BACKGROUND
Ulnar collateral ligament (UCL) injuries have steadily increased in overhead athletes, including those who throw the javelin, over the past 20 years.1–3 Various factors, including sport specialization in adolescent athletes, increased throwing volumes, and increased velocity contribute to this rise in injuries.4–10 In turn, ulnar collateral ligament reconstruction surgery (UCLR) is increasingly performed on overhead-throwing athletes.2,11–13 Baseball pitchers have been particularly affected, and historically, postoperative UCLR rehabilitation protocols for overhead throwers have focused on baseball athletes. Despite the focus on baseball, javelin athletes javelin are at an even higher risk of UCL failure14,15 with 6.69 times the odds of sustaining a UCL injury compared with all other sports and significantly higher than in baseball when compared to all other sports (odds ratio: 1.55).11,16 This is not surprising given the differences in release angle, mass of the javelin, and higher levels of force transmission up the kinetic chain compared to baseball pitchers.17
With the rise in UCLR procedures, there is an increased focus on optimizing return to sport (RTS) outcomes through effective postoperative rehabilitation and return to play programming. However, the definition of “return to sport” varies across the current body of knowledge spanning from “return to participation” to return to sport at pre-injury level of competition.18 Postoperative UCLR outcomes are generally favorable, with 86.2% of UCLR cases across multiple sports and performance levels reportedly returning to their sport at their pre-injury level of performance, but again these reports are biased towards baseball pitchers.19 Given the different injury risk profiles, there is a need for distinct return to sport strategies to specifically accommodate javelin thrower needs. This systematic review aims to assess the current literature for return-to-sport criteria and identify gaps and opportunities for developing javelin-specific return to sport progressions.
METHODS
This systematic review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines.20
Eligibility Criteria
Boolean search related to javelin, UCLR surgery, and the resumption of sports activity was performed with the assistance of a medical librarian. PubMed and Medline databases were searched using Medical Subject Headings (MeSH) terms. In addition, controlled vocabulary search terms were derived from associated MeSH terms and used to search the title and abstract of articles.
Inclusion criteria consisted of (1) articles written in English; (2) published between January 2000 and May 2024; (3) a patient population of javelin athletes of any age and level of competition, which includes professional, collegiate, high school, and middle school; (4) patient population undergoing UCLR using any surgical technique or graft; (5) a study follow-up of a minimum of one year including a return to throwing protocol; and (6) study results reporting an RTS outcome. Exclusion criteria consisted of (1) entire non-javelin athlete population of study; (2) published before the year 2000; (3) biomechanical studies; (4) epidemiologic studies; (5) conservative treatment studies; and (6) background information studies.
Information Sources and Search Strategy
The search was performed on May 31, 2024. The search strategy was first developed in PubMed and subsequently adapted to other databases, including ProQuest, PEDro, Scopus, CINAHL, Cochrane, EMBASE, and SPORTDiscus. The search strategy is provided in the Appendix.
Data Collection and Analysis
Study Identification
Screening was conducted in three phases to identify eligible studies. The initial PubMed and Medline search was conducted by Authors 1 and 2. Articles were initially screened by title first and then by abstract. Before moving to full-text screening, blind consensus was achieved on the title and abstract review using the Rayyan blind systematic review web application (Qatar Computing Research Institute, Ar-Rayyan, Qatar).21 The two lead researchers (Author 1, Author 2) reviewed the full text of the articles, and blind consensus was formed via Rayyan. The senior researcher then reviewed the results to ensure complete consensus. Data extraction was performed independently for each article by Author 1 and Author 2 via Rayyan to ensure the accuracy of the systematic review. If consensus was not achieved, discrepancies were resolved through discussion and revisitation of the article. If consensus were still unachieved, the senior researcher functioned as a “tiebreaker.”
