
INTRODUCTION
In multidirectional sports, lower limb non-contact injuries (LLNCI) predominantly occur during unilateral foot contact, involving frequent movements outside the sagittal plane such as landing and cutting.1,2 One of the key modifiable risk factors for LLNCI is the way a player moves and also the internal forces they are exposed to. Systematic reviews have identified altered kinematics associated with and/or predictive for overuse and acute LLNCI such as patellofemoral pain syndrome (PFPS), patellar tendinopathy, groin injuries, exertional medial tibial pain, and anterior cruciate ligament (ACL) during landing3–7 and single-leg squats (SLS).7,8 Considering this, regular screening of kinematics during single-leg tasks might help to identify injury risk and monitor rehabilitation.
Three-dimensional (3D) marker-based motion analysis is considered the de facto standard for movement quantification.9 However, there are limitations such as high cost, time-consuming data collection and analysis, marker placement error, and the requirement of laboratory-based testing.10 These factors make repeated screening of athletes, especially across whole squads challenging. To address this, technologies such as wearable inertial measurement units11 and markerless motion capture systems12 have been developed to enable more frequent measurements during sports activities. Markerless motion capture is an evolving technology presenting an alternative measurement of human movement.12 These systems often use two-dimensional video cameras or depth sensors in combination with machine learning algorithms to estimate human body segment positions and orientations during physical tasks.10,12 However, before assessing the changes in risk factors, tools need to be reliable to accurately assess the status of the athlete and any changes that may occur. Reliability concerns the extent to which repeated measurements provide similar results over time.13 Reliable outcome measures provide information to differentiate between a real change observed or a measurement error (i.e., systematic bias and random error or noise).13 This allows tests to be used with confidence when identifying athletes at risk of injury or monitoring rehabilitation.
Studies on the reliability of markerless motion capture have investigated trunk and lower limb kinematics during squats14–20 and landing tasks.14,15,19,21,22 However, most of the studies have focused on double-leg movements, which might not accurately replicate the injury risk maneuvers associated with LLNCI in multidirectional sports, often occurring during single-leg activities and outside the sagittal plane.23 Only a few of those studies have investigated single-leg tasks for squats15,19 and landing.14,19,22 Moreover, landing tasks have predominately been performed in the sagittal plane, with only one study19 investigating frontal plane landings (e.g., lateral landings).
Regarding the markerless system employed, studies assessing the reliability of single-leg tasks have used a limited number of cameras, including one14,15,22 and two cameras.19 Studies investigating markerless technology24,25 have demonstrated that multi-camera systems have superior agreement and reliability in capturing movement compared to single-camera systems. Single-camera systems present limitations including restricted capture volume, self-occlusion, and dependence on camera placement.10,12 Additionally, these studies have used different pose estimation models such as Microsoft Kinect Software Development Kit,15 OpenPose,19 HumanTrack (VALD),14 and MediaPipe.22 No studies to date have used Theia3D markerless motion capture system to assess the reliability of single-leg tasks. Theia3D is a commercially available markerless motion capture system that employs a machine learning algorithm and a multi-camera setup for data capture and processing.26 Conversely, marker-based motion capture studies have investigated the reliability of kinematic variables during single-leg tasks in both the sagittal27,28 and frontal plane.29,30 However, variations in protocols (e.g., task types) exist among these studies.
Therefore, investigating the reliability of data acquired using a multicamera system during single-leg movements is necessary to confirm findings from previous studies and improve the clinical applicability of markerless motion capture in sports. Additionally, exploring the reliability of marker-based motion capture using an identical protocol can help to compare the reliability between the two technologies. The primary aim was to examine the between-day reliability of trunk and lower limb kinematics during single-leg squat and single-leg landing tasks using markerless motion capture. The secondary aim was to examine the between-day reliability of the same protocol using marker-based motion capture.
