


INTRODUCTION
Shoulder problems are common in handball, affecting both male and female players. Authors have reported a weekly prevalence of shoulder problems ranging from 23%-28%1–4 with female players exhibiting a higher prevalence and severity compared to males.2,4 Substantial shoulder problems, defined as problems leading to moderate or severe reductions in sports performance or total inability to participate,5 are particular common among females athletes, who are more frequently affected in their dominant arm6 and face a greater risk of traumatic injuries compared to male players.7 Factors thought to contribute to shoulder problems in female handball players include shoulder strength and, specifically, pre-season weakness of isometric external rotation (ER) and isometric internal rotation (IR) has shown an association with increased shoulder injury rate.6 Moreover, results from Myklebust et al., on Norwegian female players, demonstrated a significantly higher proportion of players with shoulder pain had clinical signs of shoulder instability compared to those without shoulder pain.8
The act of throwing involves the entire kinetic chain, a coordinated sequence of energy transfer from the lower extremities through the trunk to the shoulder.9 Efficient kinetic chain mechanics are vital for reducing the load on more distal segments such as the shoulder. Disruptions within the kinetic chain, such as reduced lower body strength (LBS), have been postulated to increase the risk of shoulder injuries.9 A cross-sectional study in baseball pitchers has shown an association between sub-optimal kinetic chain function during pitching and increased shoulder load10 although prospective evidence to confirm this relationship is still lacking. Two studies have demonstrated positive effects of an exercise program specifically designed to reduce shoulder problems in a mixed cohort of male and female handball players.11,12 Notably, these programs included not only specific shoulder strengthening exercises but also trunk rotation strengthening exercises, highlighting the likely importance of the kinetic chain for shoulder problems. However, the specific contribution of trunk rotation strengthening to reducing shoulder problems prevalence12 and shoulder injury rates11 remains unclear.
The interaction between load and intrinsic risk factors is critical in understanding shoulder problems. Internal load, measured previously as participation-related shoulder load (PSL),13 reflects the perceived physiological load on the shoulder and may capture the chaotic and variable nature of handball. External load, such as the number of shots or passes, is more objective but might be a narrower measurement of shoulder stress. The optimal approach to document load in this context remains under consideration.14 A recent study showed that male handball players with reduced pre-season trunk rotation power (TRP) reported more severe shoulder problems as the PSL increased throughout the season.13 However, these relationships have not been explored in female athletes, highlighting a significant gender gap in sports injury research.15
Therefore, the aim of this study was to assess; A) whether pre-season LBS, TRP, and shoulder strength were associated with shoulder problems in female handball players; B) whether internal or external load measurements showed a more consistent association with shoulder problems, and C) whether pre-season strength and power influenced the association between load and shoulder problems.
The hypotheses were that: A) negative association would be seen between pre-season strength and power and shoulder problems for handball players during a regular season; B) internal load measurement would show a more consistent association with the severity of shoulder problems compared to external load, and c) magnitude of pre-season strength and power would influence the strength of the association between load and severity of shoulder problems.
