INTRODUCTION
Running is one of the most popular physical activities worldwide.1 Within running, trail running has emerged as a rapidly growing discipline,2–4 presenting unique challenges due to its varied terrains and inclines.5 Navigating these inclines requires grade-specific adaptations.6 Compared to level running, downhill running is characterized by increased aerial time, reduced step frequency and decreased duty factor6 - the proportion of the stride cycle during which the foot is in contact with the ground. Higher impact force in downhill running likely causes greater accelerations of all body tissues, requiring higher energy dissipation by muscles as well as the heel pad, bones, and spinal discs.7–10 These high impact forces have been associated with overuse injuries6 and contribute to a higher proportion of eccentric-biased muscle actions of the lower limb in downhill running.11
Uphill running is characterized by higher step frequency, increased internal mechanical work, shorter swing phase duration, a greater proportion of the stride cycle spent in stance and elevated duty factor.6 Increased internal mechanical work leads to a higher muscle activity of lower limb muscles12 and higher metabolic energy costs resulting in elevated heart rates (HR).13
The lower limbs are not the only area of concern; the runner’s back is also subjected to high forces during running.14 Nevertheless, it has received limited research attention,15 despite the prevalence of low back pain reaching up to 20.2% among runners.16 Levine et al.15 conducted the only study to date that specifically examined the effects of different gradients on lumbar spine posture during running. They reported that, compared to level running, lumbar lordosis increased during downhill running and decreased during uphill running. Standing with increased lumbar lordosis was shown to be related to a higher risk for developing or maintaining low back pain.17 In a simulation study, excessive lumbar lordosis was shown to result in greater torque and increased anteroposterior shear forces compared to normal lordosis, while compressive intervertebral forces at each lumbar joint remained unchanged.18 This highlights the importance of trunk function, as it plays a key role in maintaining proximal control during running, with inadequate motor control being linked to dynamic instability and higher injury rates.19 Key muscles include the abdominals, erector spinae and posterior hip muscles.20 The abdominals provide stability by counteracting buckling and distributing impact forces.19,20 The erector spinae primarily act as stabilizers, limiting trunk rotation as the body decelerates at foot strike.21,22 The hip muscles, including the gluteus maximus and hamstrings, support the abdominals by counteracting gravity, maintaining trunk and spinal stability, and preventing tilting and buckling.20 Additionally, a stable trunk serves as the center of the kinetic chain, enabling powerful and precise movements of the extremities.23,24 Understanding the kinetic changes in the lumbar spine and its neighboring joints could help in developing injury prevention strategies and return-to-activity protocols.
The main aim of this study was to examine how running on six different gradients (ranging from -15% downhill to +15% uphill) affects back and pelvic posture, as well as muscle activity in trunk and lower limb muscles. The hypotheses were that (1) lumbar lordosis would increase during downhill and decrease during uphill running, (2) hip drop would increase during downhill and decrease during uphill running, (3) pelvic tilt in the sagittal plane would increase in both downhill and uphill running, and (4) trunk inclination would adjust, shifting towards a backward-leaning position in downhill and a forward-leaning position in uphill running.
MATERIALS AND METHODS
Study Design
The study was conducted as a descriptive laboratory study on two different days. The first day served as a familiarization day, followed by a testing day. The interval between the familiarization and testing day was no more than two weeks. The study protocol complied with the latest version of the Declaration of Helsinki and was evaluated and approved by the regional ethics committee (Basel, Switzerland; EKNZ 2023-02146).
Subjects
This study recruited recreational runners via convenience sampling from May 2024 to September 2024. Twelve healthy recreational runners (6 women and 6 men) gave their written voluntarily informed consent to participate in the study. To be included, participants had to be between 18 and 30 years of age, engaged in at least 4.5 hours of running-related training per week, and had a personal best of under one hour for 10 km. Persons with a history of lower extremity or trunk injuries within the prior six months, or any other physical conditions that would impair full, pain-free performance, were excluded from the study. Participants were asked to avoid maximal physical exertion 48 hours prior to testing.
