
INTRODUCTION
From 2014 to 2019 Division I college football players experienced an overall injury rate of 10.37 per 1,000 athletic exposures, indicating a significant risk of injury during practice and competition.1 Shoulder injuries are widespread among elite collegiate American football players, with nearly half of those evaluated at the 2004 NFL Combine reporting a history of shoulder injury.2 Shoulder injuries in college quarterbacks are particularly concerning due to the vulnerability of the throwing position, the nature of the sport, and the mechanical stresses of throwing. In football, the repetitive overhead activity poses an increased risk for overuse injury in quarterbacks, given the mechanical stresses of throwing.3 Consequently, collegiate quarterbacks have an incident rate of approximately one shoulder injury per 1221 athlete exposures, encompassing both non-contact and contact mechanisms.4 Common anatomic shoulder structures injured in this population include the rotator cuff, labrum, and biceps long head tendon,5–7 which contributes to time loss from sport.4 The prevalence of upper extremity injuries and resultant time lost to injury in collegiate football players, especially quarterbacks, underscores the importance of proper screening, injury prevention and training to safeguard their health and performance.
Currently in orthopedic and sport rehabilitation, there are many valid and reliable tests used to assess lower extremity function and strength such as isokinetic dynamometry and force plate testing. Results of these tests guide clinical decision-making regarding training and readiness to return to sport and training decisions.8–13 However, there is a dearth of literature on comparable testing procedures for the upper extremity. The testing methodologies employed for assessing lower extremity function and performance are not applied in the same way for upper extremity function and performance. This discrepancy arises from the absence of valid and reliable tests currently available.14 Existing upper extremity strength assessments that are commonly used in the clinic are short lever isometric strength tests15 and do not mimic sport specific positions of the overhead athlete. When measuring shoulder muscle strength, it may be advantageous to objectively measure peak force in shoulder positions relevant to the athlete’s sport, in addition to the isolated muscle assessments that are currently employed. Hence, for overhead athletes such as quarterbacks, aiming to replicate voluntary force production in sport-specific positions may be more suitable using a long lever isometric test.16–18 While isokinetic testing is the gold standard to assess strength in the performance and clinical setting, clinical utility is limited by equipment availability, clinic space, cost, and time.19 A reliable and valid alternate testing option for athletes is the use of force plates.20–22 When compared to isokinetic dynamometers force plates are more affordable and have a compact design that allows for flexible placement within existing clinic spaces.
Recently, the Athletic Shoulder (ASH) test, a novel series of long-lever upper extremity isometric tests using force plates, has been proposed by Ashworth and colleagues as a safe and reliable objective measure of isometric force production across the shoulder girdle.23 The ASH test was initially developed to replicate long-lever stress and the ability to transfer force across the shoulder girdle at different degrees of shoulder abduction in elite rugby players,24 and was more recently investigated in baseball players by Trunt and colleagues.25 This test exposes the athlete to a maximal voluntary isometric contraction with cueing to produce maximal force quickly.
Due to demands required of the shoulder with throwing, we aimed to initiate ASH testing in collegiate quarterbacks at a single institution as standard of care for quality improvement. Data for peak force, peak force normalized to body weight ratio, and limb symmetry indices of three collegiate quarterbacks throughout both the pre-season and regular season, were collected utilizing the ASH test. Additional standard of care screening measures for the upper extremity in this group of collegiate quarterbacks include a three-repetition maximum dumbbell bench press test, peak grip strength assessment, and a maximal repetition pull-up test. The team’s strength coaches conduct these tests in pre-season and re-assess them over time throughout the season and off-season to help inform their strength and conditioning programming. This battery of tests assesses muscle strength in positions that are less consistent with the positions and demands of throwing. The use of the ASH test provides data from testing in functional positions that place similar demand on the shoulder in the throwing position of a quarterback.16,17 While there is published data utilizing the ASH test in rugby, softball, and baseball athletes, data does not yet exist for ASH testing in football quarterbacks.23,25,26 The primary purpose of this case series was to explore the feasibility of conducting the ASH test as a method for evaluating upper extremity strength in overhead athletes, specifically collegiate quarterbacks. In addition to this primary aim, the data were also used to compare findings to existing literature from other athletic populations and to help inform training strategies and return-to-play decisions by tracking strength progression throughout the season.