MATERIALS ANDS METHODS
Study Design and Participants
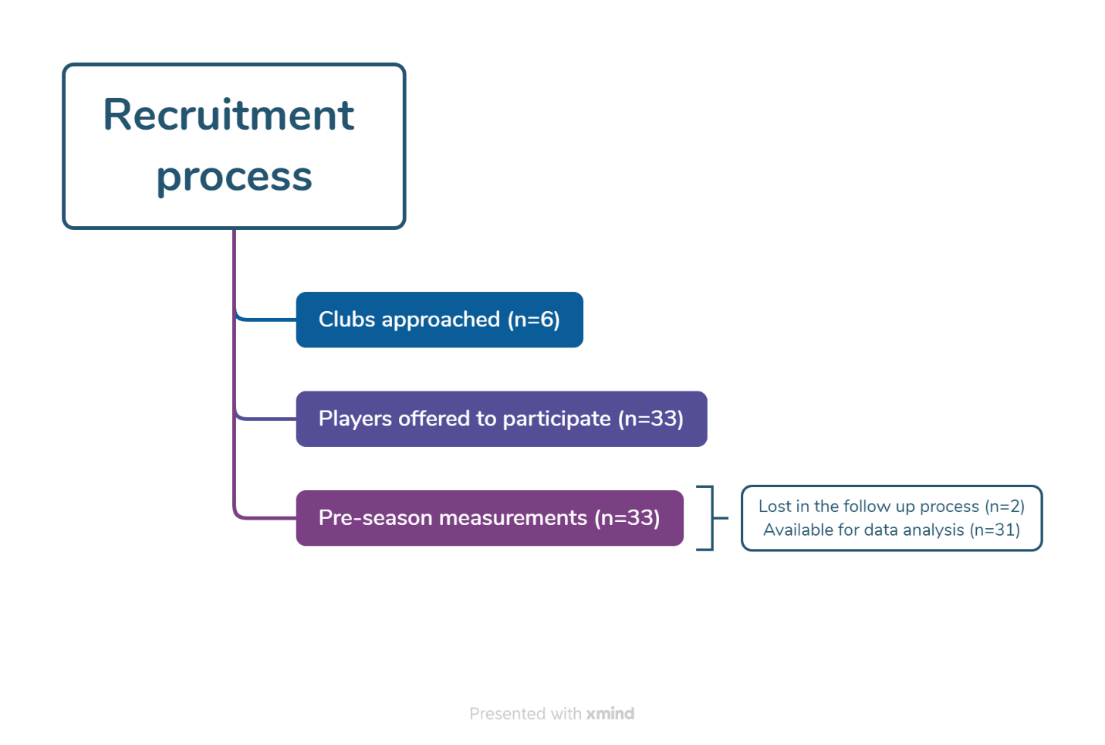
This prospective cohort study involved 33 outfield female handball players (18 years and older) from six top division teams. Pre-season strength and power measurements were conducted at the Research Center of Rehabilitation and Movement Science, University of Iceland in August and September 2023 using the same pre-season measurement protocol as published by Arnason et al.13 In addition to goalkeepers, players who were unable to fully participate in training due to injuries during the pre-season data collection period were excluded. No other exclusion criteria were used. Participants were included irrespective of their previous history of shoulder problems. A flow chart of the recruitment process and data collection is presented in Figure 1. The follow-up period lasted through a whole regular season of 29 weeks (from September 2023 to April 2024). All participants provided written informed consent prior to participation, and the study was approved by the National Bioethics Committee (VSN-22-084-V2). Each pre-season test was conducted by the same tester for all participants.

Isometric Mid-thigh Pull
The isometric mid-thigh pull (IMTP) was used to measure LBS, following the protocol outlined by Comfort et al.16 The test has been shown to correlate highly with one repetition max in both deadlift and squat and is therefore considered an appropriate test to measure peak LBS in the laboratory setting.17,18 Participants completed a standardized warm-up protocol, including a series of body weight squats and lunges, followed by three familiarization trials performed at approximately 50%, 75%, and 90% of perceived maximal effort. During the testing phase, knee and hip joint angles were standardized to 125–145° and 140–145°, respectively, in accordance with the recommendations by Comfort et al16 (Figure 2). While testing, participants held a 20 kg weightlifting bar in a fixed position while standing on a force plate sampling at 100 Hz (AMTI, Watertown, Massachusetts, USA). To minimize the effect of different grip strength, all participants’ hands were strapped to the bar with weightlifting straps. Participants got verbal encouragement during each trial and were encouraged to push as hard and as fast as possible down into the force plate, which measured the vertical component of the ground reaction force. Three trials were performed, all of which included participants’ body weight. The trial with the highest absolute peak force value (PF) was used for data analysis.

