INTRODUCTION
Anterior cruciate ligament (ACL) tears are traumatic, acutely debilitating, and have significant long-term impacts on knee health.1 An estimated 250,000 ACL injuries occur annually within the United States.2 Fifty percent of people with an ACL injury will develop symptomatic knee osteoarthritis (OA) within 5-15 years of injury, with rates reaching up to 80% at 20 years after ACL reconstruction (ACLR).3,4 Given that most ACL injuries occur in athletes under 30 years old,2 these individuals will develop early onset knee OA 15-20 years younger than their uninjured counterparts who develop idiopathic OA.5 This high rate of early onset OA after ACL injury carries a large socioeconomic burden stemming from chronic pain, greater years of disability, limitations in societal and work-related participation, increased demand for knee joint arthroplasties, and increased rate of revision arthroplasty.5–10 Thus, there is a critical need to better understand the modifiable factors in early OA development after ACL injury that can be targeted by accessible secondary preventative interventions.
Altered knee joint loading, measured through metrics such as a knee flexion moment, is one factor driving the initiation of early knee OA.11 For example, smaller knee moments during walking at six months after ACLR is associated with worse cartilage relaxation values, a metric of cartilage microstructure.12 Articular cartilage is avascular, aneural, and uniquely reliant on mechanical stimuli and the synovial fluid environment for maintenance of tissue health.13,14 Activities that dynamically load the articular cartilage, such as squatting and walking, are protective by facilitating metabolism and synthesis of proteoglycans and collagen within the extracellular matrix (ECM) of cartilage.11,15 The relationship between knee joint loading and cartilage structure has been demonstrated in uninjured knees, where larger knee joint moments have been shown to associate with thicker cartilage.16 Meanwhile, reduced proteoglycan content and cartilage thickness are seen following periods of joint unloading or immobilization in the knee, indicating the importance of adequate joint loading to cartilage health.17,18
Standard post-operative rehabilitation for patients during the first three months after ACLR focuses on restoring knee motion, reducing joint effusion, and building quadriceps strength.19 While these goals maintain an emphasis on function, they lack the precision to imprint healthy movement patterns and restore normal joint loading in the early post-operative period. Previous work has shown asymmetric knee joint loading during squatting and aberrant squat biomechanics are linked with more risky movement patterns during drop vertical jumping and subsequent second ACL injury.20–22 Given that atrophic cartilage changes are detectible by magnetic resonance imaging (MRI) within two months of ACLR through quantitative measurements such as T2 relaxation time,23–27 a marker of water content and collagen organization in cartilage, there is a need for early intervention strategies aimed at restoring healthy joint biomechanics.
To promote improved movement patterns early after ACLR, a visual biofeedback program was developed to be utilized during bodyweight bilateral squats aimed to improve symmetric knee biomechanics, implemented during the first months of rehabilitation after ACLR. The squat visual biofeedback program was developed within a multidisciplinary team and is delivered utilizing current best practice methods for post-operative rehabilitation after ACLR.19 The results of this study will inform the future development and testing of comprehensive knee loading rehabilitation interventions that seek to optimize both the magnitude and frequency of knee joint loading to prevent early knee OA after ACL injuries.
MATERIALS AND METHODS
Study Aim, Design, and Setting
This will be a prospective, parallel, randomized controlled trial28 with a primary aim to evaluate the efficacy of an eight-week squat visual biofeedback program implemented early after ACLR to improve symmetric knee joint biomechanics and knee cartilage microstructure. The trial will be conducted at single site (University of Nebraska Medical Center [UNMC]) in Omaha, Nebraska (United States) in the following spaces: Clinical Movement Analysis Laboratory, Center for Advanced Magnetic Resonance Imaging, and Center for Healthy Living. The primary end points will be immediately post-intervention (knee joint biomechanics) and six months after ACLR (with cartilage microstructure measured on quantitative MRI). The study is approved by the UNMC Institutional Review Board (IRB# 0652-21-FB) and prospectively registered at clinicaltrials.gov (NCT05363683).