METHODS
The present standard of care protocol was based on the ASH test methodology introduced by Ashworth et al. and further investigated by Trunt et al.23,25 This initiative examined the three collegiate quarterbacks from an NCAA Division 1 university. Testing commenced at the start of preseason training camp to establish baseline peak force levels and lasted eight weeks thereafter. Peak force production was tracked and monitored weekly over those nine weeks. The main variable of interest was isometric peak force.
To standardize procedures, the athletes were tested weekly, in the morning prior to the start of their team practice, on a non-game/scrimmage day to limit the possible effects of fatigue. The three quarterbacks included in this case series were the top three on the team’s depth chart and the only scholarship quarterbacks on the roster. Pre-season screening of participants revealed no current or prior upper extremity injury. Each received in-game repetitions during the season (defined as taking at least one snap) and was selected due to their greater likelihood of competitive play. The remaining quarterbacks on the roster were excluded to reduce potential variability associated with differences in throwing volume, game exposure, and fatigue.
Prior to performing the ASH test, all athletes completed a warm-up for three minutes on an upper body ergometer at a self-selected pace. Testing was then administered by the primary author. Athletes were instructed on test procedures, verbalized understanding, and witnessed a demonstration of the test performed by the primary author. At subsequent sessions, the testing procedures were reviewed and understanding of testing procedures were confirmed prior to administration.
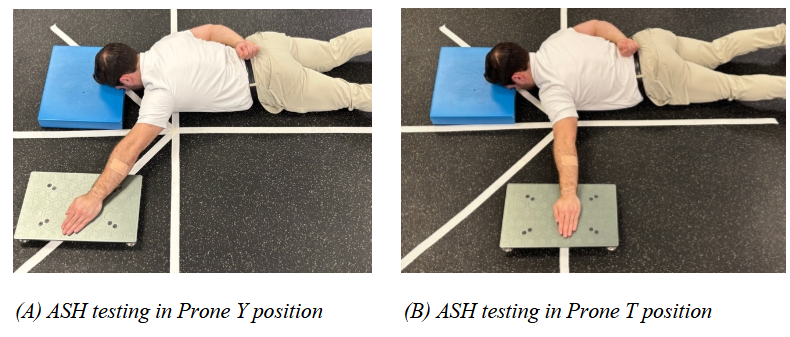
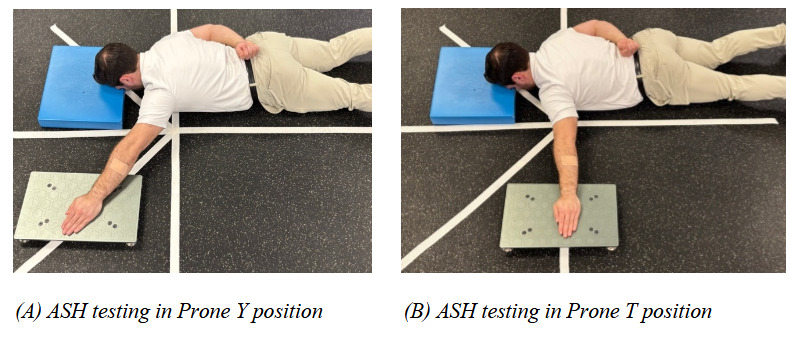
Isometric shoulder strength was measured on the dominant arm followed by the non-dominant arm using the ASH test as described by Ashworth et al.23 Figure 1 depicts the test positions with participants prone on the floor at 135 and 90 degrees of shoulder abduction for the Y and T position respectively, forehead resting on a 4cm pad, forearm pronated, and palm of the hand resting on the force plate as the point of contact. The non-testing arm was placed behind the back to avoid compensatory force production. The author chose only the “Y” and “T” positions, excluding the “I” position (180 degrees of abduction) originally included by Ashworth et al, or the “I” position (0 degrees of abduction) included by Trunt et al., due to the relevance of the “Y” and “T” shoulder positions to the common biomechanics of throwing.13,16,17,27–29 In all testing positions the elbow was fully extended (Figure 1). Testing commenced in the “Y” position followed by the “T” position. For each test position and trial, subjects were instructed to push “as hard, and as fast” as possible into a portable force plate (Vald, ForceDecks, Queensland, AU), demonstrating a maximal isometric contraction for at least three seconds. This was repeated for three trials at each testing position, with 10 seconds rest between each trial, and 30 seconds rest between each testing position. Maximal verbal encouragement was provided for each trial and force data was collected at 500 Hz. The entire testing protocol, including warm-up, rest periods, and testing trials was completed in under 10 minutes for each subject. The average peak force in each testing position was recorded, normalized to body weight, and averaged across the nine weeks for analysis. Peak force was normalized to body weight as described by Trunt.25 Limb symmetry indices were also calculated comparing dominant to non-dominant (Right to Left) arms (Table 2). All data analysis was performed on SPSS (version 29.0).