Trunk Rotation Power
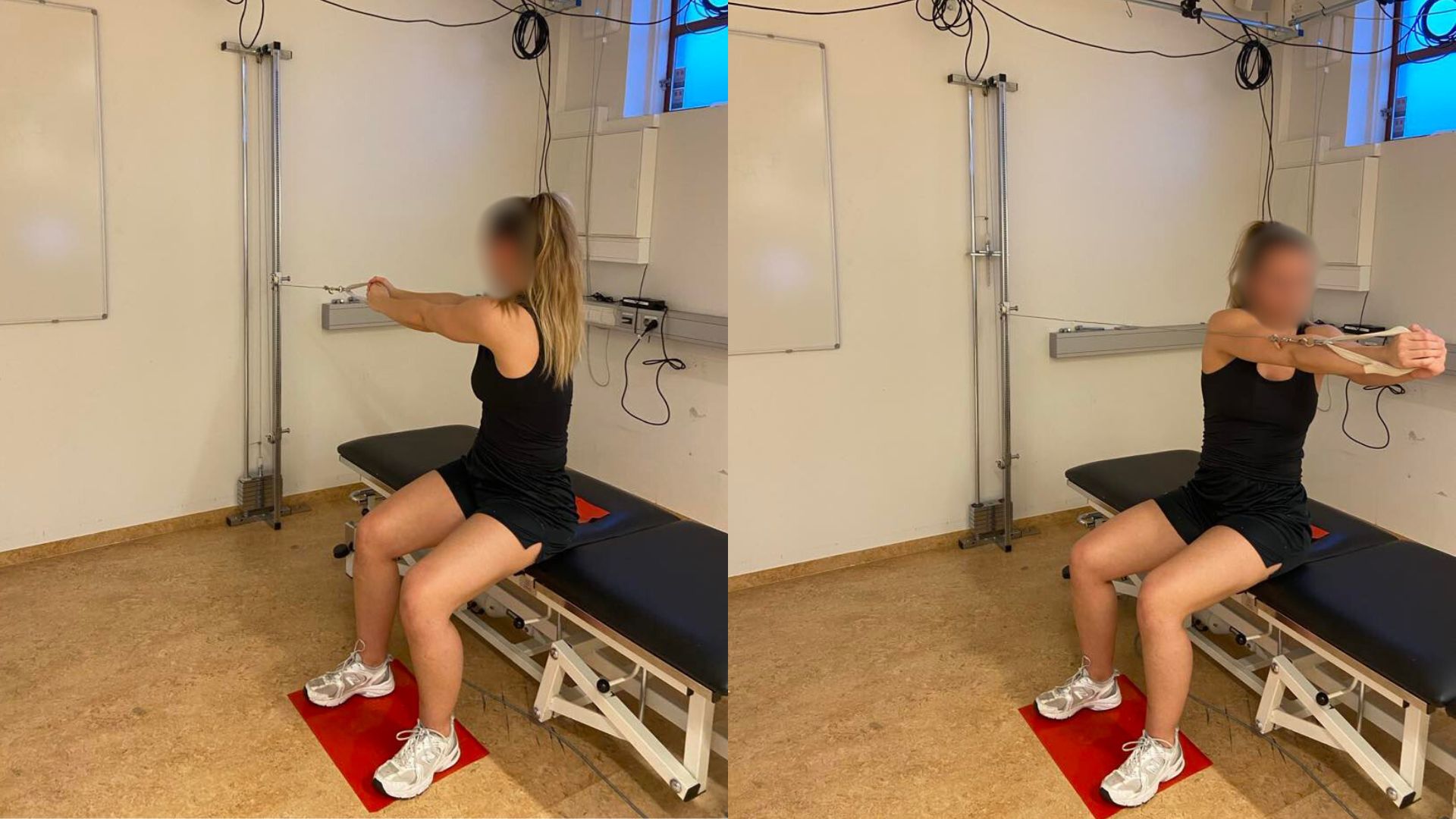
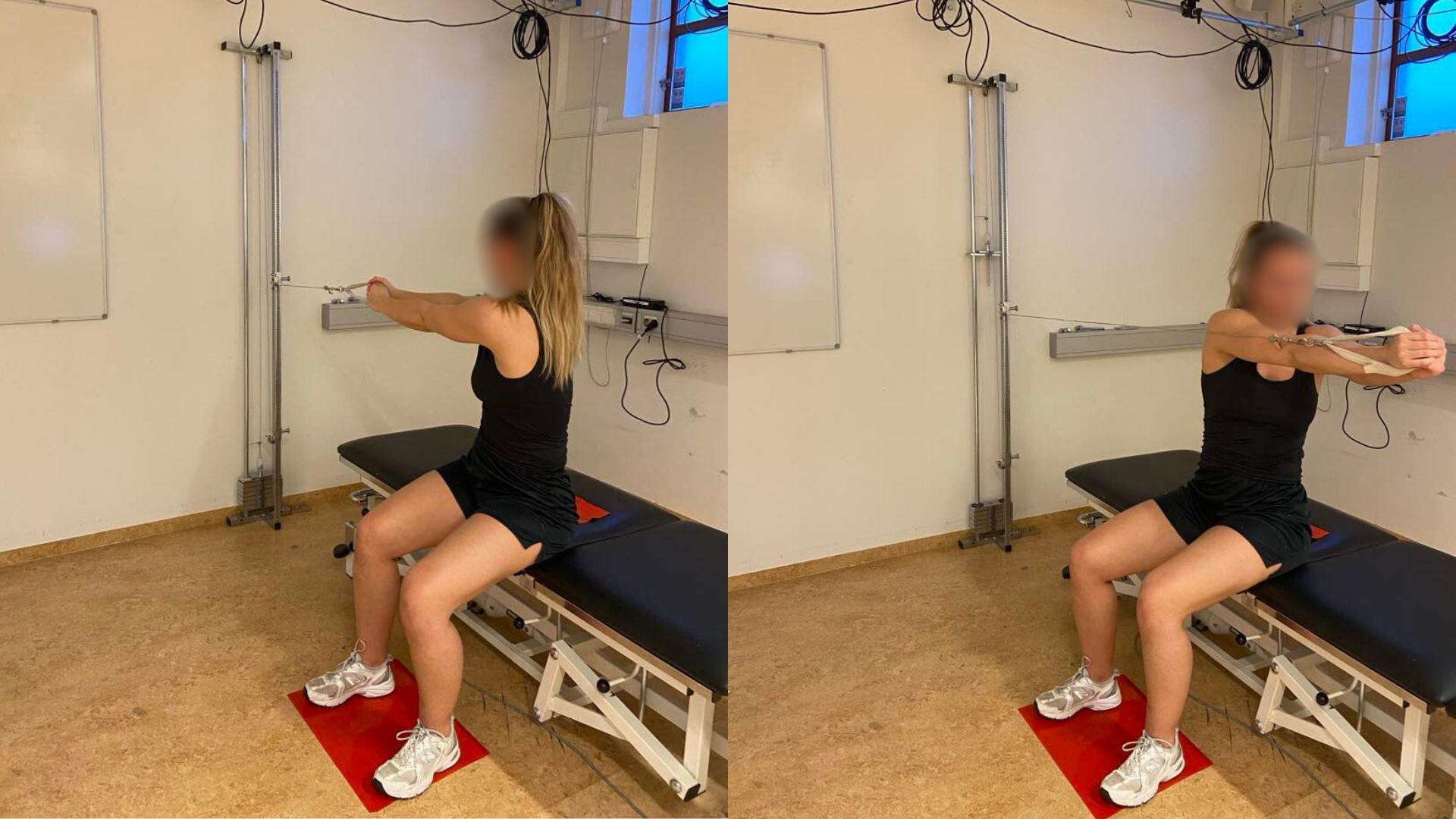
TRP was measured with a pulley machine using a testing protocol previously used to measure TRP in handball players and which has been shown to be reliable.13 Participants were seated on a treatment plinth, with hips and knees at 90° of flexion and a non-slip mat was placed under their feet and buttocks to prevent sliding (Figure 3). Participants held the pulley with both arms straight at 90° shoulder flexion and were instructed, on cue, to rotate through 180° as quickly as possible, using a weight equivalent to 5% of their body weight. A standardized warm-up routine, including two sets of 10 repetition of seated trunk rotation with 2.5% of body weight followed by two familiarization trials at 75% and 90% of perceived maximal effort, were completed prior to the measurements. Only left side rotation was measured for right-handed players and right side rotation for left-handed players. Inertial sensors (Movella dot, Henderson, Nevada, USA) were placed on the top of the weights in the pulley machine to measure acceleration. Raw data were collected through the Movella dot app (Movella dot, Henderson, Nevada, USA) and exported into Microsoft Excel for further analysis.
Acceleration data were used to calculate power output with the formula: (W=(a+g)*t*F), where W is power in watts, a is the measured acceleration (m/s²), g is the gravitational constant (9.81 m/s²), t is the time (in seconds) over which the force is applied, and F is the applied force in newtons, corresponding to the pulley load. Three trials were performed and the trial with the highest absolute power value was used for data analysis.