Procedures
During the familiarization phase, the participants completed an individual warm-up routine that they would typically perform before a running competition. Subsequently, all testing procedures were explained and performed. This session lasted approximately 90 minutes. On the testing day, subjects performed the same treadmill running protocol including different slopes and maximum voluntary isometric contractions (MVIC) testing as during familiarization. During the treadmill running protocol, muscular activity of the lower limb and the trunk muscles as well as the lumbar lordosis, hip drop, pelvic tilt, trunk inclination, heart rate (HR) and ratings of perceived exertion (RPE) were assessed. In total, the testing session lasted about two hours.
Instrumentation
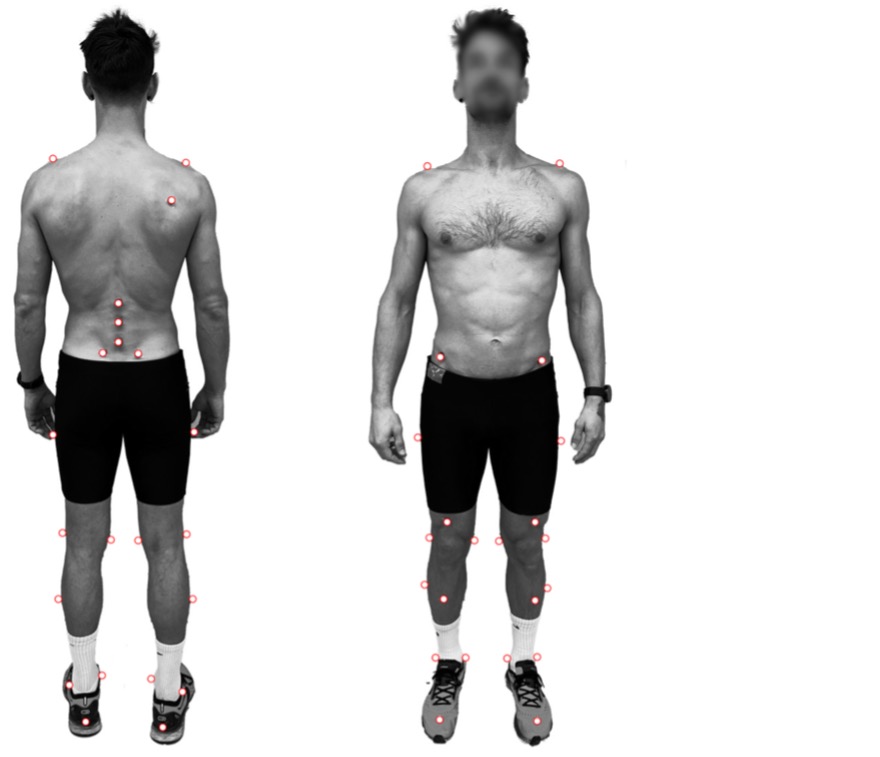
At the beginning of the testing session, surface electromyography (sEMG) sensors (Wave Plus, Cometa srl, Milan, Italy) were applied to nine muscles on the subject’s right side: medial gastrocnemius, semitendinosus, biceps femoris, gluteus maximus, gluteus medius, vastus lateralis, rectus abdominis, external oblique and erector spinae. Bipolar electrode configurations were used (2-3 cm electrode separation) with a sampling rate of 1 kHz. The sensor application followed SENIAM guidelines and was aligned with the expected fiber orientation. Prior to electrode placement, the skin was shaved, abraded with an abrasive gel (Nuprep, Weaver and Company, USA), and wiped with alcohol to ensure electrode resistance was below 10 kΩ. Electrode placement was confirmed through manual muscle testing and visual inspection of the raw signals. Additionally, 33 three-dimensional motion capture system (Vicon Motion Systems Ltd, United Kingdom) reflective markers were bilaterally placed on anatomical landmarks (Figure 1). Reliability of the kinematic system has been established for measurement of both pelvic tilt and lumbar spine position.25,26 The marker placement was based on Vicon Plug-In Gait Lower Body AI27 and was modified by additional markers. The exact placement of the important markers for data analysis was marked directly on the subject’s skin to ensure accurate repositioning in case of falling. Data were captured using 17 cameras (Vicon Motion Systems Ltd, United Kingdom) with a recording frequency of 100 Hz.
