study aims to examine its association with key athlete characteristics. The purpose of this study was to analyze the prevalence of anatomical and pathological GIRD sub-types in volleyball players and examine their association with gender, court position, weekly practice time, and experience.
METHODS
Study Design
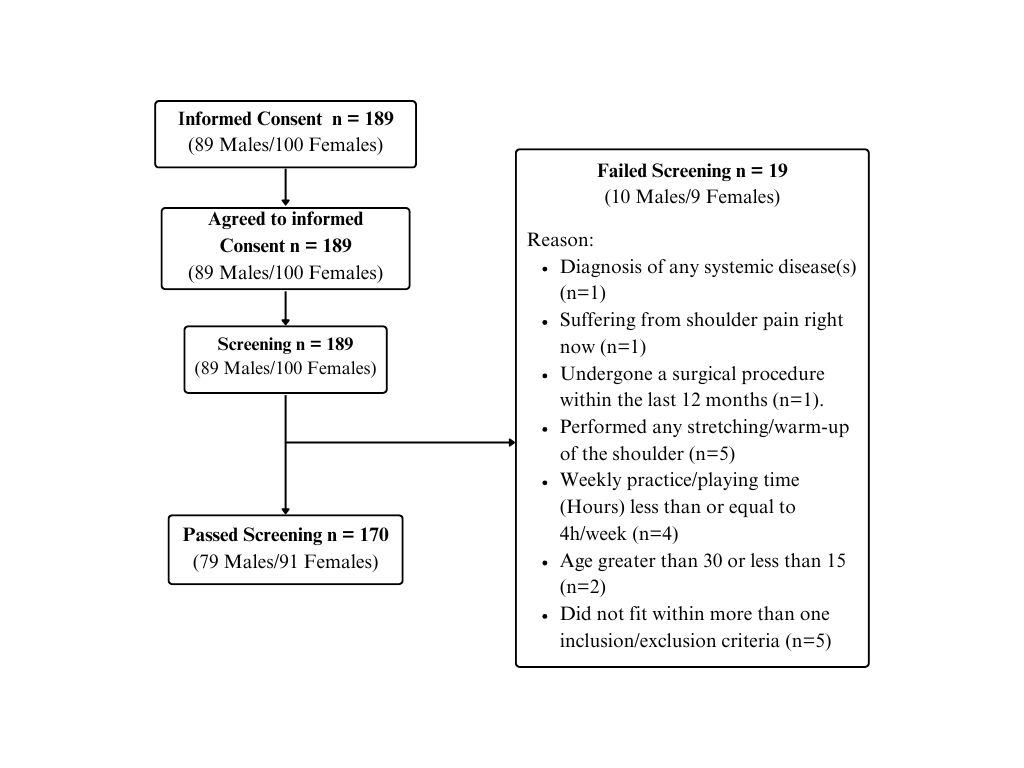
This cross-sectional study took place over six months in which the sample size (n = 189) was calculated using Slovin’s formula, where the estimated population was 360 with a 5% margin of error.28 The study was approved by the Institutional Review Board (IRB) at Ibadat International University (IRB reference number: 0223-1021).
n =N(1+Ne2)=360(1+360∗(0.05)2)=189
Non-probability convenience sampling was utilized to gather data of professional and semi-professional volleyball players from nine different locations including University Gymnasium, Volleyball Training Academies, and National Team Training Centers. Upon application of the inclusion and exclusion criteria, the final data analysis was conducted on 170 participants. The inclusion criteria consisted of those that were aged between 15-30; had experience as Volleyball Player that was greater than or equal to one year; and had a weekly practice/playing time that was greater than 4h/week. Those excluded were excluded due to prior diagnoses of internal impingement, rotator cuff injury, SLAP lesion, glenohumeral joint instability, posterior labral tear, scoliosis/kyphosis, posterior capsule contracture, partial articular-sided supraspinatus tear (PASTA), Scapular Dyskinesia (SICK scapula), Bennett lesion, and frozen shoulder. Additionally, exclusion criteria encompassed current shoulder pain, systemic disease, recent shoulder surgery (within the prior 12 months), shoulder stretching/warm-up, and recent shoulder displacement or fracture (within the prior 6 months).
Data Collection Procedure
After signing an informed consent, a semi-structured questionnaire consisting of three parts was utilized to gather data.