Shoulder Strength
The isometric strength of the internal and external rotators of the dominant shoulder was measured using an externally fixed handheld dynamometer (HHD) (Lafayette Instruments, Lafayette, Indiana, USA) in a supine position (Figure 4).2,3,19 The shoulder was positioned in 90° of abduction and 0° rotation, with the elbow at 90° flexion and the non-testing arm resting on the stomach. A towel was placed under the distal end of humerus to keep the upper arm in the horizontal plane. Participants finished a standardized warm-up protocol,19 followed by one familiarization trial at 50% of perceived maximal effort. The participants were instructed, on cue, to press as hard as possible into the HHD and maintain the pressure for three seconds. Three trials were performed and the average value from the three trials was used for data analysis.13 The pre-season ER/IR strength ratio was calculated by dividing the ER strength by the IR strength.

Self – reported Shoulder Problems and Internal Load Documentation
The Oslo Sports Trauma Research Center Overuse Injury Questionnaire (OSTRC-O2), previously used in handball related research,2,3,6,19–21 was used to collect self-reported data through REDCap electronic data capture tools hosted at University of Iceland. The OSTRC-O2 was emailed to all participants once a week throughout the regular season, covering a duration of 29 weeks. An automatic reminder was sent to non-responders after two and four days.
The questionnaire included four questions that asked whether shoulder problems (defined as any pain, ache, stiffness, clicking/catching, swelling, instability/giving way, locking, or other complaints) had affected participation, training/competition, or performance, and whether participants had experienced any pain in the dominant shoulder related to handball over the prior seven days. Each question had four response options, scored on the scale 0-8-17-25, with 0 representing no problem and 25 maximum severity. To calculate a weekly severity score, the scores from these four questions were summed, resulting in a total score ranging from 0 to 100, where 0 represents no problem and 100 the maximum severity. The average OSTRC-O2 severity score for each participant was calculated by dividing the total score from all completed questionnaires by the number of times the questionnaire was answered.2 The group weekly prevalence of shoulder problems was calculated by dividing the total number of participants reporting any problem (anything but the minimum value in any of the four questions) by the total number of questionnaire respondents that week. The individual weekly prevalence of shoulder problems (anything but the minimum value in any of the four questions) was calculated by dividing the total number of times each participant reported a problem by the total number of that participant´s questionnaire responses. The group and individual weekly prevalence of substantial problems was calculated in the same manner, specifically for shoulder problems that caused moderate or severe reduction in training/competition or performance or total inability to participate.
An additional question about the weekly PSL (internal load) was added to the questionnaire by the authors. Participants were asked to rate the weekly PSL on a modified Borg rate of perceived exertion scale (RPE - from 0-10 with specific description for each score, where 0 = no exertion, 10 = maximum exertion), by answering the question “How hard was the recent week on your throwing arm?”. The modified Borg RPE was recommended by the 2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels14 as an appropriate way to measure PSL in a sport like handball. The average PSL of each participant was calculated by dividing the total score from all the questionnaires answered during the study period by the number of times the questionnaire was answered.
External Load
To provide a more objective measure of shoulder load, data on the total number of shots taken by each participant, during all divisions matches across the season, were collected. These data were obtained from HBStatz (www.hbstatz.com), an Icelandic handball analytics platform that serves as the official statistics provider for the Icelandic Handball Association. HBStatz collects detailed, real-time match data from the top men’s and women’s divisions, using trained observers and strict quality control procedures. In this study, the total number of shots per player was used as the operational definition of external load.
Outcome measures and statistical analysis.
The outcome measures were: 1) The association between each of the pre-season measurements (LBS, TRP and shoulder strength) with OSTRC-02 results (individual prevalence, individual substantial prevalence, and severity score); 2) The influence of each pre-season measurement on the association between PSL and the OSTRC-O2 severity score; 3) The influence of each pre-season measurement on the association between external load (number of shots) and the OSTRC-O2 severity score.
An a-priori power analysis, used in other research with a similar research question and setting by the authors of this study, indicated that a sample size of minimum 46 participants was needed to achieve 80% power for a correlation value of 0.4 for the association between the pre-season measurements and the OSTRC-O2 results.13 Microsoft Excel and Jamovi statistical software were used for data analysis. The Shapiro-Wilk test was applied to assess the normality of the data. Spearman’s rank correlation coefficient was used to evaluate the associations between pre-season measurements and a) OSTRC-O2 results and b) external load. Correlation strength was interpreted as follows: 0–0.1 = negligible, 0.2–0.39 = weak, 0.4–0.69 = moderate, 0.7–0.89 = strong, and 0.9–1 = very strong.22 A mixed model ANOVA was used to assess the influence of shoulder load and each pre-season strength and power measurement on the severity of shoulder problems (main effects), and the interaction of those variables. Partial eta squared was calculated using the formula η2p=t2/(t2+dft) to demonstrate the effect size of the mixed model ANOVA interactions (t² = The square of the t-statistic from the ANOVA interaction term (Jamovi); dft = The degrees of freedom associated with the t-test). The significance level was set at p < 0.05.