Treadmill
After calibration of the motion capture model, a running protocol was performed on a treadmill (Pulsar, H/P Cosmos, Germany). Participants performed three-minute runs at each gradient, starting at level (0%), followed by three uphill (+5%, +10%, and +15%) and three downhill (-5%, -10%, and -15%) gradients. The running speed was calculated for every subject individually based on their personal best on 10 km. During level running, participants ran at 90% of their personal best speed. For downhill running the speed was increased by a consistent factor of 0.034 m/s for each 1% gradient decline.28 For uphill running, the speed was adjusted to maintain equivalent performance kilometers per hour (speed of level running in km/h / (1 + gradient in percent * 0.07)). RPE was subjectively reported by participants using the 6–20 point Borg scale following two minutes of each condition. HR was recorded with the Acentas Team System (Acentas, Hörgertshausen, Germany), with values being extracted around the two-minute mark of each condition. For 3D motion capture, 30-second recordings were initiated during the final minute of each condition. Ground reaction forces were obtained by a Kistler® force platform (Kistler, Type 9286BA, Winterthur, Switzerland) at 1000 Hz sampling rate.
MVIC testing
After the running protocol, MVIC testing was performed following a minimum rest period of 10 minutes to allow for partial recovery. Muscle activity was monitored via sEMG during all MVIC assessments. The testing included isometric trunk flexion and extension, as well as hip extension and abduction, using an isokinetic dynamometer (IsoMed 2000; D&R Ferstl, Hemau, Germany). MVIC testing of the knee extensor and flexor muscles was performed in a seated position with 50° knee flexion. Additionally, isometric plantar flexion was evaluated with participants in a standing position. To ensure the contractions remained isometric, a fixed, immovable bar was positioned above their shoulders. Each MVIC test position was held for a minimum of 5 seconds and repeated three times. The highest peak force across trials was used to determine the MVIC.
Statistical Analysis
For statistical analysis, all downhill gradients (-5%, -10%, and -15%) and uphill gradients (+5%, +10%, and +15%) were separately compared to level running (0%). All subsequent lower limb parameters were calculated for the right side only.