METHODS
Participants
Recreational athletes were recruited (defined as participating in physical activity for at least one hour, three times a week). Since the goal of this reliability study was to know if the variables were reliable, a hypothesis testing approach was implemented to calculate the sample size.31 To demonstrate that the ICC is at least 0.8 (i.e., good reliability), performing two measures, with 80% statistical power, 0.5 of significance level, a dropout of 10%, and suspecting that the true ICC is 0.95 a sample size of 18 was needed. The suspected ICC was based on a study investigating the reliability of the same variables.27 Additionally, a separate study including 10 different participants of similar characteristics was conducted to examine the between-day reliability of marker-based motion capture (Appendix 1). Exclusion criteria included surgery to lower limbs in the prior 12 months and any pain in the two weeks before the study that interfered with the ability to train or compete fully.27 This study was approved by the university’s ethics board and conducted in accordance with the Declaration of Helsinki (Application ID: 5219).
Procedures
Participants performed two sessions separated by a week. For the assessment of markerless motion capture eight cameras (Qualisys Miqus, 3 Megapixel resolution video cameras collecting at 100Hz) measured lower limb kinematics during a set of tasks. For marker-based motion capture, a 10-camera Qualisys (Qualisys, Sweden) OQUS3 motion analysis system (collected at 100 Hz) was used (Appendix 1). In both set-ups, three force plates (AMTI. USA collecting at 1000 Hz) embedded in the ground were used to identify the initial contact during the landing tasks. Participants underwent a 5-minute warm-up on a bike. Then, three tasks were recorded in the following order: SLS, forward landing, and medial landing. Tasks were selected for their relevance to LLNCI mechanisms and rehabilitation. Landing is a key injury mechanism for ACL injuries,1,2 and is typically assessed in later stages of rehabilitation. Although SLS is not an injury mechanism, it is commonly used in early rehabilitation, and movement alterations during this task have been observed in individuals with PFPS.7
Single Leg Squat
The SLS is a functional clinical test used by clinicians in the musculoskeletal assessment of the lower limb.32 Participants stood on one leg (hip and knee extended in a natural stance position, arms by sides, and opposite thigh held vertical with knee flexed 90°). Then, they squatted down on the weight-bearing leg to a depth similar to what is needed to sit onto a chair over a 5-second period (descend over two seconds, hold one second, and ascend over two seconds).27 This reduced the effects of speed on knee angles and movement patterns.27 The squat depth was not controlled in order to maintain a method that is most similar to clinical practice.27
Single Leg Hops
Single-leg hop tests were chosen over double-leg hops as the latter may not fully represent the biomechanical demands during high-injury risk activities in multidirectional sports.33 It has been shown that single-leg hops elicit greater joint moments and more rigid landings (i.e., less knee and hip flexion angles, which have been reported as risk factors) than double-leg hops.34 Forward landing was assessed due to the high contribution of the knee joint (65%).34 Additionally, the landing was assessed in the medial direction due to their different demands - landings after frontal plane movements elicited more predominant signs of dynamic lower extremity valgus.33 Therefore, a combination of these two planes of movement might provide more information on the monitoring of injury and rehabilitation in athletes. Details of the landing tasks can be found in Appendix 2.
Forward Landing
Participants stood on one leg (hip and knee extended in a natural stance position arms relaxed by sides, and opposite thigh held vertical with knee flexed 90°). Then, they performed three forward 1m hops onto the force plates. The researchers ensured that balance was held for a minimum of 3 seconds on the final landing.27
Medial Landing
Participants stood on one leg (hip and knee extended in a natural stance position arms relaxed by sides, and opposite thigh held vertical with knee flexed 90°). Then, they performed one forward 1 m hop and one medial 0.60m hop onto the force plate. A medial hop distance of 0.60m was chosen, as it was found to be both achievable and appropriately challenging for all participants. This decision is supported by studies that utilized similar distances (with a mean of 40cm) for both medial and lateral landings.30,35 The researchers ensured that balance was held for a minimum of 3 seconds on the final hop.27
Before data collection, each participant was allowed one to three practice trials on each leg. Five trials of each test were performed on both limbs, and the results across trials were averaged for the right and left limbs separately. Rest periods of 15 seconds were given between tasks and trials to minimise fatigue. The same location and testing procedure (e.g., warm-up, tasks, and visits to the lab) were used to assess the reliability of marker-based motion capture (Appendix 1).