Part 1: Demographics
This section of the questionnaire consisted of questions regarding age (years), sex, presence of specified shoulder condition(s) (internal impingement, rotator cuff injury, Superior Labrum Anterior (SLAP), glenohumeral joint instability, posterior labral tear, scoliosis/kyphosis, posterior capsule contracture, partial articular-sided supraspinatus tear (PASTA), Scapular Dyskinesia (SICK scapula), Bennett lesion, frozen shoulder). Additionally, details regarding the presence of any systemic illness, history of shoulder dislocation or fracture within the prior six months, history of shoulder surgery within the prior 12 months. The questionnaire included a section to determine whether players had engaged in shoulder warm-ups or stretching immediately before completing the questionnaire. This information was collected to account for potential differences in range of motion due to warm-up effects. Additionally, data regarding the presence of pain at the time of assessment were recorded.
Part 2: Environmental Factors
The second part of the questionnaire focused on the collection of data related to the participants’ play including hand dominance (defined as the arm used to spike or serve), court playing position (setter, middle blocker, libero, outside hitter/left-side hitter, middle hitter, opposite hitter/right-side hitter), weekly practice time (hours), and experience (years).
Part 3: Physical Examination
This section involved measuring and recording the internal and external range of motion of the participants’ shoulder joints in both the dominant and non-dominant arms using a goniometer. These physical measurements were then used to calculate the total range of motion for each shoulder.
Goniometric Measurements
A universal goniometer with 1° increments was utilized to measure the rotational range of motion in the dominant and non-dominant shoulder. The participants were placed in a supine-lying position with their arms sufficiently hanging beyond the plinth to allow full range of motion in 90° of shoulder abduction, 90° of elbow flexion and the wrist in neutral. Shoulder internal and external rotation were measured passively by placing the goniometer axis on the olecranon process and the stationary arm perpendicular to the floor, while the moveable was kept in line with the ulnar styloid process. Another examiner stabilized the shoulder joint superior to prevent scapular accessory motion from causing errors in measurement. The measurements were performed by two consistent examiners, who were students, overseen by a certified physical therapist.
Internal Rotation Deficit and Total Range of Motion Calculation
Internal rotation deficit was calculated by finding the difference between the internal rotation of the dominant arm and the non-dominant arm (internal rotation dominant – internal rotation non-dominant = internal rotation deficit). The total range of motion dominant arm was calculated by summing the internal and external rotation of dominant arm (internal rotation dominant arm + external rotation dominant arm = total range of motion dominant arm) and the same was done for non-dominant arm total range of motion (internal rotation non-dominant arm + external rotation non-dominant arm = total range of motion non-dominant arm). Finally, the total range of motion difference was calculated by finding the difference between the total range of motion in the dominant arm with the total range of motion in the non-dominant arm.
Data Analysis Procedure
All statistical analyses were performed using SPSS 26.0 software (IBM SPSS Inc, Armonk, NY, USA). Normality of variables including age, weekly practice time, experience in years, internal rotation (dominant and non-dominant), internal rotation difference, external rotation (dominant and non-dominant), total range of motion (dominant and non-dominant), total range of motion difference was checked using Kolmogorov-Smirnov test, which showed all variables had non-normal distribution, except for the total range of motion of the dominant arm. Hence, data distribution was summarized as mean with standard deviation and median with quartiles. Categorical variables were summarized with counts and percentages Chi-square tests of independence were conducted to examine associations between GIRD classification (aGIRD, pGIRD, absent GIRD) and categorical variables including playing experience, weekly practice time, gender, and court playing position. These analyses were used to identify potential relationships between athlete characteristics and GIRD type.
RESULTS
A total of 189 individuals completed the survey, of which 19 did not meet the inclusion criteria leaving 170 participants who completed the study. Participants recruitment and reasons for exclusion are illustrated in Figure 1.