Quality Assessment
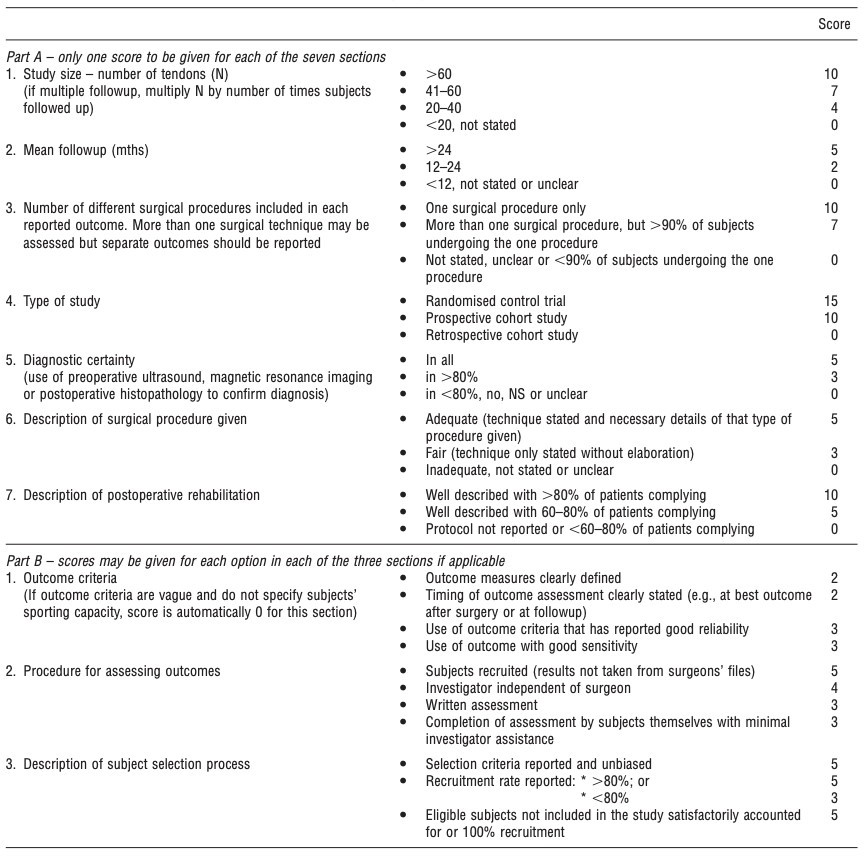
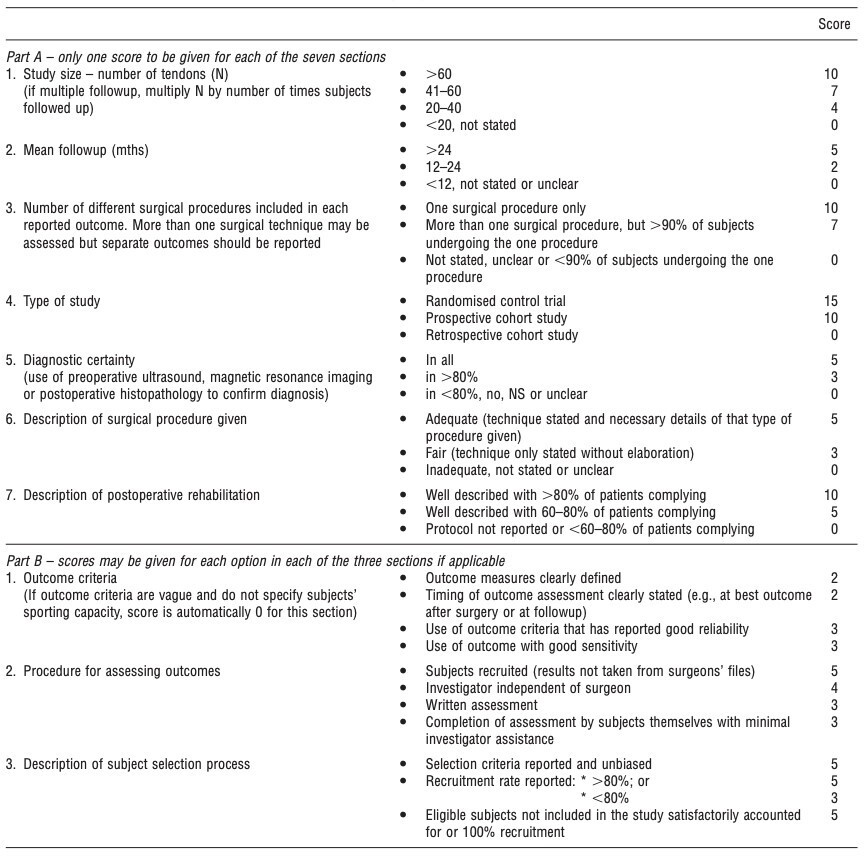
Study Authors 1 and 2 independently conducted quality assessment of the included studies via the Coleman Methodology Score (CMS) (Figure 1). The CMS was initially developed to assess the quantitative methodologic quality of studies evaluating surgical outcomes.22 Scoring is based on 10 criteria, covering aspects of the study design and recruitment, sample size, surgical procedure, diagnostic certainty, and postoperative outcomes. Scores range from 0 to 100, with lower scores representing more significant bias and higher scores representing an absence of bias. CMS scores are categorically arranged based on the representation of the total score (Table 1). The scoring is as follows: excellent (85-100), good (70-85), fair (50-69), and poor (less than 50) (Figure 1). CMS scores were not utilized for inclusion/exclusion purposes; the quality assessment was used to give context to interpretation of the findings.