RESULTS
Participants
Thirty-three female outfield players (age 18-35, Table 1) participated in this study. Two participants stopped answering the OSTRC-02 early in the follow-up period and did not respond to repeated contacts, leaving results from 31 players for data analysis. Six participants reported dealing with shoulder problems in the throwing shoulder during the previous season, but no participant reported acute shoulder injury during the follow-up period or any major lower limb injuries.
Self-reported Shoulder Problems, Internal (PSL) and External load (number of shots)
The average response rate for the OSTRC-02 throughout the season was 88%, with 18 players having a response rate above 95% (range: 31-100%). The average group weekly prevalence of shoulder problems was 20% (95% CI 17-22.5, range 4-32%), and 3.4% (95% CI 2.2-4.6, range: 0-11%) for substantial shoulder problems. Twenty-four out of 31 players (77%) reported a shoulder problem at some point during the season. Despite this, the average severity score was low, with a mean OSTRC-O2 severity score of 7.7 out of 100 (95% CI 3.8-11.7, range: 0-40.2), and 19 players (61%) registered a score below 5. For internal load, the average PSL throughout the season was 3.9 out of 10 (95% CI 3.4-4.4, range: 1.1-6.4). For external load, the average number of shots taken during all division matches across the season was 71 shots per player (95% CI 47-95, range: 0-245).
Pre-season Strength and Power and their Association with the OSTRC-O2 Results and the External Load
Table 2 summarizes the average absolute max values for the pre-season ER, IR and LBS strength tests, TRP, and the average pre-season ER/IR ratio.
A moderate and positive correlation was observed between pre-season LBS and the individual prevalence of substantial shoulder problems (rs = 0.40, p = 0.03). A weak and positive correlation was observed between pre-season ER and IR strength and the individual average OSTRC-02 severity score (rs = 0.37, p = 0.04 for both), as well as between ER strength and the individual prevalence of substantial shoulder problems (rs = 0.38, p = 0.04). A moderate to strong positive correlation was found between all pre-season measurements and the external load, indicating that stronger players threw more shots during all division matches across the season (ER rs = 0.61; IR rs = 0.50; LBS rs = 0.73; TRP rs = 0.54, p > 0.001 for all).
Association Between Internal Load and the OSTRC-O2 Severity Score, and the Influence of Pre-season Strength and Power
For all mixed model ANOVAs, an association was identified between the PSL and the OSTRC-O2 severity score (main effect, p < 0.001), indicating that a higher PSL was associated with a higher OSTRC-O2 severity score. However, a significant interaction was observed as pre-season TRP, LBS, and ER strength influenced this association (r2 = 0.57, p = 0.001, η2p = 0.014; r2 =0.59, p = < 0.001, η2p = 0.02; r2=0.57 p = 0.01, η2p = 0.008 respectively). Players with pre-season TRP, LBS, and ER strength more than one standard deviation (SD) above the group’s mean exhibited stronger association between PSL and the severity score, whereas weaker association was observed for players with pre-season TRP, LBS and ER strength values one SD below the group´s mean (Figure 5). The interaction between pre-season IR strength and PSL with respect to the OSTRC-02 severity score did not reach statistical significance (p=0.1).

Association Between External Load and the OSTRC-O2 Severity Score, and the Influence of Pre-season Strength and Power
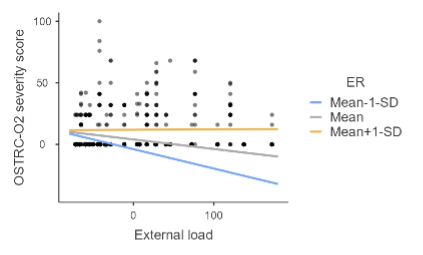
A significant negative association was found between the external load and the OSTRC-O2 severity score, (main effect, p=0.04), indicating that increased number of shots was associated with decreased severity score. However, a main effect was only found when the mixed model ANOVA included pre-season ER strength as a covariate. Further, a significant interaction was found (r2=0.52, p=0.04, η2p = 0.15) showing that the association between OSTRC-02 severity score and external load was only apparent for players with ER strength one SD below the group´s mean (Figure 6). No other interactions were observed for the influence of pre-season measurements on the association between the external load and the OSTRC-O2 severity score.