.png)
RESULTS
Descriptive statistics including mean and standard deviation for continuous variables were calculated to characterize the study participants. This initiative examined the three collegiate quarterbacks from an NCAA Division 1 university (Age: 20.00 +/- 1.00 years) (Height: 189 +/- 5.29 cm) (Weight: 88.17+/- 3.99 kg). Athlete anthropometrics and demographics can be found in Table 1.
Data for peak force, peak force normalized to body weight, and limb symmetry indices of three collegiate quarterbacks throughout both the pre-season and regular season, was collected utilizing the ASH test. Peak force means, limb symmetry indices, and peak force normalized to body weight for each individual athlete can be found in Tables 2 and 3.
The mean peak force of all trials of the total study population, in the Y-position was 142.33N (+/- 15.06) on the athletes’ dominant side (R), and 128.00N (+/-20.26) on their non-dominant side (L). The limb symmetry index for peak force in the Y-position was 1.13 (+/-0.15). The dominant limb, in the Y-position, for all athletes produced an average of 13% more force than the non-dominant limb (range: 4%-16%).
In the T-position average peak force production was 134.04N (+/-16.20) on the athletes’ dominant side (R), and 119.44N (+/-18.68) on their non-dominant side (L). The limb symmetry index for peak force in the T-position was 1.14 (+/-0.14). The dominant limb, in the T-position, for all athletes produced an average of 14% more force than the non-dominant limb (range: 9%-19%). When comparing within limbs, it was observed that greater average peak force was observed in the Y-position (RY = 142.33N, RT = 134.04N, LY = 128.00N, LT = 119.44N) compared to the T-position. When analyzing both positions and both arms, athletes generated an average of at least 14% of their body weight in force.
DISCUSSION
The feasibility of using force plates to conduct the ASH test on a population of collegiate quarterbacks was demonstrated throughout this study. ASH testing was initiated for three collegiate quarterbacks due to the high demands on the shoulder from throwing. Over the nine-week period, 100% compliance was ensured by standardizing testing procedures (Figure 2) and conducting the tests in a controlled environment. Each quarterback was tested weekly, in the morning before team practice, on non-game days to reduce the effects of fatigue. A consistent warm-up protocol was provided, and clear instructions were given before each session to ensure participants fully understood the procedures.
Mean peak force was analyzed in each arm position, limb symmetry in each position, and peak force normalized to body weight for each athlete, as well as across the group. This data was shared weekly with the athletic training and strength and conditioning staffs, helping guide their training program development in real time with hopes of improving performance and mitigating the risk of throwing-related injury. The portable design of the force plates, along with the short testing duration (under 10 minutes per athlete), allowed seamless integration of the ASH test into the athletes’ routines. Additionally, the relevance of the “Y” and “T” positions to the throwing mechanics of quarterbacks made the data particularly valuable for assessing upper extremity strength in this specific population.
The second aim, to compare the findings of this study to existing literature from other athletic populations where the ASH test or similar methodologies have been applied, was achieved by observing greater force production in the dominant limb in both the Y- and T- positions, compared to the non-dominant limb. These observations align with findings from prior research in other athletic populations during specific upper extremity isometric tests.25,30–33
Additionally, it has been shown that when using the gold standard method of assessment of isokinetic testing in overhead athletes, the dominant arm is also observed to be stronger than the non-dominant arm.34–36
In both positions and in both arms, athletes on average generated at least 14% of their body weight in force. This observation is consistent with the findings of Trunt et al., who reported that a group of 30 healthy baseball players produced at least 11% of their body weight in force in each testing position and for both arms.25 To improve the quality of the injury and performance assessment battery already implemented by this university, we suggested that the athletic training staff and strength and conditioning staff use this observation of 14% body weight as a proxy for intra-organizational normative values, as a shoulder strength screen for their quarterbacks moving forward. In the lower extremity orthopedic injury and rehabilitation literature, assessing peak force normalized to body has been a strategy utilized when developing recommendations for certain return to sporting activities, for example peak knee extension torque normalized to body weight post ACL reconstruction of 2.07-3.0 Nm/kg has been used as a metric to inform return to sport decisions in field sport athletes.37,38 Similarly, by further investigating peak force normalized to bodyweight in overhead athletes, there is potential to use this measure to guide return to play decision making.