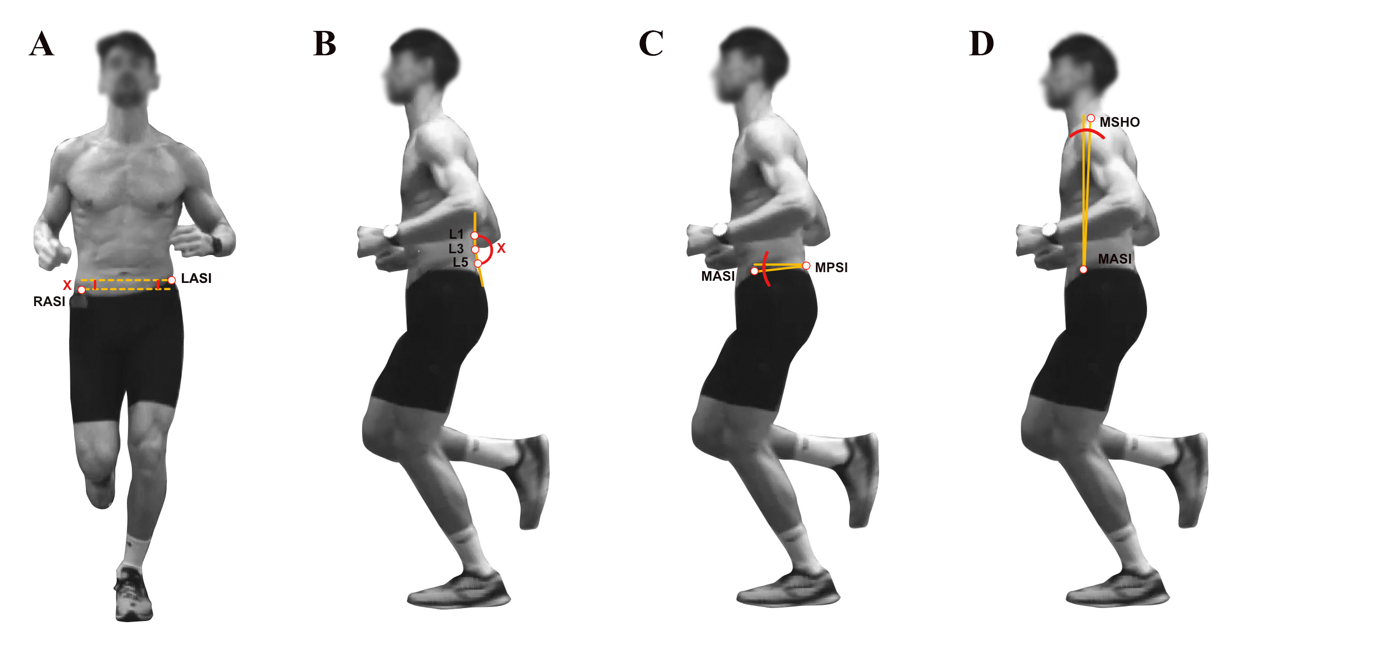
Raw trajectory data from the 3D motion capture were processed using inbuilt software (Vicon Nexus 2.16, Vicon Motion Systems Ltd, United Kingdom). To account for slope-related changes in foot strike patterns,6 stance phase was defined as the interval from initial contact of any part of the foot to full foot-off, based on force plate data. Step length was calculated by multiplying the sum of contact time and aerial time (in ms) by the running speed (in m/s). Contact time and aerial time were defined according to the definitions provided by Hollander et al.29 Maximum horizontal hip drop was defined as the greatest vertical displacement (in mm) between the right (R) and left (L) anterior superior iliac spine (ASI) during the stance phase (Figure 2A). Additionally, total hip drop was calculated as the vertical displacement (in mm) between the RASI and LASI from foot strike to maximum hip drop during the stance phase. Lumbar lordosis, pelvic tilt, and trunk inclination were calculated at the frame of maximal hip drop. Lumbar lordosis was determined in degrees as the angle between the L1, L3, and L5 markers (Figure 2B). Pelvic tilt was calculated as the vertical displacement (in degrees) between the midpoint of the right and left posterior inferior iliac spine markers (midPSI) and the midpoint of the right and left ASI markers (midASI) (Figure 2C). Trunk inclination was defined in the sagittal plane as the horizontal displacement (in degrees) of the midpoint between right and left shoulder markers (midSHO), relative to the the right and left midASI markers (Figure 2D). Shifts toward a forward-leaning position are represented as positive angles, while shifts toward a backward-leaning position are represented as negative angles.
_lumbar_lordosis_(b)_pelvic_tilt_(c)__t.png)
EMG data were filtered using a Butterworth bandpass filter (10-400 Hz) and a notch filter (50 Hz). Average activation during the stance phase was extracted for each step and muscle during the 30-second recordings of each condition. Muscle activity recorded during running was normalized (%MVIC) to the maximum activation magnitude observed during corresponding MVIC testing exercises. All calculations were performed using MATLAB (R2024b, The MathWorks, Inc., Natick, MA, USA).