_and_pre-season_er_strength_reg.png)
DISCUSSION
The main findings of this study indicate that players with high pre-season TRP, ER and LBS reported more severe shoulder problems as PSL increased throughout the season. The association between PSL and shoulder problems was greater in those players with high pre-season strength and power. These findings were unexpected and contradict the proposed hypotheses.
The results also indicated that PSL was more consistently associated with severity of shoulder problems than external load. However, the measures of internal vs external load seem to reflect different things and should both be considered from a clinical perspective. To the authors´ knowledge, this is the first prospective study to link high pre-season strength and power to increased shoulder problems in female handball players and the first to suggest that internal load measurements, such as PSL, might be more relevant for monitoring shoulder load that can influence the development of shoulder problems among handball players during a season. External load (number of shots) may only partially represent load as defensive load during matches is ignored and the measure can also be influenced by shoulder problems, which may lead to fewer shots being taken. Importantly, the influence of internal and external load measures was mediated by pre-season strength and power
Self-reported Shoulder Problems, Internal (PSL) and External load (number of shots)
The average weekly prevalence of shoulder problems and of substantial shoulder problems in this study was somewhat lower than those shown in recent studies.2,4 In a large study involving elite female handball players, shoulder problems and substantial problems were 26% and 9% respectively.2 Similarly, a study involving male and female adolescent players found prevalence of 25% and 6%, respectively.4 However, the cohorts in those studies were much larger than in this present study, limiting direct comparison. The seasonal prevalence of shoulder problems in this study (77%) was notably higher than 48% reported by Asker et al.4 This discrepancy may be partly due to different demographics, in particular athletes of younger ages in that study.
Due to the limited number of studies addressing PSL in female handball players, direct comparison for this metric is unavailable. Nevertheless, the average PSL of 3.9 characterized as “somewhat hard” on the Borg scale23 aligns with results reported for elite male handball players.13 For this study, external load was measured as the total number of shots taken during division matches across the season, providing an objective albeit limited perspective on shoulder stress. The optimal method for measuring shoulder load in overhead athletes has been debated, as differences between sports, playing position and load types complicate standardization.14 The results of this study show that a self-reported measure of internal load, such as the PSL, may be more important than external load as it represents all shoulder load during offense and defense in training and competition. It may therefore capture cumulative shoulder load in handball better than the external load, in the form of number of shots, that reflects a limited aspect of competition alone and can be influenced by shoulder problems (e.g. players taking fewer shots) and/or their role during matches (e.g. predominantly defensive playing time).
The results from the mixed model ANOVA including the external load and ER strength as covariates, showing that increased number of shots were associated with decreased severity score, were interesting and surprising. The interaction showed that lower ER strength was a driving factor in that association. One possibility is that low pre-season ER strength might lead to decreased ball velocity while throwing, with less deceleration and eccentric load on the posterior rotator cuff.
The overall low severity score and limited variability of the raw data also introduces the possibility of a floor effect, which may have led to an underestimation of the true strength of associations between pre-season strength and power and shoulder problems in this cohort through the effect of attenuation bias. The clinical meaning must therefore be considered with caution despite statistical significance.
Pre-season Strength and Power and their Association with the OSTRC-O2 Results, and Internal Load
The observed pre-season ER/IR ratio and absolute ER and IR shoulder strength in this study are consistent with previously reported reference values for female handball players.24 However, contrary to expectations ER strength was positively correlated with the individual prevalence of substantial shoulder problems and OSTRC-O2 severity score. These findings challenge prior research suggesting that ER strength serves as a protective factor against shoulder problems in both male and female handball players.3,6,25,26 Similarly, the positive correlation between the pre-season IR strength and the severity score contradicts studies identifying reduced IR strength as a risk factor for shoulder problem in female adolescent handball players.6 The observation that players with high pre-season LBS, ER strength and TRP reported more severe shoulder problems as the PSL increased throughout the season contradicts previous findings from male handball, where players with low pre-season TRP reported more severe shoulder problems.13 It also calls into question the assumption that greater LBS may protect the shoulder by reducing shoulder load during throwing motion by effectively transferring forces up through the kinetic chain.9,27,28 This suggests the likely importance of additional factors when considering shoulder problems, such as playing and training time and physical or biomechanical differences, which may predispose stronger individuals to more shoulder problems.