Data Processing
Video data were processed using Theia3D (v2022.1.0.2309, Theia Markerless Inc., Kingston, ON, Canada) to obtain 3D subject body segment positions and orientations estimates of lower limbs segments and trunk. The resulting pose estimates for each body segment were exported to Visual3D Professional (v2021.06.02, C-Motion, Inc., Germantown, MD, USA) for further analysis.26 Theia3D creates an skeletal model automatically in Visual3D by tracking the pose matrices.26 By default, the lower body joints have six degrees-of-freedom (DOF) at the pelvis and three DOF at the hip, knee, and ankle.26 Kinematic variables during the stance phase were analyzed for the trunk, hip, knee, and ankle. The following variables were calculated based on their frequent use in studies examining potential biomechanical risk factors for NCI in multidirectional sports3–8: trunk flexion and ipsilateral inclination; hip flexion, adduction, and internal rotation; knee flexion and abduction; and ankle dorsiflexion.
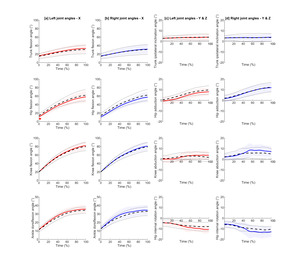
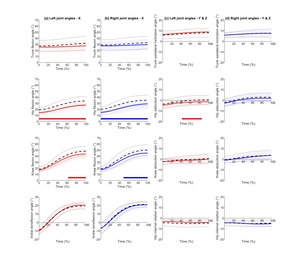
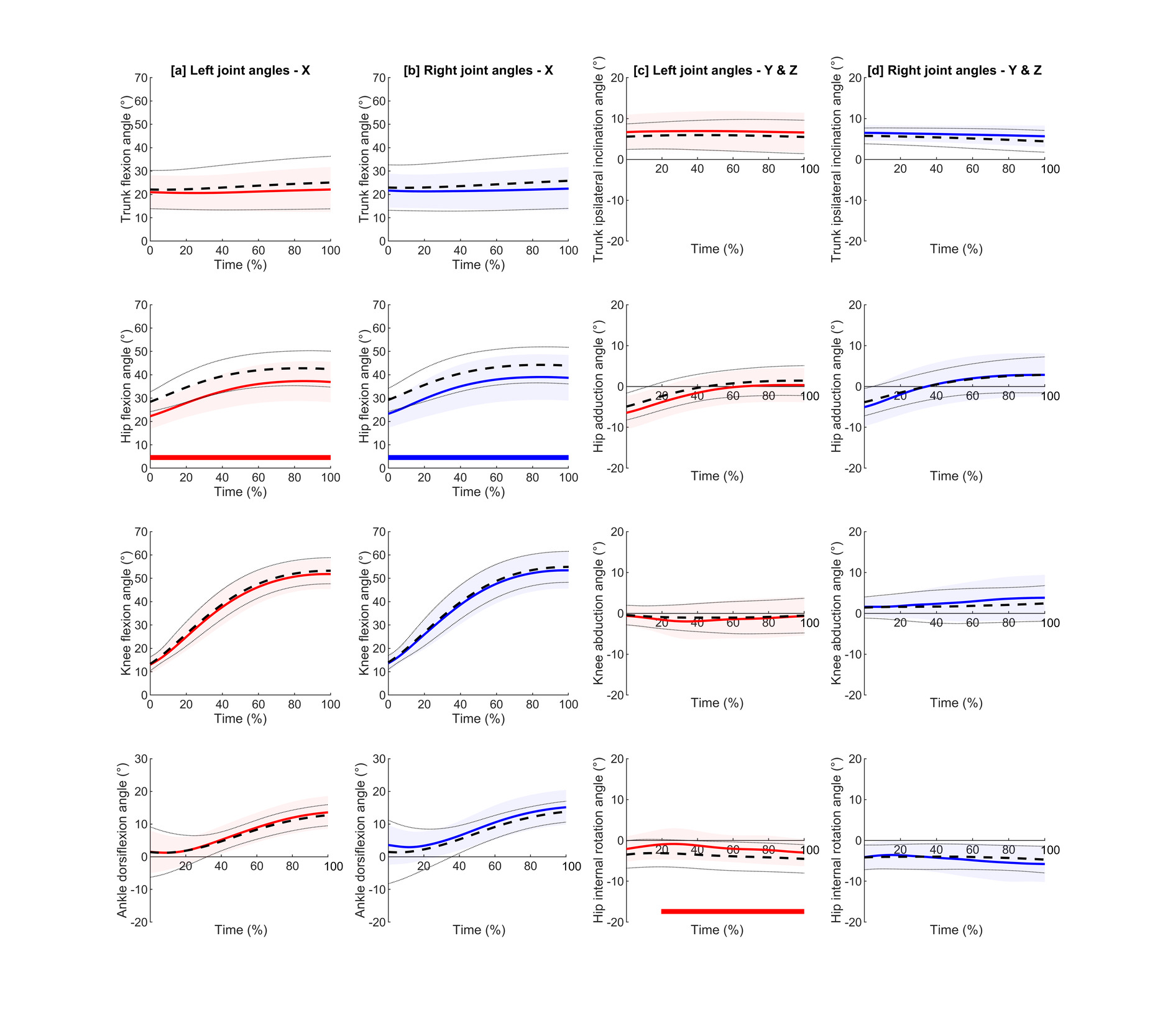
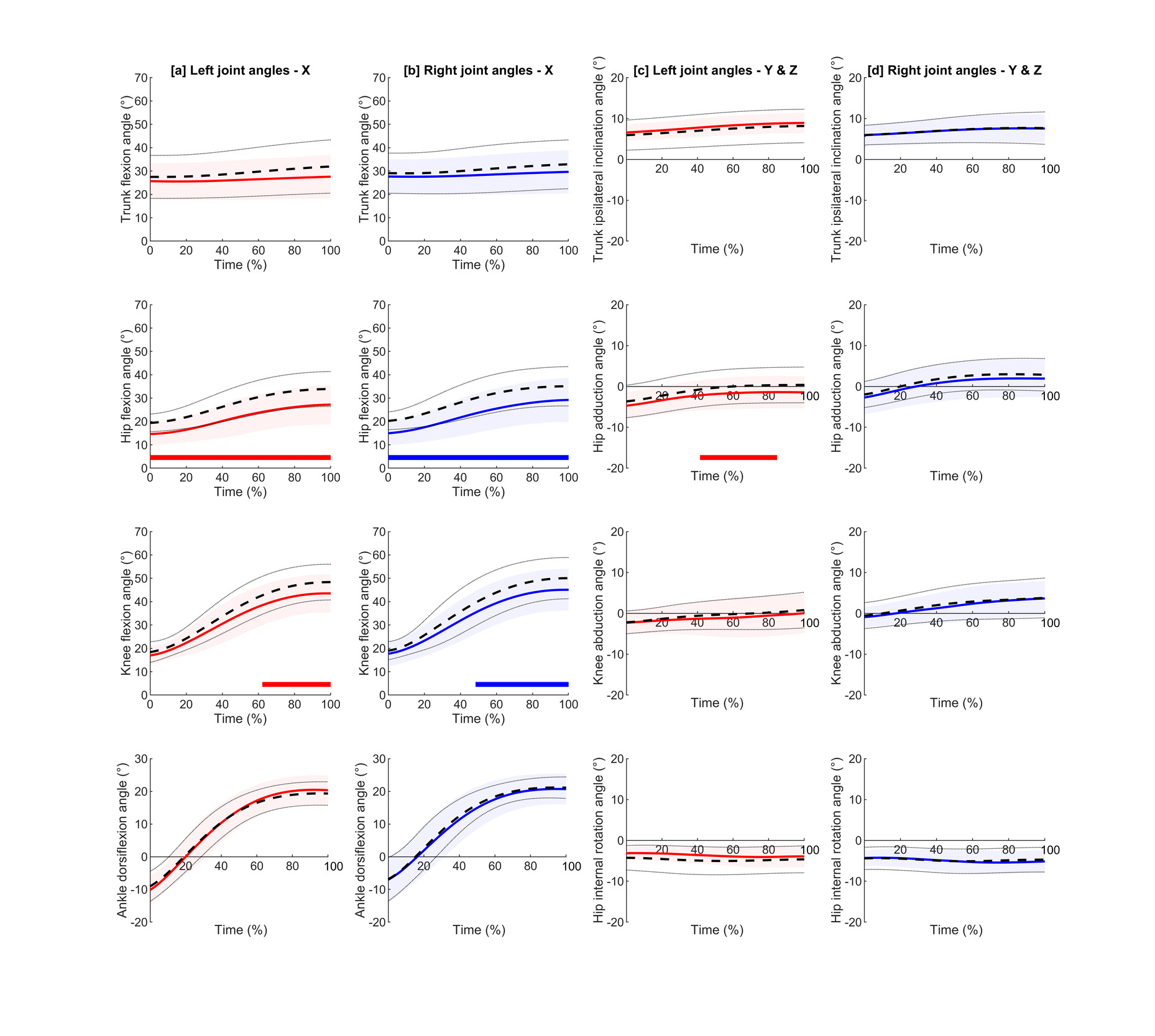
Landing tasks were time normalized from initial contact to the point of maximum knee flexion, which was considered the end of the weight acceptance phase.36 Initial contact was defined as the instant after ground contact, when the vertical GRF was higher than 20 N.36 For the hop tasks, only the last hop (i.e., landing) was analysed as this represents one of the most important mechanisms of injury in multidirectional sports.1,2 SLS trials were normalized from 20° of knee flexion angle to the point of maximum knee flexion. This angle was chosen as it was the angle that all the participants achieved in the test and retest sessions as a starting point. For