


INTRODUCTION
Traumatic anterior shoulder instability is a prevalent issue, particularly among young athletes and individuals leading active lifestyles. It frequently arises in those engaged in high-impact activities and contact sports. After experiencing a primary instability event, there is a high likelihood of recurrence. It has been reported that subjects who experience primary instability event who are under the age of 20 have a 90% chance of recurrent instability, while subjects 20-30 years old have a 70-82% chance of recurrence.1 To address this persistent issue and restore stability to the glenohumeral joint, many opt for surgical stabilization procedures. While the arthroscopic Bankart repair stands as the preferred surgical approach in the United States, studies have described recurrent instability rates of 6-50%.1 Subsequent instability events lead to increased time away from sport and may also lead to further disruption to the bony anatomy of the glenohumeral joint, rendering it even more unstable. The risk factors for recurrence of anterior shoulder instability following Bankart repair are multifactorial, reflecting a combination of variables. The Latarjet procedure is a well-established method for stabilizing recurrent anterior shoulder instability, boasting reported recurrent dislocation rates of only 3-15%.2 The Latarjet is particularly advantageous in cases where subjects exhibit a glenoid bone loss of >20%, engage in contact or competitive sports, or demonstrate ligamentous laxity. This procedure has been suggested to yield superior outcomes regarding failure rates with similar return to sport at preinjury level rates of 81% compared to 84% after arthroscopic Bankart repairs, but with a higher complication rate.3
A recent systematic review showed that the return to play rates following an open Latarjet procedure ranged from 72%-96.8% compared to a range of 61.5%-94.1% following an arthroscopic Bankart repair.4 Another systematic review that studied the results and outcomes of the Latarjet procedure in overhead athletes, demonstrated a 90.3% return to play rate with 80.6% returning to the same level of play. That systematic review primarily included a male cohort with 86.9% of 2,134 included cases being male athletes with a mean age of 25.4 years.5
Epidemiological and prognostic variances between male and female orthopedic subjects have been extensively documented across the health spectrum. These differences stem from a complex interplay of anatomical, hormonal, and genetic factors. For example, it has been well established that coracoid and glenoid anatomy differs between males and females, which may affect their outcome or potentially render them unfit for the Latarjet procedure. There is a paucity of research looking at the outcomes of the Latarjet procedure in female subjects. Understanding the sex-related distinctions is crucial in tailoring effective treatment strategies and optimizing outcomes for both male and female subjects. The purpose of this case report was to assess the long-term outcome and return to sport relative to preinjury level of a Division 1 women’s basketball player following a Latarjet procedure.
CASE DESCRIPTION
The subject was a right hand dominant, 23-year-old female, who was actively competing in Division 1 women’s basketball as a point guard. The subject had sustained >five dislocations and/or subluxations on her dominant/shooting arm over the course of her collegiate (four-year) basketball career. She attempted conservative management with bracing, physical therapy, and anti-inflammatory medication for six weeks following her most recent dislocation event before electing to undergo surgical repair. The subject underwent an arthroscopic anterior labral repair followed by formal rehabilitation and returned to sport at eight months post-op during her junior year. The subject then sustained a shoulder dislocation following clearance to return to sport (eight months post-op) at practice while attempting a single-arm, overhead pass with the shoulder in abduction and external rotation position. This event was followed up by a subsequent dislocation that occurred while lying in bed. An MRI was obtained revealing an anterior labral tear, bony Bankart lesion involving ~10% bone loss, and a Hill-Sachs lesion measuring 24mm x 15mm x 5mm. Based on timing of the commencement of the season, desire to improve her collegiate body of work prior to the WNBA draft, and her recurrent instability, she elected to explore further surgical interventions. In this case, the surgeon evaluated the subject’s preoperative imagining and determined that the coracoid had adequate dimensions and morphology to support safe and effective grafting, and the decision to move forward with a Latarjet procedure. It should be noted that certain coracoid morphologies may present contraindications to this technique. Specifically, a small, dysplastic, or excessively curved coracoid may not provide adequate bone stock or surface area for secure fixation, compromising the structural integrity and biomechanical effectiveness of the graft.