Participants
Thirty-four individuals between the ages of 13-35 with an acute ACL injury within the prior six months will be included in this study. Participants will be enrolled within one month of ACLR. If enrolled prior to surgery, ACLR must be planned. Persons will be excluded if they have had previous ipsilateral knee injury or surgery, concomitant posterior cruciate ligament reconstruction or cartilage restoration procedure, body mass index over 35 kg/m2, current pregnancy, or planned pregnancy during study duration.
Recruitment and Enrollment
Local orthopedic surgeons, physical therapists, and athletic trainers will identify eligible patients in their clinical practices. Interested persons will provide verbal consent to meet with a member of the study team during a clinic visit or for their medical team to provide their name, phone number, and/or email to a member of the study team. The person will be contacted by the research team to discuss study participation.
Other interested persons that have not been identified in local clinics will be reached through study flyers posted across the community and social media accounts. Individuals will be directed to an online screening survey within REDCap electronic data capture tools hosted at University of Nebraska Medical Center. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies.29 REDCap at University of Nebraska Medical Center is supported by the Research IT Office funded by the Vice Chancellor for Research (VCR). This publication’s contents are the sole responsibility of the authors and do not necessarily represent the official views of the VCR. Persons who meet initial REDCap screening criteria will be contacted by the research team to confirm eligibility.
Participants will present in-person with the research team either before ACLR or within one month of ACLR to complete study enrollment and begin physical therapy treatment. All participants will provide written informed consent prior to study testing and intervention.
Randomization Allocation, Concealment, and Blinding
After ACLR, participants will be randomized in a 1:1 allocation ratio to either the visual biofeedback group or standard-of-care group across six strata based on presence of concomitant meniscal repair (either present or absent), concomitant meniscectomy (either present or absent), or history of contralateral ACL injury to reduce variability by distributing these factors evenly between the visual biofeedback and standard-of-care group. Concomitant meniscal procedures will be identified from the participant’s operative report obtained from the treating surgeon after ACLR. For each stratum, randomization will be performed using a block randomization schedule with blocks of 2. A randomization schedule was created a priori by an administrative assistant not involved with any other aspect of this study. A random number generator will be used to generate a number between 0-1 to the first individual in each block. If that number is <0.50, the first individual will be enrolled in the visual biofeedback group. The subsequent participant assigned to that same block will be enrolled in the standard-of-care group. If the number is ≥0.50, then the first individual in that block will be enrolled in the standard-of-care group with the subsequent individual enrolled in the visual biofeedback group. To ensure appropriate concealment, group allocation for the first participant within each block will be kept within a sealed envelope.
This is a planned double-blinded study. Study team members conducting study assessments will be blinded to group allocation. To blind participants to study group, individuals in both groups will complete their respective squat protocol while standing on two portable force plates. The physical therapists leading the treatment sessions and squat protocol cannot be blinded to group allocation owing to the type of physical therapy intervention.
Rehabilitation and Interventions
Participants in both the visual biofeedback and standard-of-care groups will complete the University of Delaware ACL post-operative PT protocol in which squatting is included within the early and middle stages of rehabilitation after ACLR to promote lower extremity strength and improved biomechanics.19 This protocol provides a clinically benchmarked strategy for ACLR rehabilitation. Its characteristics include the use of frequent and valid quadriceps strength testing, immediate use of open kinetic chain exercise, standardized home exercise programs, and criterion-based progressions for running, sprinting, plyometrics, agility, cutting/pivoting, and return to competition. A licensed physical therapist will directly supervise all PT sessions.
Following randomization, participants will undergo pre-intervention testing and begin the visual biofeedback or standard-of-care squat protocol at either two weeks after ACLR or when 50% weightbearing is allowed by the treating surgeon. All participants, regardless of group allocation, will complete the same number of sets and repetitions of bilateral bodyweight squats during the squatting intervention period, completed twice weekly over a period of eight weeks (16 total sessions). Participants in both groups will complete squats while standing with each foot on a separate portable force plate with raw data collected for exploratory analyses (495 X 595mm, Bertec Corporation, Columbus, Ohio). Participants in the visual biofeedback group will receive real-time visual feedback on a television screen during all squats. In contrast, the control group will receive no visual feedback but will be provided standard verbal instructions at the beginning of each set of squats (keep knees in line with toes, keep hips back, keep equal weight on each foot). Participants will be instructed to complete squats up to 90° of knee flexion, as able. At least 30 seconds of rest will be provided between each set.