marker-based motion capture, raw data were labelled through Qualisys Track Manager Software (version 2.16) and kinematic variables were calculated using the 6DOF model in Visual3D software (Appendix 1). Measurement errors of kinematics were examined by both full curve and discrete point analysis. Full curve examination provides the ability to detect possible differences that may not be detected using discrete analysis. For discrete point analysis, the instant of interest for SLS was the peak knee flexion.37 For landing tasks, initial contact and peak knee flexion were analysed. Reduction of peak knee flexion angle during landing tasks has been associated with the development of non-contact knee injuries such as PFPS3 and has been reported in patients following ACL reconstruction.5 Initial contact was included in the analysis due to its association with the ACL injury mechanism.2 Joint angles for each joint were extracted at these events.
Statistical Analysis
Three statistical methods were used to report reliability: systematic bias (i.e., change in the mean), relative reliability (i.e., test-retest correlation) and absolute reliability (i.e., repeated-measurement variability).38 For full curve analysis, one-dimensional (1-D) statistical parametric mapping (SPM) was implemented in Matlab (MATLAB R2021a, MathWorks) using the open-source spm1d code (spm1d version M.0.4.10).39 Two-tailed SPM paired 1-D t-test with a Sidak corrected alpha level of 0.05 was calculated. It has been suggested the use of paired t-test for the detection of large systematic bias between sessions.38 All analyses were performed for both markerless and marker-based motion capture, except for SPM, which was applied only to markerless data. Additionally, the root-mean-square differences (RMSD) were calculated to evaluate between-day differences