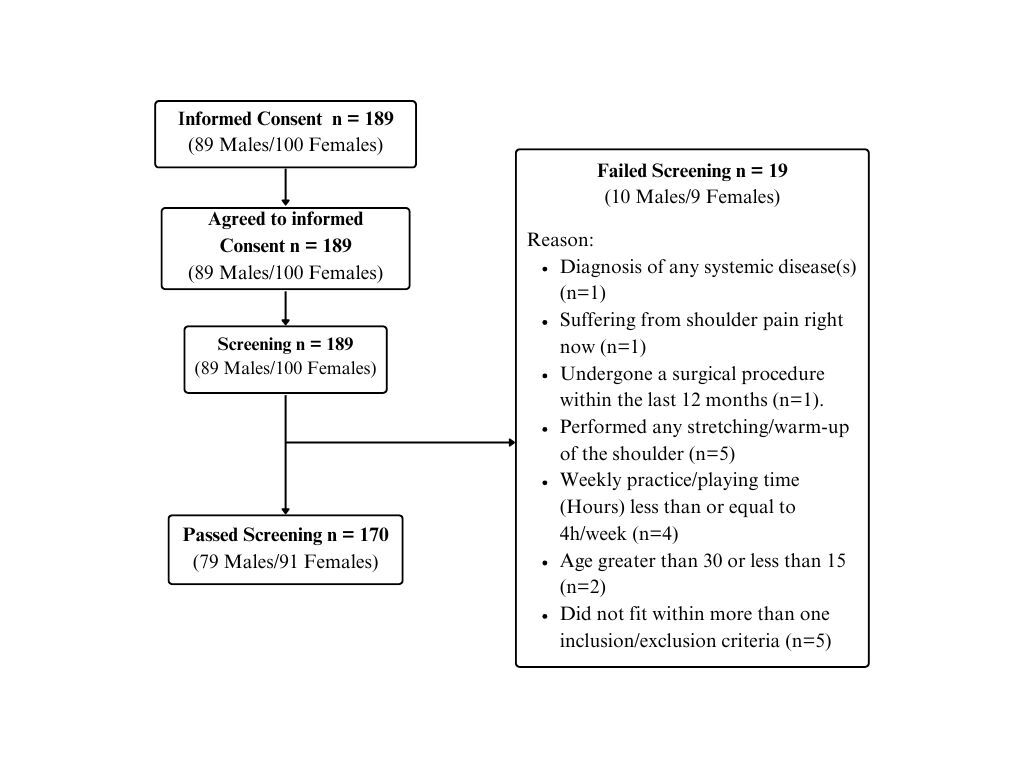
Table 1 shows the mean with standard deviations and median with quartiles for all continuous variables providing us insight that most players were young, with minimal experience, however, they showed high weekly practice time. The rotational values shown in Table 2 indicate that the mean internal rotation difference was -6.51° ± 8.22°, with a median of -6.00° (Q1: -10.00, Q3: -5.00). While the group mean does not exceed the 18° threshold for pathological GIRD, individual variability was present, with some participants exhibiting internal rotation deficits greater than 18°. Additionally, the total range of motion (TROM) had a mean of -7.21° ± 15.95°, with a median of -5.00° (Q1: -15.00, Q3: 2.00). Given that Manske et al. classify GIRD not only by an internal rotation deficit exceeding 18° but also by a TROM asymmetry greater than 5°, some participants in the sample met the criteria for pathological GIRD through this alternative classification. However, the median for the total range of motion difference (-5.00°) indicates anatomical GIRD presence (anatomical GIRD = internal rotation difference < 18° and TROM asymmetry or up to 5-degree difference).
Table 1 also summarizes the count and percentages for the categorical variables. There were more female participants than male, the majority of the athletes were right-hand dominant (n=137), and a large majority with middle hitters (n=63).
The prevalence of GIRD accounted for 89.4% as shown in Table 3. Of those found to have GIRD majority were found to have pathological GIRD rather than anatomical GIRD, although the difference was minimal.
Further analysis revealed significant associations between GIRD classification and key athlete characteristics, including experience, weekly practice time, gender, and court playing position, as shown in Table 4. Athletes with more experience and higher weekly practice hours were more likely to exhibit pathological GIRD, suggesting that increased exposure to repetitive overhead movements may contribute to a more pronounced internal rotation deficit. Additionally, male athletes were found to have a significantly higher prevalence of pathological GIRD, while females showed a greater incidence of anatomical GIRD. Court playing position also played a role, with positions such as Middle Hitter and Outside Hitter showing a higher prevalence of pathological GIRD, whereas Setters and Middle Blockers had more balanced shoulder mobility profiles.
DISCUSSION
The present study aimed to investigate the prevalence of GIRD among volleyball players, offering a unique perspective on this condition that deviates from previous research findings. The results of this study revealed an exceptionally high prevalence of GIRD within this volleyball player population (89.4%). Notably, the majority of participants were middle hitters (37.1%), a position that demands frequent and forceful overhead movements, which may have contributed to the high prevalence observed. The repetitive nature of spiking and blocking in this role places substantial stress on the shoulder, potentially increasing the risk of internal rotation deficits over time.