The visual biofeedback and standard-of-care interventions integrate evidence-based motor learning principles to support neuroplasticity that results in improved functional performance, including 1) repeated skill practice (i.e., 2x/week for 8 weeks); 2) external focus of attention (i.e., visual biofeedback protocol); 3) implicit learning (e.g., avoiding cues such as standing shoulder-width apart); 4) differential learning (e.g., completed with varying arm positions [crossed over chest, straight out in front, or at side], varying environments [loud music, different rooms, different people around], and different times during the rehabilitation session); 5) self-controlled learning (self-controlled feedback schedules regarding squat symmetry after each set in visual biofeedback protocol) and 6) contextual interference (varied visual feedback during weeks 7 and 10 of visual biofeedback protocol).30
Visual Biofeedback Squat Intervention
The visual biofeedback squat intervention has been designed to promote symmetric movement patterns and shift muscular demands to the quadriceps without requiring additional treatment time. It provides participants with ground reaction force (GRF) and/or center of pressure (COP) feedback that is projected in real-time on a screen in front of the participant. The visual biofeedback program was developed using Matlab R2023a (Mathworks, Natick, MA).
Visual biofeedback conditions will be progressed from simplest level (GRF only) to most complex (GRF+COP) with standard verbal instructions provided for each condition (Table 1). The goal of GRF feedback was to promote symmetric magnitude of GRF between each limb. The goal of the COP feedback was to promote symmetric anterior-posterior position of the COP between each limb. Individuals after ACLR squat with intralimb compensations that redistribute joint moment contributions away from the knee to the hip and ankle joints.21,31,32 COP position predicts the magnitude of these intralimb joint moment compensations during squatting33; therefore, COP was chosen as a visual biofeedback target in addition to GRF. If squat protocol appointments are missed, a participant will be progressed to the next level only after completing at least 75% of the sessions at a specific level with four sessions (e.g., must complete at least three sessions in Level 1 before progressing to Level 2) or 50% of sessions at a specific level with two sessions (e.g., must complete at least one session in Level 3 before progressing to Level 4) (Table 1). Interlimb threshold levels will be standardized initially and progressed based on individual interlimb accuracy. Accuracy was defined and measured as the percent time during a single set that the participant remained within the thresholds for the respective condition. Initial interlimb thresholds and threshold progressions were established based on prior pilot testing.
Standard-of-Care Squat Intervention
The standard-of-care group will not receive any visual feedback. Standard verbal instructions provided will be provided at the beginning of each set of squats (“I would like you to squat keeping your knees in line with toes, hips back, and weight evenly balanced between your feet”).