in the full curves of all joints and planes of motion. For discrete point analysis, relative and absolute reliability were analysed. For relative reliability intraclass correlation coefficients (ICC) with a 95% confidence interval (CI) were calculated (i.e., the degree to which individuals maintain their position in a sample).13 Model 3 (two-way mixed) type absolute agreement with an average of five measurements was used (3,5). ICC >0.90 was considered excellent reliability, between 0.90 and 0.75 good reliability, between 0.75 and 0.50 moderate reliability, and <0.50 low reliability.40 Absolute reliability (i.e., the degree which repeated measurements vary for individuals) was calculated using the standard error of measurement (SEM) and minimal detectable change (MDC). These parameters are easy to interpret as they are expressed in the actual scale of measurement.13 SEM was calculated as the SD of the difference between trials divided by √2.41 The SEM can be interpreted as a reference interval with a coverage probability that approximates to 68% of all true scores in a population.41 The MDC with a 95% confidence level was also calculated, which can be considered an extension of the SEM.38 MDC was calculated using the following formula41: MDC95= SEM x 1.96 x √2. Measurement error was considered low if SEM was <5° as this amount of error has been considered clinically acceptable for biomechanical variables.42,43
RESULTS
Nineteen participants were included in markerless motion capture analysis (age= 27.4±6.5 years, height= 176.5.8±6.7, mass= 73.6±9.3). Their primary physical activity included football (68.4%), running (20.1%), rugby (10.5%), and basketball (5.3%). Participants included in the marker-based analysis (n=10) had similar demographic characteristics and primary physical activity (Appendix 1).