RESULTS
Study Selection
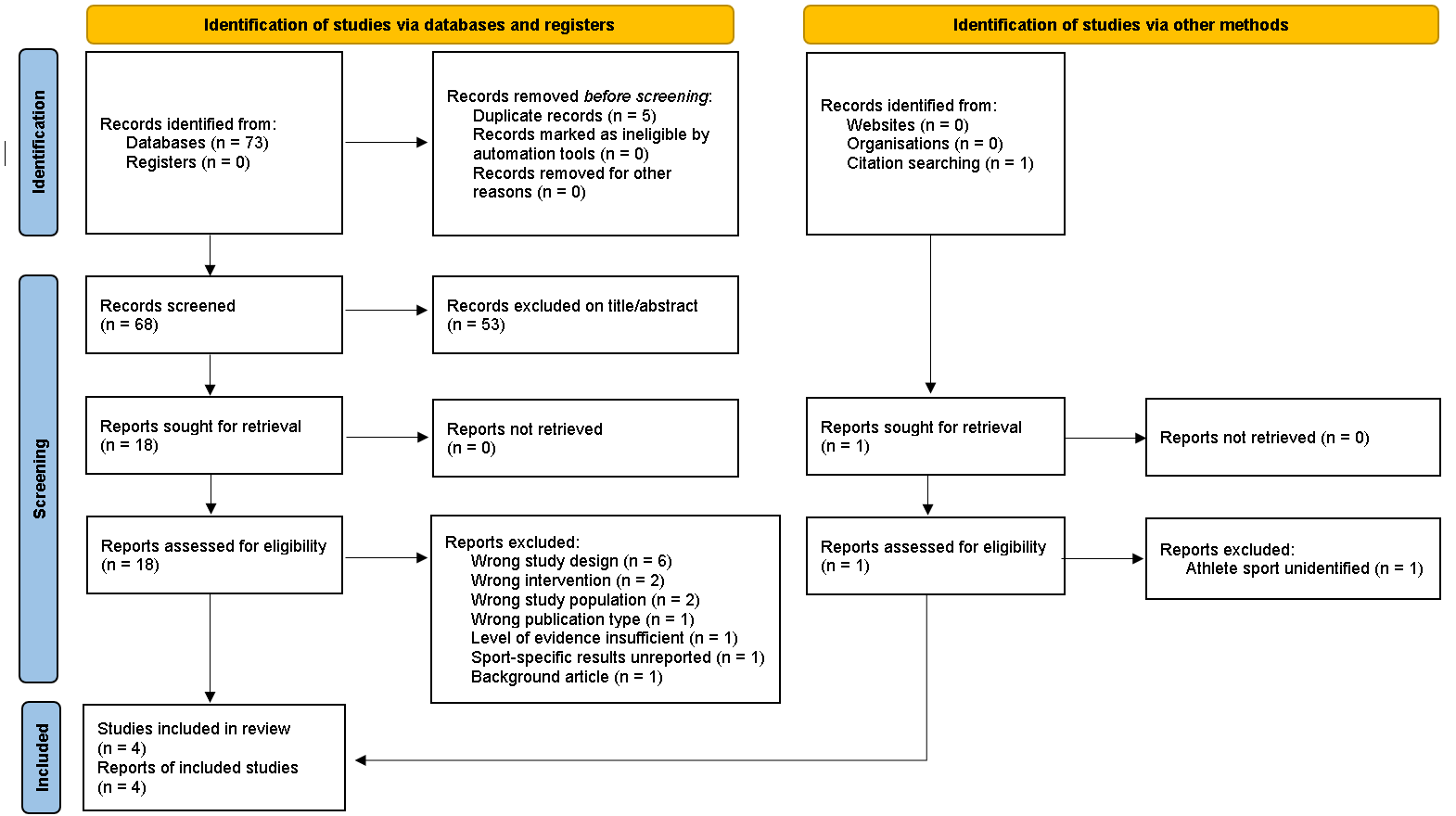
Database searches identified 73 records, 68 remaining after removal of duplicates. 53 records were excluded after title and abstract screening, leaving 18 full-text articles undergoing eligibility assessment. Following the screening process, four studies met the inclusion criteria for this systematic review (Level 3a evidence).23–26 The PRISMA flow chart reports stepwise study identification and selection processes (Figure 2).