Comparisons with prior research findings are intriguing, as they have generally reported lower prevalence rates. For instance, a study conducted by Mizoguchi et al. in Japan found a prevalence of 38.2% among 123 adolescent volleyball players. In their study, internal rotation differences over 10° and a total range of motion greater than 5° were established as diagnostic criteria for GIRD.29
The reason for this difference in the current findings and the Mizoguchi study may be attributed to several factors. First, the Mizoguchi study focused on adolescent athletes, while the current study included a cohort of adult participants (24.45 ± 3.24). Additionally, participants had significantly higher weekly practice time (18.58 ± 16.44 hours), which may contribute to a higher prevalence of GIRD. Furthermore, the current study excluded symptomatic or injured participants to ensure that measurements reflected true range of motion, whereas the Mizoguchi study did not exclude these individuals. Finally, differences in injury history and playing positions, as well as potential variations in training protocols between the two populations, could also explain the disparity in prevalence rates.
Another study by Miura et al. in Japan that studied the prevalence of GIRD and its association with suprascapular nerve neuropathy in male volleyball players noted a prevalence of 18.2% in a sample of 22 participants, among this sample four participants were found to have pathological GIRD (internal rotation difference > 20°).30 Research on beach volleyball players done by Saccol et al. reported a significantly lower dominant GIRD prevalence of 18.2% in young beach volleyball players, additionally, the study primarily focused on asymptomatic athletes and identified only 6 cases of pathological GIRD from a sample of 33 players.31
Other research including overhead athletes in general also reported significantly lower prevalence rates of GIRD. An investigation by Srivastav et al. among collegiate overhead athletes in India indicated a prevalence of 29.1%; these players included athletes that played cricket, baseball, basketball, throw ball, volleyball, badminton, lawn tennis, and squash.32 This discrepancy in findings between the two studies may be due to differences in training volume, with athletes in this study having higher weekly practice hours, leading to greater shoulder adaptations. Additionally, volleyball’s repetitive overhead demands, along with the classification of both anatomical and pathological GIRD, likely contributed to the increased prevalence. Methodological differences, such as goniometer use under PT supervision versus an inclinometer in a prone position, may have also influenced results. Lastly, gender and positional differences played a role, with male athletes and hitting positions showing higher rates of pathological GIRD. These factors may collectively explain the higher prevalence observed in this study.
Another study by Whiteley et al. involving professional male overhead athletes (baseball, handball, and volleyball) reported a GIRD prevalence of 15.4% and a TROM deficit prevalence of 34%. The criteria defining GIRD was set as internal rotation loss of ≥ 20° and TROM difference was set at ≥ 5°.33 The difference in reported prevalence can be attributed to several factors, such as, Whiteley et al. included athletes from multiple sports, whereas this study focused exclusively on volleyball players, whose frequent, high-velocity overhead movements, such as spiking and serving, may lead to more pronounced shoulder adaptations. Additionally, differences in measurement techniques may have contributed - Whiteley et al. used an inclinometer in a supine position, while this study utilized a universal goniometer under physical therapist supervision, potentially affecting accuracy and sensitivity. Another major factor is the difference in diagnostic criteria; while Whiteley et al. defined GIRD based solely on an IR loss of ≥20°, the present study classified both aGIRD and pGIRD subtypes, incorporating total range of motion (TROM) asymmetry into the diagnosis. This broader classification may have increased the sensitivity of detection. Furthermore, variations in training volume and athlete experience likely played a role, as participants in this study had higher weekly practice hours, which has been associated with an increased prevalence of pathological GIRD.
A study conducted by Schmalzl et al. in Germany showed the closest prevalence rate to the current findings, reporting a GIRD prevalence of 72% in a sample of 134 players (67 volleyball + 67 handball).34 Common factors contributing to this high prevalence in both studies include the repetitive nature of overhead sports, prolonged exposure to these movements, and the cumulative effects of training load over time. Both studies also highlight that increased experience and training frequency are associated with higher GIRD prevalence, reinforcing the notion that prolonged engagement in overhead sports leads to greater adaptations or deficits in shoulder mobility.
However, slight differences exist between these two studies. While Schmalzl et al. examined both volleyball and handball players, the current study focused exclusively on volleyball athletes, potentially influencing the higher prevalence. Additionally, the current study differentiated between anatomical and pathological GIRD, which provided a more nuanced understanding of the condition’s severity. Another key distinction is training volume; participants reported higher weekly practice time (18.58 ± 16.44 hours), which may have contributed to the increased prevalence compared to Schmalzl et al., where professional athletes were categorized based on training frequency (>3 sessions per week). Despite these differences, both studies emphasize the importance of monitoring and managing GIRD to prevent potential shoulder pathologies in overhead athletes.