For statistical analysis, a random effects linear mixed model (GAMLj, Jamovi) was used to investigate differences in the measured physiological, neuromuscular, and biomechanical parameters. Random intercept per participant model was used to account for repeated measures. Values are reported with mean and standard deviation. Level of significance was set at p < 0.05. Additionally, Cohen’s d was computed and interpreted as trivial (< 0.2), small (0.2–0.49), moderate (0.5–0.79), large (0.8–1.19) and very large (> 1.2). Normal distribution of residuals was verified visually through inspection of Q-Q-Plots. Values exceeding two standard deviations from the mean for each condition and parameter were identified as outliers and excluded from the statistical analysis.
RESULTS
Participants included six women (age: 25.0 ± 1.6 years; body mass: 61.1 ± 3.5 kg; height: 167.8 ± 5.4 cm) and six men (age: 26.3 ± 1.2 years; body mass: 75.0 ± 6.9 kg; height: 178.0 ± 8.5 cm). The results are categorized into three key areas: postural and biomechanical adaptations, muscle activity, and physiological demands. Within each category and parameter, results for downhill running are presented first, followed by the results for uphill running. The discussion will follow the same structure.
Postural and Biomechanical Adaptations
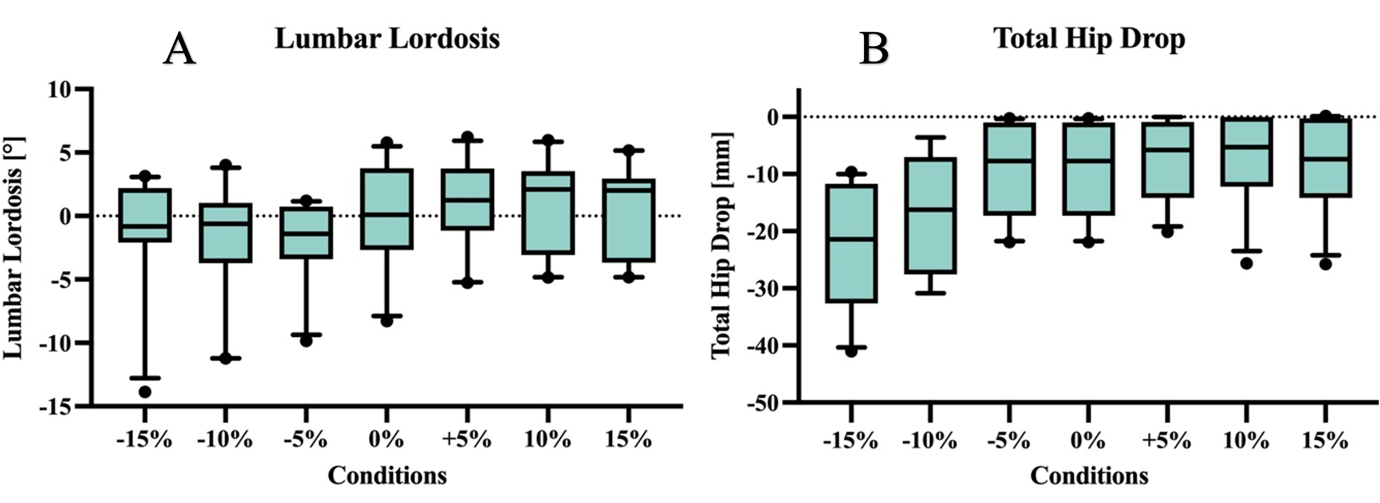
Table 1 shows the mean values and standard deviations for lumbar lordosis, hip drop, pelvic tilt, and trunk inclination. Statistical analyses, including Cohen’s d effect sizes and confidence intervals, are summarized in Table 2. Horizontal hip drop decreased across all slopes compared to level running. Total hip drop in contrast progressively increased with steeper negative gradients, while showing a slight decrease at uphill gradients. Pelvic tilt increased during downhill gradients and decreased at +5% and +10%. No change was observed at +15%. Trunk inclination shifted backward on downhill and forward on uphill gradients, with progressively larger effects as gradients increased.