.png)
Quality Assessment
Of the four included studies, three were rated as fair,23–25 with one rated as poor.26 CMS total scores ranged between 44 and 61. Only one study reported on the number of different surgical procedures included in the outcomes23 and one provided a description of the surgical procedures utilized rated as adequate using CMS scoring,25 with the remaining three rated as fair. All four studies scored a 10/10 on the CMS for outcome criteria reporting.
Demographics and Procedures
The four studies included in this systematic review included a total of 34 javelin throwers competing at the professional (1),24 Olympic (1),26 collegiate (21),23–26 high school (9),23–26 and recreational levels of play (1),24 with one study participant competing at an unaccounted for level of play (Table 2).25 Mean ages of study participants were between 18 and 21 years in the individual study populations with an overall mean age of 19.7 years. Of the 34 study participants, seven female and 27 were male. While all participants in the four studies underwent primary UCLR, variations in the surgical techniques were used.23–26 All studies included the utilization of palmaris longus and gracilis autografts, with Hadley et al.24 also including plantaris autografts and O’Brien et al.26 including medial Achilles grafts and semitendinosus allo- and autografts.23–26 The minimum follow-up period for all studies was two years.
Outcomes were assessed by return to sport rates (Table 3) and patient-reported outcome scores (Table 4). No physical or functional performance measures were reported to signify the completion of a protocol phase in any of the studies or to determine a successful outcome.
Return to Sport
All studies used the completion of a UCLR rehabilitation protocol and throwing program to measure the success of UCLR surgery (Table 3).23–26 Physical and functional measures, such as range of motion, power, endurance, coordination, or strength, were not assessed in any study. These studies also outlined a formal return-to-throwing (RTT) program as part of the rehabilitation protocol, with time as the criteria for initiation. Initiation of postoperative RTT was eight months for the Dines study,23 six months for the Hadley study,24 and four months for the O’Brien study.26 Jones did not report when the RTT was initiated for javelin throwers, however, baseball pitchers in the study began their RTT protocol at four months postoperatively.25 Study RTS rates are provided in Table 3.
Patient Reported Outcomes
The Timmerman-Andrews Elbow Score (TAES) and the Conway-Jobe Score (CJS) were used as patient-reported outcomes (PRO) measures in three of the four studies.23–25 The Kerlan-Jobe Orthopaedic Clinical Shoulder and Elbow Score (KJOC) score was also reported in the O’Brien, Hadley, and Jones studies.24–26
The TAES was created to measure objective and subjective postoperative symptoms in patients undergoing arthroscopic procedures for traumatic injuries of the elbow.27 Objective (flexion contracture, pronation/supination, sagittal arc of motion) and subjective (pain, swelling, locking/catching, activity limitations) symptoms are scored separately on a scale from 0-100 and are then combined to give an overall total score between 20 and 200. Higher scores reflect more favorable outcomes. Scores as categorized as excellent (90-100), good (80-89), fair (60-79), and poor (<60). Overall total scores are categorized as excellent (180-200), good (160-179), fair (120-159), and poor (<120).28 Despite its adoption as a measure of the success of surgical procedures of the elbow, the TAES is not a validated patient-reported outcome measure, with no minimally meaningful clinical difference in scores determined.28
The CJS was developed to quantify an athlete’s ability to return to performance after UCLR and uses the same excellent-good-fair-poor rubric as the TAES to evaluate postoperative outcomes.28 Like the TAES, the CJS has not been validated, and no minimally meaningful clinical difference has been reported.28
The KJOC is an inventory of the presence and impact of pain, fatigue, weakness, instability, and activity limitations specific to the overhead athlete.29 It has been previously validated in adult and youth male baseball populations and youth female softball populations.29–31 Questions are scored using a 10-point Visual Analog Scale (VAS) and summarized with a final score on a 0-100 scale. Athletes with higher KJOC scores are more likely to throw without symptoms. Hadley et al. also recorded PRO results using a return-to-sport questionnaire and a satisfaction survey.24 All Hadley et al. PRO results were included only if a study participant achieved two or more years of follow-up.24
PRO scores for the included studies are summarized in Table 4. TAES subjective scores were rated as excellent across the three studies utilizing it, with average scores ranging from 90.7 and 97.23–25 CJS scores were recorded in three studies, with 80% of Jones et al.25 and 90% of Dines et al.23 outcomes considered excellent. Outcomes in the Hadley et al.24 study were less frequently rated as excellent using the CJS (37.5%) and showed greater variability in CJS scores in comparison to the Jones et al.25 and Dines et al.23 studies. Average KJOC scores were indicative of athletes throwing without symptoms post UCLR, with Jones et al.25 participants reporting higher scores (94.8) in comparison to those in the O’Brien et al.26 (77.5) and Hadley et al.24 (77.3) studies. Across all the respective studies and assessments, participants reported favorable post UCLR outcomes.