Increased physical fitness has been associated with improved performance index rating in female elite basketball players29 and greater playing time30 in youth football. Therefore, stronger players in this study may have seen more playing time, increasing both offensive throwing load and defensive tackling/collision load, which may have contributed to reports of shoulder problems. In general, more physically robust handball players are positioned in the middle of the defensive line where the collision load is the highest. This speculation is supported by the observed association between the PSL and the severity score and the positive correlation between pre-season strength and power and the external load. Possibly, female handball teams include fewer players of sufficient physical fitness to play at elite level compared to male teams. Therefore, the stronger and fitter players might be exposed to more loads as they are more likely to be both defensive and offensive players. Implementation of adequate strength training early in the career of female handball players is therefore considered to be vital. To be able to distribute playing time, female handball teams need to have a large number of players with sufficient physical fitness.
Throwing technique and sex-specific kinematics may also play a role in explaining sex-dependent differences in the prevalence of shoulder problems and influence of strength and power in handball. Female players have been shown to demonstrate a higher ER angle during the cocking phase and slower trunk rotation angular velocity compared to males.31 Greater ER has, in turn, been linked to improper trunk rotation sequence and greater shoulder load in baseball pitchers.10 Less explosive trunk rotation in the acceleration phase31 might lead to more load being placed on the shoulder in order to achieve optimal ball velocity as trunk rotation angular velocity has been shown to strongly and positively correlate with ball speed.32 In terms of trunk contribution to throwing, reaching max trunk rotation angular velocity closer to ball release is thought to have a protective effect on the shoulder by reducing the load on the shoulder joint.33 Female handball players have been shown to demonstrate a different movement pattern than males during throwing where they reach max trunk flexion and pelvis tilting angular velocity earlier, relative to ball release, compared to males,31 which may disrupt the proximal to distal transfer of energy.
Limitations and Methodological Considerations
The main limitation of this study is the small sample size, which restricts generalizability to larger populations and limits statistical power. The statistically significant results must therefore be interpreted with caution. The sample size goal from the power analysis calculation was not reached due to unavailability of a few teams in the top division, some of which were based in another part of the country. Additionally, pre-season testing was scheduled based on player availability, introducing potential variability in fatigue levels at the time of assessment. The OSTRC-O2 relies on participants’ subjective recall of shoulder problems for the prior seven days, which introduces the possibility of recall bias. The same applies with the question regarding players’ estimate of the PSL during the previous week. Using the total number of shots per player in division matches as a definition of external load is limited, as it does not account for long passes during matches and training, or the number of shots during training. However, accurately documenting the number of passes and shots per player during training is impractical. The strength of this study is the overall high response rate to the OSTRC-O2 questionnaire, coupled with the extended follow up period, which provides precise information about the prevalence and severity of shoulder problems. However, as handball exposure in terms of minutes was not documented, true handball exposure during the season for each participant remains unknown. At this elite level players would be expected to engage in a similar amount of training during the season. However, some players might have had limited playing time during matches across the season, which could have affected their OSTRC-O2 results, PSL and external load and thereby influenced the association between the pre-season variables, the PSL, external load and the OSTRC-O2 results.
CONCLUSION
The results of this study highlight the complexity of the association between pre-season strength and power and shoulder problems in female handball players, and the influence of additional factors, such as match and training exposure, and female-specific throwing kinematics, which require further investigation. Furthermore, this is the first study to demonstrate that internal load measurements, such as PSL were more consistently associated with the physical load placed on the shoulder in a chaotic sport like handball, compared to external load, via registered number of shots during matches.
Conflicts of interest
The authors declare no conflicts of interest.
Acknowledgement
Dr. Þórarinn Sveinsson for his assistance during the statistical analysis, Dr. Hilde Fredriksen and Dr. Elís Þór Rafnsson for their guidance during the writing of this manuscript and HBStatz for providing performance-related data.