_and_total_hip_drop_(b)_across_conditions._the_median_is_sh.png)
Muscle Activity
Muscle activation patterns during the stance phase varied across gradients, as summarized in Tables 3 and 4. Table 3 provides mean values and standard deviations, while Table 4 details the differences relative to level running in standardized effect sizes with confidence intervals. For the lower limb muscles, the gastrocnemius exhibited increased activity during downhill running at a -15% gradient, while the vastus lateralis showed heightened activity at -5%, -10%, and -15%. The gluteus maximus, gluteus medius, and biceps femoris showed numerically increased activation during downhill gradients, although no statistically detectable difference was found. During uphill running, the gastrocnemius, biceps femoris, and vastus lateralis all demonstrated higher activity across all uphill gradients. In contrast, the gluteus maximus showed increased activity only at +10%, while the gluteus medius showed increased activity only at +15%. No significant changes were observed in the other lower limb muscles. Among the abdominal muscles, only the obliquus externus showed numerically higher activity across gradients compared to level running, with a significant difference observed only at -10%.. The erector spinae was the only muscle to exhibit reduced activity, with decreases observed at -10%, -5%, +10% and +15% but not at -15% and +5%.
Physiological Demands
The mean values for HR, RPE, contact time, aerial time, and step length across all conditions are summarized in Table 5. Cohen’s d effect sizes and their confidence intervals are provided in Table 6.
HR was lower at -15% and -10%, and higher at +10% and +15%. Compared to level running, no effect was observed at -5% and +5%. RPE increased for downhill gradients (-15% to -5%) and rose during uphill gradients. Contact time increased progressively from the steepest downhill gradient (−15%), where it was shortest, to the steepest uphill gradient (+15%), where it was longest. Aerial time was higher across downhill gradients and lower across uphill gradients. Step length increased sharply with steeper downhill gradients and strongly decreased with increasing uphill gradients.
DISCUSSION
Running, particularly trail running, often involves both downhill and uphill segments. This study examined the physiological adaptations, muscle activity changes, and biomechanical alterations in the back and pelvis during varying gradients. The main findings were that compared to Level, lumbar lordosis increased across all downhill gradients and decreased during uphill gradients of +5% and +10%. Additionally, while horizontal hip drop was lower for both downhill and uphill gradients, total hip drop was higher during steep downhill running.
Postural and Biomechanical Adaptations
The lower horizontal but markedly greater total hip drop in downhill running suggests that runners approached foot strike with a higher hip position than during level running, potentially as a preventive strategy to anticipate the elevated ground reaction forces.8 However, no increase in gluteus medius activity was observed, despite its potential role in force dissipation. Similarly, Forch et al.30 reported only weak associations between hip drop, hip abductor strength, and hip abductor muscle activity during level running. The observed increased lumbar lordosis during downhill running aligns with the results of Levine et al.15 This increase may be related to the greater pelvic tilt angle and the smaller trunk inclination angle as a runner shifts towards a backward-leaning position.
The reduced horizontal and total hip drop across uphill gradients may be attributed to lower vertical ground reaction forces31 and increased muscle activity in force-dissipating muscles, such as the knee and hip extensors.32 Higher gluteus medius activation that was observed at +15% could further contribute to the decreased hip drop. Additionally, uphill gradients alter foot strike patterns, promoting a shift toward mid- to forefoot strikes,6 which are associated with reduced loading rates during running.33 The reduction in lumbar lordosis is consistent with the findings of Levine et al.15 The decreased pelvic tilt at +5% and +10%, which typically correlates with smaller lumbar lordosis in level running,34 together with the observed shift in trunk inclination towards a forward-leaning position, could contribute to the decreased lumbar lordosis. The change in trunk inclination likely affects load distribution across the knee, hip,35 and potentially the lower back, although its impact on lower back loading remains unexplored.