DISCUSSION
Overview
To the authors’ knowledge, this is the first systematic review focusing on sport-specific criteria for RTT/RTS after UCLR among javelin athletes. A key finding is that none of the studies under review reported evaluation criteria for RTT/RTS programs based on physical or functional performance measures, such as range of motion, strength, or pain, found in other sports.32–35
A recent systematic scoping review of RTS guidelines post-UCL surgery found baseball studies to be similarly limited in the scope of their criteria, with a single study including strength or ROM assessment and three with pain as part of their criteria.35 This limitation contrasts with soccer, where more formal, objective criteria with measures of functional performance are standard practice in RTS post-anterior cruciate ligament (ACL) reconstruction.33,36,37 Furthermore, failure to meet all aspects of the RTS criteria has been associated with a greater risk of ACL reinjury, highlighting the importance of introducing more comprehensive criteria in post-UCLR RTS protocols in javelin.33
The final phase of the rehabilitation process involves the implementation of an RTT program to allow the athlete to prepare for RTS at pre-injury levels of competition. A detailed description of the RTT program components that include specifics for throwing distances and intensity, throw counts, and throwing session frequency at each stage of the program are commonly reported in post-UCLR outcomes studies in baseball.38–40 Neither Dines,23 Jones,25 or O’Brien26 elaborated on their throwing prescription, only reporting the program’s start as beginning eight months into the rehabilitation program. A comprehensive description of RTT programming was provided only in the Hadley et al. study whose subjects started postoperative RTT at six months.24
Given the biomechanical requirements of the sport, future javelin assessments must incorporate both temporal and objective (physical and functional) milestones analogous to those included in postoperative RTS procedures in other sports, such as soccer, and interpret their findings as part of post-UCLR rehabilitation progression criteria. For further objectivity and reliability of grading advancement through an RTT program, the use of wearable sensor technology to measure kinematic values is also encouraged.41
Return to Sport
Ther RTS rates reported by the Dines,23 Hadley,24 Jones,25 and O’Brien26 javelin studies under review are poor compared to other sports, except for Dines study subjects.23 In a systematic review by Erickson et al., the pooled rate of post-UCLR RTS across multiple sports was 86.2% (n = 2,019).19 An average RTS rate of 84.1% was reported by Trofa et al., in their systematic review evaluating RTS outcomes in 2,154 athletes across multiple sports undergoing a primary UCLR using palmaris versus hamstring tendon grafts; the average RTS at the previous level of play was 79.0% in the study.42
Comparable results are observed in literature limited to baseball pitchers. A review and meta-analysis by Peters et al.43 of 22 studies involving 2,020 baseball pitchers with UCL injury (with or without tear) undergoing surgical or conservative treatment specified a mean RTS of 90% across all levels of competition (95% CI: 86% - 94%). RTS at the previous level of play for the study was 79% (95% CI: 75% - 84%). Glogovac et al.43 reviewed studies of post-revision UCLR RTS in high-level baseball players and reported an overall return to preinjury level of performance of 62.8% and returned at any level of performance of 78.1% in 160 athletes across five studies.