When comparing shoulder positions within limbs, it was observed that greater peak force was observed in the Y-position compared to the T-position. These observations align with previous studies using the ASH test, which showed that athletes tend to produce greater force in the Y-position than in the T-position.23,25,39,40 This result is particularly interesting due to the similarity of the Y-position to the common biomechanics of throwing,41 and compared to other currently practiced orthopedic strength tests, the ASH test uniquely assesses force output in this overhead position and degree of glenohumeral abduction, making it a valuable tool for evaluating quarterbacks. Not only might the ASH test be beneficial to clinicians such as athletic trainers and physical therapists in rehabilitation, but testing peak force in specific positions in healthy throwing athletes may help strength coaches and performance coaches tailor training programs to address positional weaknesses and optimize performance gains.41–43
The third aim of using data to guide strength and conditioning was achieved by utilizing the baseline test measurements in the Y- and T-positions, recorded during week one, as the athlete’s baseline data. Throughout the season the strength coaches compared each week’s test results to those baseline numbers to screen for an increase or decrease of peak isometric force output, potentially providing insight into the athlete’s readiness at that moment in time. If an athlete’s ASH test peak force numbers were below their baseline at any point within those nine weeks, the strength and conditioning staff may have adjusted that athletes programming to improve the quality of their training, rest, and recovery. Until further research on the ASH test is conducted, this is also the recommendation to the staff moving forward in subsequent seasons.
Prior research also shows the use of clinical strength assessments to evaluate a throwers dominant and non-dominant arm strength can elucidate strength deficits and asymmetries that may pre-dispose an overhead athlete to injury.44–46 Moreover, the lower extremity orthopedic rehabilitation literature indicates that peak isometric and isokinetic strength limb symmetry indices (LSI) are instrumental in identifying athletes at risk of injury, those with prior history of injury, guiding return-to-play decisions and informing treatment interventions and training.47–54 We recommend using the ASH test as a pre-season baseline screen and routine monitoring for healthy quarterbacks as well as integrating it into a comprehensive test battery for overhead athletes returning from injury. Establishing a healthy baseline limb symmetry index at the start of the season might provide a valuable reference point for monitoring arm health and readiness throughout the year. This enables the assessment of arm condition before and after competitions, training blocks or cycles, or during rehabilitation. Additionally, post-competition and pre/post-training testing should be further investigated as it may help quantify fatigue levels and inform daily training adjustments.
Analyzing peak force measurements, inter-limb strength asymmetries and peak force normalized to body weight may highlight strength deficits and imbalances, thereby informing strength and conditioning programming or return to sport decisions. With further understanding of the ASH test we are hopeful that it may eventually aid in injury prevention screening and also enhance performance by tailoring training to each athlete’s specific needs. Understanding upper extremity performance, neuromuscular fatigue, and ability to transfer force across the shoulder girdle in quarterbacks may inform injury prevention strategies and may help optimize player health and performance. Assessment of shoulder strength may be an important contribution to objectively inform clinical decisions when returning an injured overhead athlete back to sport55 and could inform training strategies aimed at improving throwing performance and reducing injury risk in healthy athletes.45,56–59
Results of ASH testing may help rehabilitation and performance professionals with exercise prescription to enhance overall performance and mitigate injury risk.59,60 Given the specific demands of throwing athletes like quarterbacks, who demonstrate positions with large shoulder abduction angles, it might be helpful to tailor strength assessments to the athlete’s specific movement patterns and positions. Testing overhead athletes in throwing relevant positions, whether in the “T” or “Y,” may provide results that are similar to their sport-specific positions, supporting the need for further research using the ASH test. Understanding the athletic demands of overhead athletes is paramount, as they often demonstrate long lever movement strategies at large degrees of shoulder abduction, increased shoulder torque requirements, and generate high forces. Therefore, integrating the ASH test into an assessment framework aligns with these demands.