RMSD and SEM values (Tables 1-4) for all tasks were <5° for most of the variables using markerless technology, suggesting acceptable absolute reliability.42 Only hip flexion presented values >5° in all tasks for the full curve analysis (5° to 7°) and in SLS for discrete point analysis (6°). SPM showed statistical differences for bilateral hip flexion (full curve) and unilateral hip adduction, hip rotation, and knee flexion during a specific percentage of the landing tasks (Figures 1-3). All variables reported moderate to excellent relative reliability, except for hip rotation during SLS which showed low reliability (ICC= 0.16 to 0.41). Similarly, most variables presented RMSD and SEM values <5° using marker-based motion capture. Only hip and trunk flexion during SLS (both full and discrete curve analyses) and ankle dorsiflexion at initial contact during landing reported values >5° (6° to 8°). All variables reported moderate to excellent relative reliability. Discrete point analysis showed similar relative and absolute values at initial contact and max knee flexion in landing tasks for both technologies.

DISCUSSION
To the authors’ knowledge, this is the first study to investigate the reliability of markerless motion capture of single-leg tasks using Theia3D. Most of the assessed variables presented an error <5° for full curve (RMSD) and discrete variable (SEM) analysis using markerless motion capture. The highest errors were found in hip flexion for full curve analysis across all tasks (RMSD between 5° to 7°), with SPM showing statistical difference (0-100% of the task) for the hop tasks indicating possible systematic bias. Furthermore, all variables showed at least a moderate level of relative reliability, except for hip rotation in SLS which showed low reliability. When using the same protocol, despite having different subjects, marker-based motion capture reported similar, or slightly higher between-day error compared to markerless motion capture, with hip flexion angle also being the variable with the highest error. Regarding relative reliability, all variables also showed at least moderate reliability, but with mean values slightly higher than markerless motion capture. Overall, the results show markerless motion capture has low between-day error during single-leg tasks which is comparable to marker-based motion capture.
Parameters such as SEM and RMSD will be mainly discussed and compared to the literature because of their clinical relevance (expressed in the actual scale of measurement). Determining reliability only based on ICC values may lead to erroneous conclusions.13 For instance, right hip IR in markerless motion capture during SLS reported poor reliability (ICC= 0.16), whereas marker-based motion capture presented good reliability (ICC= 0.89). Based on these results, we might assume that markerless motion capture is less reliable. However, based on absolute reliability parameters, both present similar SEM values (markerless= 3.4°; marker-based= 3.8°). The lower ICC found in markerless might be due to lower between-subject variability (SD= ±3.4°) compared to marker-based motion capture (SD= ±8.2°), despite similar within-subject trial-to-trial variability (3.1° vs 2.9°). If there is a small inter-subject variability, small ICC values may be reported even if trial-to-trial variability is low; small differences between subjects are more difficult to detect than large ones, impacting the ICC value.13,41 Although an ICC will show if the instrument can differentiate between patients, it does not provide within-subject trial-to-trial variability which is important and useful for practitioners.13
Single Leg Squat
All variables, except for hip flexion, reported absolute reliability values below 5˚ for both discrete and full curve analyses, demonstrating the reliability of markerless technology during SLS. Due to the association with injuries,7 the results of this study will be compared to studies evaluating single-leg squats.15,19 Mentiplay et al.15 investigated the between-day reliability of trunk and lower limb kinematics at maximum knee flexion angle during SLS in the sagittal and frontal planes. The SEM values (2.8° to 7.8°) were similar to those observed in the present study (SEM 2.1° to 6.0°) for the same variables. Similarly, Lima et al.19 recently examined the between-day reliability of trunk and lower limb kinematics using markerless motion capture during SLS at initial contact and peak angles, including the transverse plane in their analysis. For absolute reliability parameters, the authors reported MDC values ranging from 5.3˚ to 17.5˚, which also aligns with the findings of this study (MDC=4.7˚ to 16.7˚). Despite the different pose estimation models used, the measurement errors found in this study for SLS are comparable to the literature.