For the javelin studies, postoperative RTS rates at any level of performance was between 62.5% and 100%, which are comparable to those in baseball, but generally lower than rates seen in non-baseball sports. Javelin throwers also fared poorly in achieving RTS at the same level of performance before UCLR (range: 43.7% - 90%), especially in comparison to college baseball pitchers (92%), a cohort of similar age and biomechanical demands of their sport.34
Patient Reported Outcomes
The studies used several patient-reported outcome tools, including the KJOC, TAES, and the CJS. All athletes participating in these studies scored highly on the TAES (TAES >90%). The CJS was reported most frequently as Excellent across all studies. Average KJOC scores varied substantially between athletes in the Hadley24 (77.3) and O’Brien26 (77.5) studies in contrast to those in the Jones study (94.8).25 The interpretation of the authors is that differences in age, instructions provided to study participants for assessment completion, and the type of surgical procedure and graft used by the surgeon could contribute to these differences. The heterogeneity amongst the PRO results underlines a lack of consensus on outcomes measurement standards for RTT programming and the criteria used to determine satisfactory program completion. This observation has implications for patient-reported outcomes when returning to pre-injury throwing levels, further highlighting a gap in the current literature.
Quality Assessment
The CMS scores of the four studies reflect a sizeable amount of study design susceptibility to uncontrolled bias, confounding, and results attributable to chance (Dines: 61; Hadley: 55; Jones: 51; O’Brien: 44).23–26 While total scores indicate fair overall quality, Part B items of the CMS are strong points of the individual studies (outcome criteria, outcome assessment procedure, subject selection procedure). A notable difference in the number of procedure types per group category (Part A) is observed (Dines:7; Hadley, Jones, and O’Brien: 0/not stated or unclear), contributing a significant source of vulnerability to bias and confounding.23–26
These total scores resemble a systematic review of return to sport outcomes post-UCLR with palmaris versus hamstring tendon grafts in overhead athletes performed by Trofa and colleagues, which reported a mean total score of 63 using the modified CMS (mCMS).42 Erickson et al. also used mCMS in their systematic review to determine bias risk, reporting a mean total score of 34.7, rated as low.19
Heterogeneity of bias assessment results is seen within the studies and across comparable RTS studies, which all used differing tools for evaluation methodologic rigor.19,42–44 Direct appraisal of bias across studies is not feasible due to these method variations.
Limitations
Certain limitations in this study should be considered when interpreting the results of this review. The total number of athletes represented in the four articles meeting all inclusion is 34.23–26 This systematic review identified only two studies that included female participants, contributing only three of the 34 total subjects.25,26 The sparsity of available data related to the javelin population limits the authors’ confidence in establishing the generalizability of success of UCLR outcomes in javelin athletes. Surgical attributes varied within and across studies. Differences in reconstruction technique and autograft selection are noted. As such, the effects of these clinical decisions on the findings cannot be ascertained with certainty. This limitation is further highlighted by the CMS scoring, predominately rated as fair or unclear for these factors, indicative of results low in certitude. Surgical outcomes were also subject to variability, with three studies having UCLR procedures performed by multiple surgeons and one having procedures performed by one surgeon. These surgeon-specific effects introduce further confounding and uncertainty on the understanding of the study outcomes. Follow-up times showed substantial variability, ranging between 24 months to 9.6 years. Inconsistencies in the PRO instruments selected by the studies are notable, as is the use of instruments whose psychometric properties have not been validated. The scarcity of consensus-based, comprehensive criteria for the minimum time and programming volume requirements of post-UCLR rehabilitation should be considered when evaluating potential reasons for lower RTS success in javelin.
CONCLUSION
There is evidence of a gap in the literature identified by this systematic review: substantial criteria for RTT/RTS clearance assessing physical and functional progressions do not exist for post-UCLR javelin athletes. Four studies reported RTS criteria for post-UCLR javelin athletes, with time the most common criterion used. Only one study provided a specific RTT program, which included stepwise progressions for number, effort, quality, and distance for throws and javelin weights used for each program phase. No studies were identified providing guidelines for RTT or RTS criteria specifically for javelin athletes following UCLR that emphasized objective measures of rehabilitation progress and completion. Defining specific RTT/RTS benchmarks beyond a time-bound completion of protocol steps is necessary, as are future studies with more rigorous methodological quality. The findings of this systematic review suggest an opportunity to develop and establish javelin-specific criteria for post-UCLR rehabilitation that incorporate objective physical performance measures.