This case series demonstrates the feasibility and clinical utility of the ASH test in collegiate quarterbacks. Observations from this study and the current literature support the recommendation to further investigate the use of the ASH test in quarterbacks to establish validity, reliability, and normative values, as well as monitor trends over time. The ASH test may be a helpful tool to assist the rehabilitation and performance team as it may assist decision making regarding an overhead athlete’s readiness to practice or compete. For example, Wollin et al, demonstrated that through monthly monitoring of hip and groin isometric strength using dynamometry in healthy soccer players in season, they could track strength changes over time, identifying players who were either experiencing or at risk of developing an injury.61 Additionally, monitoring changes in strength metrics and peak force overtime using the ASH test allows for the evaluation of training effectiveness and adjustment of training protocols to ensure optimal performance outcomes.42,62
In this study, limb symmetry index data from the ASH test was used in-season by the team’s strength coaches to improve the quality of their strength and conditioning programming. For example, when a quarterback’s LSI fell below 1.0 (dominant compared to non-dominant) athletes training volume load and prescribed intensities were further analyzed by the strength and conditioning staff and guided adjustments to their programming that they deemed necessary. Findings from this study, alongside existing literature, support the ASH test’s broader use as a profiling, monitoring, and return-to-performance tool, ensuring overhead athletes are adequately prepared for the high demands of their sport. Further investigation into the ASH test’s validity and reliability is warranted, but it already serves as an excellent starting point for understanding the upper body strength profiles of overhead athletes and guiding targeted interventions to improve performance and ensure long-term athletic health.
In addition to the utility of isometric peak force testing, it is worth acknowledging the value of incorporating dynamic and functional assessments into shoulder evaluation and performance profiling for overhead athletes. Tests such as the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) may provide complementary insight into neuromuscular control, endurance, proprioception, and shoulder stability. The CKCUEST has been shown to predict in-season shoulder injury in collegiate football players, with a threshold of 21 touches as having high sensitivity and specificity.63 Furthermore, Kadlec et al. demonstrated that CKCUEST outcomes had only modest correlations with traditional single-joint (e.g., external/internal rotation) and multi-joint (e.g., bench press) strength tests, reinforcing that these different assessments measure distinct physiological qualities.40 Notably, the strength and conditioning staff at this university already employs multi-joint dynamic tests like the bench press and pull-ups as part of their athlete profiling battery. Integrating a validated dynamic test like the CKCUEST alongside these existing tools, and in conjunction with isometric assessments like the ASH test, may provide a more complete picture of shoulder function, particularly when monitoring in-season fatigue or evaluating readiness to return to play. Future research should explore the relationship between ASH test metrics and dynamic tests, like the CKCUEST performance to better understand how static and dynamic measures can be combined to enhance upper extremity profiling and individualized programming for quarterbacks and other overhead athletes.
This study has several limitations that should be acknowledged. A significant limitation is the limitation associated with the small sample size included in this case series, which limits the generalizability of the findings. Additionally, athletes were not tested on the same day of the week each week, which could have affected consistency. The data collection period was limited to nine weeks, which may not be sufficient to observe long-term trends or effects. The athletes were from a single institution and consisted solely of elite Division 1 athletes, making the results less applicable to the general population or athletes from different competitive levels or institutions.
This study adds to the body of literature exploring the utility of the ASH test in overhead athletes in a single sport. Future research to explore cross-sport comparisons of ASH test performance among overhead athletes is warranted. While prior studies have investigated the ASH test in rugby, softball, and baseball populations, this study is the first to explore its application in collegiate football quarterbacks, a group with unique biomechanical demands but similar long-lever overhead force requirements. Comparing data across these overhead athlete populations could possibly reveal both shared strength profiles and sport-specific adaptations, which could inform normative values, return-to-play benchmarks, and training strategies. Future research should aim to establish comparative ASH test profiles across these sports to better understand upper extremity performance demands and guide individualized performance and rehabilitation programming.
CONCLUSION
The results of this case series indicate that the ASH test demonstrates potential in assessing the performance of NCAA Division I collegiate quarterbacks at this one institution. The findings suggest that the ASH test is effective in measuring isometric peak force and identifying inter-limb strength asymmetries, which can be helpful information for developing tailored strength assessments, training interventions, and performance enhancement programs. The integration of the ASH test into preseason and in-season monitoring may provide a valuable reference for evaluating arm health and readiness levels, informing training adjustments, and ensuring athletes can handle training volumes and intensities. Despite the need for further research to establish its validity and reliability, the ASH test may be a practical tool for profiling, monitoring, assessing injury risk, and assisting overhead athletes towards peak performance. By analyzing sport-specific positions, it offers a nuanced understanding of upper body strength, aiding in injury prevention and performance optimization for quarterbacks and other overhead athletes.
Corresponding author
Carmen Sclafani
3318 Long Point Drive
Toms River, NJ 08753
(p) (732)-608-3455
carmen@resilientperformance.com
Conflicts of Interest
The authors report no conflicts of interest