Regarding specific variables associated with injuries, greater ipsilateral trunk inclination during SLS has been found in individuals with PFP.7 This strategy is reported to compensate for hip abductor weakness in individuals with PFP and may increase knee valgus moment.44 Mentiplay et al.15 did not report trunk inclination, whereas Lima et al.19 found MDC ranging between 7.9˚ and 8.2˚ at initial contact and peak angles. The current study found lower MDC values (5.4˚ to 6.2˚) for discrete analysis. Importantly, the present study also included full curve analysis, showing RMSD for trunk inclination between 2.0˚ and 2.3˚, with the SPM curve showing no statistically significant differences. The results increase the confidence in the use of markerless motion capture for the monitoring of this variable in the clinical setting.
Landing
Similar to SLS, most variables during landing tasks showed absolute reliability values below 5˚ for discrete and full curve analyses, except for hip flexion. Three studies14,19,22 have investigated the reliability of markerless motion capture during single-leg landing tasks. McCarthy et al.14 found higher SEM values for intrarater reliability of knee and hip kinematics in the sagittal plane during single-leg drop jump task (6.6° to 9.3°) compared to forward (1.9° to 3.0°) and medial landing tasks (1.7° to 4.0°) reported in this study. Similarly, using markerless motion capture, Lima et al.19 also found higher MDC values ranging from 6.6˚ to 23.6˚ for single-leg forward and side hops (lateral direction), than this study (1.5˚ to 12.4˚). A recent study conducted by Asaeda et al.22 specifically investigated the intrarater reliability of knee valgus angle during single-leg landing using markerless motion capture. However, they only reported relative reliability parameters. Their results (ICC=0.69 to 0.89) are comparable to those reported in this study (ICC=0.51 to 0.98) for knee valgus. The lack of absolute reliability parameters limits the ability to make more clinically meaningful comparisons.
One possible explanation for the lower SEM and MDC values observed in the landing tasks of this study could be the greater number of cameras and the higher capture rates used. This study used eight video cameras with a capture rate of 100Hz, whereas previous studies assessing absolute reliability during landing tasks used a single depth-sensing camera at 30Hz15 or two mobile devices at 60Hz.19 Considering that SLS results were consistent with the literature, the number of cameras and capture rate did not impact the results for this task. However, the errors in landing tasks in this study were significantly lower than those reported in the literature. Since landing is a faster and more demanding task, the higher capture rates used in the present study could explain the results. Pose estimation performance is suggested to depend on the task, as higher limb velocities may introduce image noise in the form of blur, which can affect joint center detection in markerless motion capture.9 The use of digital video cameras with higher resolution and capture rates is recommended for evaluating sports-related tasks such as landing or running.45 Although this might explain the superior results of this study, further research is needed to confirm these findings.
ACL injuries often occur during single-leg landing tasks at initial contact, which is associated with an increased knee valgus loading.2 This study showed low SEM (0.5˚ to 1.0˚) and MDC values (1.5˚ to 2.8˚) for knee abduction at initial contact during both landing tasks. However, Lima et al.19 and McCarthy et al.14 did not include knee abduction in their analyses, so no comparisons can be made. Although Asaeda et al.22 calculated knee abduction angle during single-leg landing, only ICC values were reported, which enabled absolute reliability comparisons. Another variable to consider during landing is the knee flexion angle. ACL injuries mainly occur in early knee flexion during landing,2 whereas reduction of knee peak flexion angle during landing has been associated with the development of PFPS3 and reported in patients following ACL reconstruction.5 This study reported low knee flexion values at both initial contact (SEM=1.4˚ to 2.5˚; MDC=4.0˚ to 6.8˚) and peak angle (SEM=2.9˚ to 3.2˚; MDC=7.9˚ to 8.8˚). Although Lima et al.19 found similar results for side hop, the forward hop task reported higher values at initial contact (MDC=23.6˚). Similarly, McCarthy et al.14 found higher values at peak knee flexion (SEM=7.8˚; MDC=21.5˚) for single-leg drop jump. This study provides low absolute reliability values for knee abduction and flexion angles compared to the literature during landing tasks.