Data Collection and Management
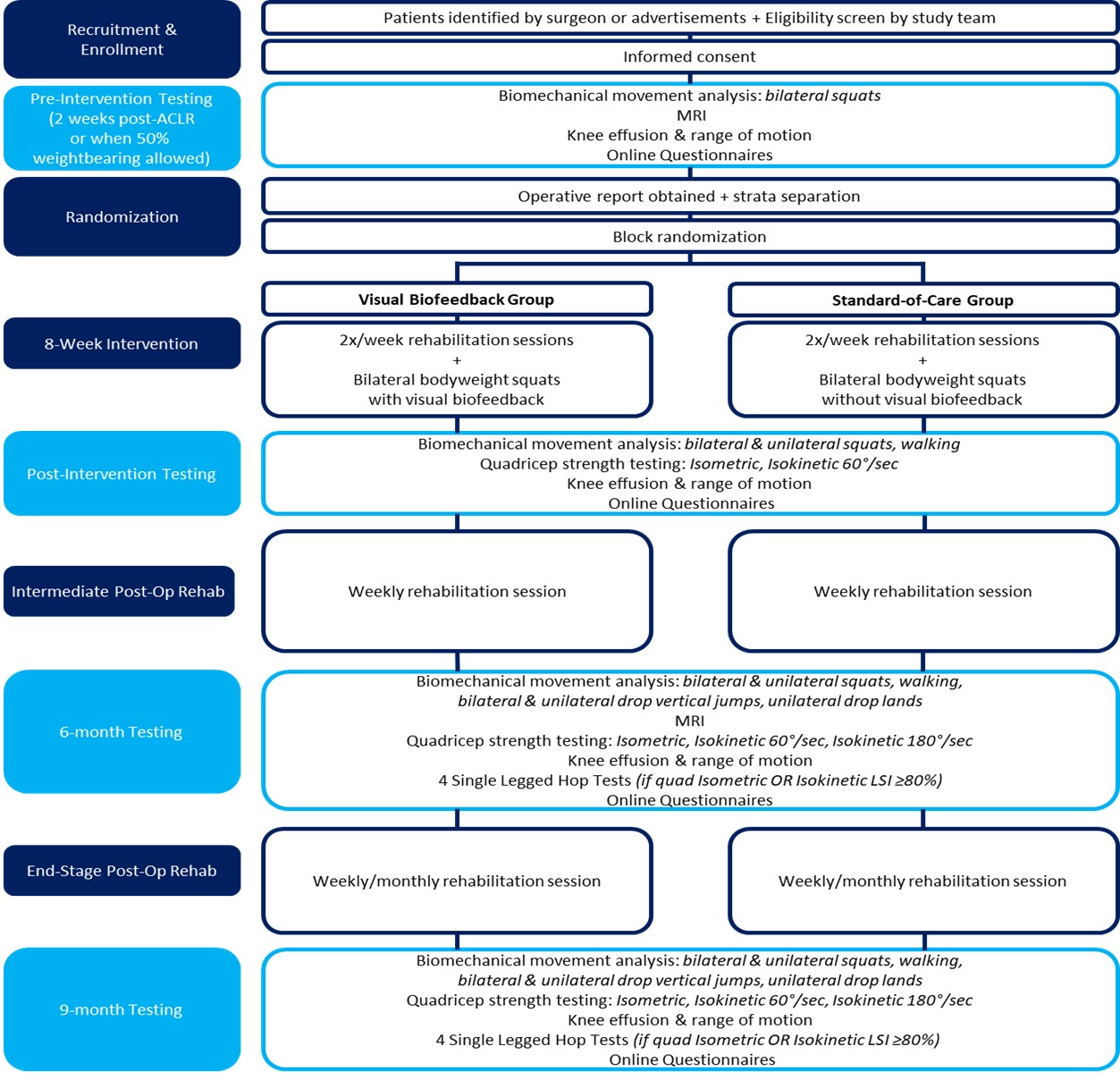
Participants will undergo testing after ACLR at pre-intervention, post-intervention, six months post-ACLR, and nine months post-ACLR as outlined in Figure 1. Pre-intervention testing will be completed prior to initiation of the squat protocol at two weeks after ACLR or when 50% weightbearing is allowed. Participants will complete post-intervention testing within one week of completing the squat protocol.

Data will be collected and managed within REDCap software hosted at UNMC. Data manually measured during testing sessions (e.g., knee range of motion, effusion, height, mass) will be initially recorded on paper with subsequent double data entry into REDCap. Data collected electronically (e.g., muscle strength, biomechanics) will be stored on UNMC-supported Box data storage.
Outcomes
Participant Characteristics
Table 2 provides an overview of participant demographics, surveys and physical function tests that will be collected throughout the study. Demographics and participant characteristics will be self-reported within REDCap surveys during pre-intervention testing. The operative report will be obtained from each participant’s treating surgeon after ACLR and surgical details including date, graft type and concomitant injuries and procedures will be recorded. At each of the four testing sessions, height and body mass will be measured using a standard stadiometer and scale.