Lastly, the current study went beyond mere prevalence assessment and aimed to quantify the classification of GIRD sub-types, and a higher prevalence of pathological GIRD (52.6%) than anatomical GIRD (47.4%) was found. This higher prevalence of both anatomical and pathological sub-types of GIRD is a novel finding that diverges from the existing literature, which could be a factor that significantly contributed to the high prevalence rate.
While the reasons for this increased prevalence in the current study require additional examination, there are probable variables contributing to this study’s unique findings, which may include variances in training methodologies, playing styles, and biomechanical demands particular to volleyball. It is worth noting that the current research sample was diverse, thus the findings may be relevant outside of a certain group. Furthermore, the lack of pre-season screening and post-season readings may worsen this gap in prevalence. A complete pre-season screening that includes biomechanics, range of motion, and muscle imbalance tests could give insight into possible risk factors for GIRD. Similarly, post-season evaluation might help in understanding the impact of certain sports related activities and demands on athletes’ shoulders. The lack of pre-season screening in this study’s volleyball players may render players vulnerable to injuries, which may contribute to this study’s significantly greater GIRD prevalence. As a result, adopting pre- and post-season examinations might be critical in enhancing athletes’ general well-being and decreasing the occurrence of GIRD in the volleyball community. Future longitudinal studies are warranted to evaluate the effectiveness of such preventative strategies over time.
Limitations
This study is not without its limitations. One potential source of bias is the population of higher-level athletes included in this study sample. The majority of participants in this study were professional-level players which could have influenced the higher observed prevalence of GIRD. Professional athletes are subjected to more intensive training and competition, which may increase their risk for developing shoulder conditions like GIRD. As such, the current findings may not be generalizable to lower-level or recreational athletes.
This study’s reliance on participants’ self-reported shoulder conditions presents a limitation, as memory lapses and the possibility of asymptomatic cases could have impacted the accuracy of the data. Additionally, due to budget constraints, comprehensive diagnostic verification was not feasible, which may have affected the reported prevalence accuracy. These factors should be considered when interpreting the findings.
Another limitation of this study is that the “Experience” variable only reflects participants’ professional-level playing experience and does not account for their youth-level experience. As a result, the reported years of experience may appear lower than the true cumulative experience of the athletes. This could impact on the comparison of current findings with other studies that focus on youth athletes, where experience at the youth level may have a more significant influence on the prevalence of GIRD. Future studies may benefit from including total playing experience, encompassing both youth and professional levels, to provide a more comprehensive understanding of the relationship between playing experience and the development of GIRD.
Finally, this study lacks reporting the Intraclass Correlation Coefficients (ICCs) to assess the inter-rater reliability of the goniometric measurements that were performed. Although the measurements were taken by trained students under the supervision of a qualified physical therapist using standardized protocols, ICC’s were not specifically calculated or reported to quantify the consistency of the measurements across examiners. Future studies may consider including ICCs to further assess the reliability of the range of motion assessments and ensure the precision of the data collected.
A limitation of the Pearson Chi-square test used in the court playing position analysis is that five cells (27.8%) had expected counts less than five, which violates one of the assumptions of the test. This should be considered when interpreting the results. However, despite this limitation, the Pearson Chi-square values remained statistically significant, suggesting meaningful relationships between court playing position and GIRD classification.
CONCLUSION
Based on the findings of this study, it is evident that Glenohumeral Internal Rotation Deficit (GIRD) is highly prevalent among volleyball players, with 89.4% of participants exhibiting some form of GIRD. The majority of those affected had pGIRD, although aGIRD was also present in a significant portion of the sample. Factors such as years of experience, weekly practice time, gender, and court playing position were all found to have significant associations with the classification of GIRD, highlighting the influence of repetitive overhead movements on the development of internal rotation deficits.
These findings emphasize the importance of continued monitoring and early intervention to manage GIRD and mitigate its potential impact on shoulder health and performance. The results suggest that athletes with more experience and higher training loads are particularly at risk for pathological GIRD, underscoring the need to address shoulder mobility deficits in this group. Given the high prevalence of GIRD and its potential consequences for performance and injury risk, further research is necessary to explore effective prevention and treatment strategies in volleyball athletes.
Acknowledgements
The author would like to thank Dr. Giampietro Vairo at The Pennsylvania State University for his invaluable support, encouragement, and feedback throughout the process, which made this publication possible.