Comparison with Marker-Based Motion Capture
Markerless demonstrated similar or slightly superior absolute reliability compared to marker-based motion capture. This minor difference might be attributed to the error introduced by marker placement.46 The results obtained with the reliability of marker-based motion capture are similar to the literature investigating SLS and single-leg landing tasks in both the sagittal27,28 and frontal plane.29,30 Regarding the variables, hip flexion exhibited the greatest error in both technologies, which is in agreement with the literature.14,15,27 In markerless motion capture, the difference in hip flexion exceeded 5° but was less than 7° across all tasks, but this was solely observed in the full curve analysis. This variation was confirmed by the SPM analysis, showing statistical differences between trials (i.e., the second session had a lower mean hip flexion angle) during the whole landing tasks, possibly indicating systematic bias. Systematic bias is consistent in direction and magnitude (e.g., learning effects or participant fatigue), while random error varies (e.g., due to mechanical or biological variation and measurement protocol inconsistencies).38 To reduce systematic bias, participants performed practice trials to familiarize themselves with the tests and had sufficient rest periods between trials to avoid fatigue. Despite this, learning effects associated with landing strategies in some participants might explain the differences in hip flexion angle. Since no studies using Theia3D have examined the reliability of single-leg landing tasks, further research is required to determine whether the systematic errors in hip flexion angle are attributed to learning effects or to the characteristics of the task.
Limitations
As with any study, there are limitations in that the measurements were performed in a controlled laboratory setting, which might not represent the environment where this new technology may be used to screen athletes. To the authors’ knowledge, the reliability of Theia3D has only been investigated outside a laboratory setting in the study conducted by Riazati et al.47 Future research should focus on the ecological validity of markerless technology by capturing data in real-world environments. However, this approach requires caution, as this may compromise internal validity due to the difficulty of controlling task performance outside a lab setting. Secondly, the results obtained are specific to the Theia3D software and may not be necessarily transferrable to other markerless motion capture methods such as Microsoft Kinect Software Development Kit, OpenPose, HumanTrack (VALD), and MediaPipe. However, due to the lack of studies investigating the reliability of single-leg tasks using Theia3D, the results had to be compared to existing literature using other pose estimation methods. Since Theia3D detects a higher number of key points during tracking than some open-source pose estimation algorithms,10 the current results might explain the superiority of Theia particularly during landing tasks. However, further research comparing Theia with other markerless motion capture methods is needed to confirm this. Thirdly, the comparison between markerless and marker-based motion capture would have been influenced by the differences in participants and sample size. To mitigate this, participants with similar characteristics were included and the same protocol was performed for both technologies. Finally, this study only included landing and squat tasks, which may not represent the broader range of movements associated with sports-related injuries. Tasks such as running48 and cutting,2 also linked to LLNCI, were not examined and represent a potential limitation. Additionally, the tasks included were performed at a submaximal level, which might affect their associations with injury risk. However, repeated screening of maximal tasks within a sports environment with a strict training regime and periods of match congestion might not be appropriate due to possible increased injury risk as well as being perceived as unsafe among coaches.49
CONCLUSIONS
Markerless motion capture using Theia3D can reliably measure single-leg tasks with measurement errors comparable to marker-based motion capture. The low measurement error provides confidence for monitoring or screening athletes during single-leg tasks and allows for quicker assessments which are advantageous for elite screening.
Acknowledgements
This work was supported by the University of Salford and Machine Learning in Athletics.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.