Primary Outcomes
Knee flexion moment impulse during squatting at post-intervention
Abnormal joint loading during squatting is associated with early cartilage degradation after ACLR.11 Given this, three-dimensional biomechanical movement analysis will be conducted during bilateral bodyweight squats following the completion of the visual biofeedback intervention. Biomechanics will be captured using a 16-camera motion capture system (Qualisys AB, Göteborg, Sweden) integrated with three embedded force plates (Bertec Corporation, Columbus, Ohio). A retroreflective marker set previously described will be placed on each participant.34 Participants will complete 3 sets of 5 bilateral bodyweight squats with arms crossed at the chest. Participants will be instructed to complete squats at a speed of three seconds during squat descent and three seconds during squat ascent using a metronome set at one-second increments. The external knee flexion moment will be calculated using an inverse dynamics approach.35 Knee joint loading will be assessed utilizing the interlimb ratio of knee flexion moment impulse throughout descent and ascent phase of the middle three squats of each set (nine total squats).
Change in cartilage microstructure from pre-intervention to six months after ACLR
Changes in cartilage structure and composition are detectible by MRI within two months of ACLR.23–27 Therefore, a 3-Tesla MRI scanner will be used to obtain T2 maps of the injured knee using MRI procedures and parameters established by the Osteoarthritis Initiative, a nationwide, multi-center research study aimed to understand and prevent knee OA.36,37 All MRI procedures will be performed without contrast. Custom computer programs developed in Interactive Data Language (IDL; Harris Geospatial Solutions Inc., Broomfield, CO, USA) will be used to calculate T2 maps and extract mean T2 relaxation times from segmented cartilage regions of interest. T2 relaxation times are sensitive to detect alterations in collagen organization and water content.38,39 MRIs will be read by a board-certified musculoskeletal radiologist for incidental findings. The percent change in cartilage T2 relaxation time from two weeks to six months after ACLR will be calculated, with an increase in T2 relaxation time representing negative cartilage health.
Secondary Outcomes
Knee flexion moment impulse interlimb ratio during squatting at six months after ACLR
The interlimb ratio of the knee flexion moment impulse during bilateral squatting will be collected at six months using the same methods described above to assess the carryover effect of the squat intervention.
Gait biomechanics at post-intervention and 6 months after ACLR
Gait asymmetries are common following ACL injury and have been shown to persist up to 6-12 months after ACLR.40 Dynamic mechanical loading during activities such as squatting and walking is protective for articular cartilage11 by facilitating proteoglycan and collagen synthesis. Restoring gait symmetry following ACLR may be another indicator of healthy loading to minimize risk of early knee OA. Gait biomechanics will be collected using the same 3D motion capture system used for bilateral squats. Participants will walk at a self-selected speed that will be maintained within ±5% at six months. Variables of interest will include the interlimb ratio of the peak external knee flexion moment during stance phase.
Quadriceps muscle strength at post-intervention and six months after ACLR
Quadriceps weakness is an established independent risk factor for development of OA,41–44 and deficits in quadriceps function have been shown to persist for years beyond ACL injury and reconstruction.45 Quadriceps strength will be assessed at post-intervention and 6 months after ACLR both isometrically at 90° and isokinetically at 60°/second on an isokinetic dynamometer (Biodex, System 4™, Biodex Medical Systems Inc. USA). A maximum of three recorded maximal effort isometric trials will be completed. One set of five consecutive alternating repetitions of concentric knee extension and concentric knee flexion will be recorded. The interlimb ratio of the peak value of isometric and isokinetic quadriceps strength will be calculated, respectively.
Exploratory Outcomes
Measures of knee function
At each testing session, active knee flexion and extension will be measured using a standard goniometer. Knee effusion will be assessed and using the modified stroke test and a 5-point semiquantitative grading scale.46 At six- and nine-month testing, four single-legged hop tests will be assessed as previously described47 if isometric or isokinetic quadriceps strength is at least 80% compared to the uninjured limb. Hop testing will not be completed if quadriceps strength is less than 80%.
Quadriceps muscle strength
Isometric quadriceps strength at 90° of knee flexion and isokinetic quadriceps strength at 60°/second will be assessed as an exploratory outcome at nine months after ACLR. Additionally, isokinetic quadriceps strength at 180°/second will be assessed at 6 and 9 months after ACLR.