Muscle Activity
In discussing the findings of this study, it is evident that slope-induced changes in running biomechanics influence muscle activation patterns in both uphill and downhill running. Increased muscle activity in the gastrocnemius at -15% and vastus lateralis across all downhill gradients may be attributed to the heightened forces required for energy dissipation,8 consistent with previous research.6 Although not statistically distinct, the gluteus maximus, gluteus medius, and biceps femoris consistently showed numerically higher activation across all downhill gradients compared to level running. This lack of a statistically clear difference may be related to the greater proportion of eccentric-based muscle actions involved in downhill running.11 These eccentric contractions generate greater forces at the same activation level,36 which may be sufficient to manage the heightened forces without an increase in muscle activity.
The increased muscle activity in some lower limb muscles during uphill running aligns with the demands of overcoming the incline.6 These findings indicate that uphill running at gradients of +5%, +10%, and +15% requires greater force production from the lower limbs, as reflected by increased EMG activity in specific muscles such as the gastrocnemius, vastus lateralis, and biceps femoris.
The tendency for increased obliquus externus activity during steep downhill running may be explained by the greater lumbo-pelvic rotation in the transverse plane, which is facilitated by the longer stride length.37 Interestingly, despite its role in stabilizing the lumbar spine and preventing excessive curvature,38,39 the rectus abdominis did not exhibit a notable increase in activity during downhill running.
A notable finding from this study is the significant decrease in erector spinae muscle activity during all gradients except of -15% and +5%. Reduced activity of erector spinae during downhill gradients may prevent increasing the lumbar lordosis further, which would shorten the muscle and possibly lowers activation potential, respectively. The typical backward-leaning trunk position seen during downhill running may also enhance lumbar lordosis through compressive forces acting upon ground contact.
Physiological Demands
The observed changes in HR and RPE highlight the differing physiological and perceptual demands of graded running. Apparently, RPE for downhill running did not reflect cardiocirculatory strain but may have been elevated due to high-impact forces on musculoskeletal tissues, which can reduce muscle function, and increase RPE.40–43 The elevated RPE seems to be more pronounced in novel bouts of downhill running, highlighting the importance of structuring grade-specific downhill training. During uphill running, both HR and RPE exhibited a predictable increase, consistent with previous research.6,13
METHODOLOGICAL LIMITATIONS
Lumbar lordosis was assessed using data derived from markers applied to the skin, which can detect changes in lumbar curvature, though the absolute values may be uncertain due to soft tissue movements.44 Additionally, sEMG measurements estimate activity from a single muscle area and are susceptible to crosstalk.45 Furthermore, muscle activity during the stance phase varies depending on treadmill mechanics and differs from overground running.46 Therefore, caution should be exercised when transferring these results to running on surfaces other than a treadmill. Finally, only healthy runners were included in the study. This limits the generalizability of the findings, as individuals with low back pain may exhibit different biomechanical patterns.
PRACTICAL APPLICATIONS
The slope-specific physiological, biomechanical, and neuromuscular demands should be considered in training as well as prevention and rehabilitation of running injuries. For load buildup in slope running, especially for runners with pre-existing back issues, a gradual progression starting with uphill running, followed by level and finally downhill running may be advisable. Downhill running may require focused training to improve eccentric control and shock absorption, with activation of the posterior kinetic chain of the lower limb potentially aiding in the management of eccentric load and impact forces.
CONCLUSION
Graded running, including both downhill and uphill, imposes distinct biomechanical, neuromuscular, and physiological demands. Tailored training protocols may help to enhance performance, prevent injuries, and support rehabilitation, with special attention to slope-specific adaptations and pre-existing conditions.
Future studies should address the role of fatigue, refine methodological approaches, and focus on injury prevention and rehabilitation to enhance understanding of and safety in slope-specific running. Research specifically involving individuals with low back pain is also warranted, as their responses may differ from those of healthy runners.
Conflicts of interest
The authors report no conflicts of interest.