Additional Biomechanical Outcomes
Bilateral squats and gait at a speed of ±5% from post-intervention testing will also be assessed at nine months after ACLR. Unilateral squats on each limb will be completed at post-intervention, six months and nine months after ACLR using the same methodology as outlined above for bilateral squats. Five trials each of bilateral drop vertical jumps, unilateral drop lands at each limb, and unilateral drop vertical jumps at each limb will be completed at nine months after ACLR from a 31-centimeter box using previously described methods.48,49
Patient-Reported Outcomes
Participants will complete the Grit Scale,50 Global Rating Scale,51 International Knee Documentation Committee Subjective Knee Form 2000 (IKDC),52 Tampa Scale of Kinesiophobia (TSK-11),53 Numeric Pain Rating Scale (NPRS),54,55 ACL Return to Sport after Injury Scale (ACL-RSI),56 Knee injury and Osteoarthritis Outcome Score (KOOS),57 Anterior Knee Pain Scale (AKPS),58 Marx Activity Rating Scale,59 European Quality of Life 5 Dimensions (EQ-5D),60 and Knee-Self Efficacy Scale61–63 within REDCap surveys at time points outlined in Table 2. In addition, participants will complete survey questions pertaining to return-to-sport clearance, current sports and activity level, current muscle strengthening, information sources, and ACL knowledge at nine months after ACLR.
Sample Size
Sample sizes were calculated for each of the primary outcomes: knee flexion moment impulse interlimb ratio during bilateral squatting and knee cartilage structure measured by T2 relaxation times. A sample size of 20 (10 per group) achieves 82.5% power to detect a difference in the knee flexion moment impulse interlimb ratio of 0.283 during squatting between the visual biofeedback (expected interlimb ratio=0.800±0.183) and standard-of-care group (expected interlimb ratio=0.517±0.228) using a two-sided hypothesis test and a=0.05. Group differences are based on our previous preliminary data from a prospective cohort study of participants receiving standard-of-care post-operative PT: knee flexion moment impulse interlimb ratio at four months (N=20):0.517±0.228; knee flexion moment impulse interlimb ratio at 10 months after clearance to return to sport (N=5):0.971±0.183. It is anticipated that post-intervention testing of bilateral squat biomechanics will occur on average at 3.5 months after ACLR. Thus, it is not expected that the visual biofeedback group will achieve a knee flexion moment impulse interlimb ratio of 0.971 demonstrated by participants in our preliminary data at 10 months after ACLR. Accordingly, a more conservative estimate of the knee flexion moment impulse interlimb ratio of 0.800±0.183 was used for the visual biofeedback group at post-intervention.
To test group differences in cartilage T2 relaxation time, a sample size of 30 (15 per group) achieves 81.0% power to detect a group difference of 2.9±2.7 milliseconds in T2 relaxation time. We are using this expected group difference based on the reported change in T2 relaxation time of 2.2±2.4 ms in the medial femoral cartilage by six months after ACLR as reported by Kumar et al.64
To account for the sample sized required for both primary outcomes and expected attrition, a total of 34 participants will be enrolled in this study.
Statistical Analysis
To test the efficacy of the squat biofeedback intervention to improve symmetric knee joint biomechanics, analyses of covariance will be used to test group differences in the interlimb ratio (equal to injured limb / uninjured limb) of the knee flexion moment impulse during squatting at post-intervention after adjusting for baseline knee flexion moment impulse during squatting at pre-intervention. To test the squat intervention’s efficacy to improve structural knee cartilage health measured by MRI T2-relaxation times, independent t-tests will be used to test the difference in the change in cartilage T2 relaxation time in the injured knee from two weeks to six months after ACLR between visual biofeedback and standard-of-care groups. If assumptions for any of these tests are violated, a nonparametric test will be conducted. Covariates such as age and concomitant injuries will be explored.
Patient and clinician involvement
Three clinician partners (two physical therapists with 10+ years of clinical experience, one physical therapist with 30+ years of clinical experience) were engaged throughout the design and planning of this study. They provided guidance on the research objectives, funding applications, physical therapy protocol, and design of the visual biofeedback intervention to make clinical implementation feasible in the future. They also participated in the development and design of physical therapy home exercise programs. Participants in this study will complete post-study surveys to obtain patient perspectives on completion of the study intervention and participation within the study.
Monitoring
The principal investigator, research coordinator, physical therapists, and other members of the research team will remain in close contact and meet bi-monthly to monitor recruitment, participant timelines, data management, and adverse events or other issues. Protocol implementation and efficacy will be monitored throughout as part of bi-monthly meetings between members of the research team. Fidelity checks of assessment methods (i.e., knee range of motion and effusion) and study interventions (i.e. quadriceps exercises, use of neuromuscular electrical stimulation, and squatting exercises) will be completed by a study team member (board certified in sports PT) not completing treatments or outcome assessments. Results will be reported to the research team.
Study Adherence
Several strategies will be used to promote study adherence by enrolled participants. Participants will be provided text message reminders for physical therapy treatment sessions, study testing sessions, and wearing physical activity monitors. Participants will receive gift cards for participating in testing sessions and returning physical activity monitors with valid data. Treatment sessions will be conducted 1:1 by physical therapists with expertise in treating patients with ACL injury and who have orthopedic and sports certifications in physical therapy from the American Board of Physical Therapy Specialties. Participants will be given summary sheets after each testing session to provide knowledge of their recovery according to objective clinical milestones. These measures include knee effusion, range of motion, global rating scale, IKDC, ACL-RSI, quadriceps strength, and single-legged hop tests. A biomechanics summary of squats and drop vertical jumps will be given to participants at nine months. The summaries will be shared with the participant’s treating surgeon to aid in shared decision-making. A lay description of testing details and clinical targets will be provided to participants. A clinical description of testing details and clinical targets will be provided to treating surgeons.
Dissemination
The findings of the study will be disseminated at relevant scientific and professional conferences and published in relevant peer-reviewed journals. Important protocol amendments will be reported to the IRB and registered through U.S. National Library of Medicine clinical trials registry (clinicaltrials.gov). Study participants will be provided with a lay summary of findings.
Discussion
ACL injury rates continue to rise within the US and around the world with a 75% increase over a recent 15-year period.65–67 The onset of post-traumatic knee OA presents a significant healthcare and societal burden. Currently, there are limited interventions available to mitigate the early onset of OA. Reduced joint loading has been shown to be a contributing factor in the initiation of post-traumatic knee OA.68 This trial will determine the efficacy of an eight-week visual biofeedback program aimed at improving involved limb joint loading, initiated two weeks after ACLR or when cleared for 50% weight-bearing by the treating surgeon, by assessing changes in movement biomechanics and cartilage microstructure changes on MRI. Successful completion of this project will establish a rehabilitation intervention that effectively and optimally loads the knee joint early after ACLR, providing the initial steps in our work to prevent OA after ACL injury.
CONCLUSION
This randomized controlled trial will represent an important step towards identifying potential secondary prevention interventions to reduce the rate of post-traumatic knee OA following ACL injury. The results of this study will inform the future development and testing of comprehensive knee loading rehabilitation interventions that seek to optimize both the magnitude and frequency of knee joint loading to prevent early knee OA after ACLR.
Disclosures
The authors have no professional relationships with companies or manufacturers who will benefit from the results of the present study. Other conflicts include the following: EW is funded by the following: U54GM115458; R01AR080346; R15AG085105; R34AR083077; Arthritis Foundation Osteoarthritis Clinical Trials Network (OACTN) Clinical Trial Unit; MT serves on the editorial board for Current Review in Musculoskeletal Medicine, provides consulting for NewClip and Vericel, and owns stock in Overture and NeAT Surgical; BS is an associate editor for the Journal of Magnetic Resonance Imaging and was not involved in the editorial review or the decision to publish this article. For the remaining authors, no conflicts were declared.
Acknowledgements
This work was supported by the Nebraska Research Initiative and the National Institute of General Medical Sciences, U54 GM115458, which funds the Great Plains IDeA-CTR Network. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.