SURGICAL PROCEDURE
The subject was placed in the modified beach-chair position for the procedure A subscapularis split was performed in the lower one-third/two-thirds section of the subscapularis. The capsule was identified and incised in the shape of a reverse L. Previously placed suture anchors were removed, and the anterior neck was prepared using a burr and a hand-held saw to create a bleeding surface. The graft was placed flush with the articular surface and two screws were placed with good fixation. Palpation demonstrated no step-off or overhang. There was good compression and good tension on the conjoint tendon. The L’d capsule was then repaired using a 1.8 mm FiberTak™ anchor placed between the 2 screws and the inferior capsular was shifted over the top of the coracoid. The superior leaf was then closed to that. The lateral edge of the subscapularis split was closed lateral to the conjoint tendon. Typical closure was performed, and she was placed in a sling.
EXAMINATION
The subject was referred to physical therapy the day after undergoing the open Latarjet procedure. The subject was examined at baseline by the physical therapist (day one post-surgery), and then re-examined at two months, and four months post-operative. An additional examination occurred postseason (nine months post-operative) to obtain follow-up outcomes. Performance measurements were obtained at four months (return to sport-specific activities) and nine months (post season).
All ROM measures were taken with the subject lying in the supine position. A two-tester range of motion method was utilized in which one tester stabilized the scapula and passively moved the shoulder joint to the end of the available glenohumeral range of motion. The second tester aligned the axis of rotation and the goniometer arms to the anatomical landmarks.6 The literature reported good reliability with ICC ranging from 0.85 to 0.97 and a MDC of 7.11° for shoulder flexion, 7.48° for external rotation at 0° of shoulder abduction, 8.03° for external rotation at 90° of shoulder abduction, and 4.93° for internal rotation at 90° of shoulder abduction utilizing the technique described.7
To objectively test muscular strength, endurance, power, and performance, a battery of upper extremity tests was used to help assess readiness to return to sport. This specific testing battery was utilized to objectively assess strength, power, endurance, and the kinetic chain. Strength, power, and endurance encompass many components, such as peak force, rate of force development, fatigue resistance, and velocity of contraction. Shoulder strength requirements are sport and position specific.8
To measure pain, shoulder function, and the subject’s satisfaction with shoulder function, the Pennsylvania Shoulder Score (PSS) was used. This self-report questionnaire has been shown to be a reliable and valid measure for reporting outcomes of subjects with various shoulder disorders.9 The PSS consists of 24 questions (three items for pain, one item for satisfaction with function, and 20 items for function). The score ranges from 0 to 100, where 100 indicates no pain and full function and subject satisfaction. The minimal clinically important difference (MCID) for improvement was 11.4 points.9
The Single Assessment Numeric Evaluation (SANE) is a subject rating from 0-100. Subjects rate their current illness score in relation to their pre-injury baseline.10 The SANE is regarded as a valid and reliable tool to assess subject outcomes across operative and non-operative shoulder conditions. The MCID is 15% and the SANE is a simple and efficient tool to assess treatment effects for shoulder disorders.11
The QuickDASH is a region-specific measure of disability and symptoms in subjects with musculoskeletal disorders of the upper limb.12 The QuickDASH is a shortened version of the Disabilities of the Arm, Shoulder and Hand (DASH) that uses 11 items to measure the degree of difficulty a subject may have in performing various physical activities due to shoulder, arm, or hand problems (six items); the severity of pain (two items); and the problem’s effect on social activities, work, and sleep (three items).12 If at least 10 of the 11 items were completed, the responses to the items were added up to form a raw score, then converted to a 0-100 scale with higher scores indicating greater disability. The MCID for improvement is 15.91 points.12 The optional sports module of the QuickDASH was also completed by the subject. This specific, four-item sub-section assesses the impact that the arm, shoulder, and/or hand injury has on the subject’s ability to perform her sport.
The Optimal Screening for Prediction of Referral and Outcome Yellow Flag (OSPRO-YF) tool was utilized with this subject to assess negative mood, fear avoidance, and positive affect and coping.13 The OSPRO-YF is a reliable and valid concise, multidimensional yellow flag tool applied and utilized to screen for psychological distress in orthopedic physical therapy practice. The 17-item OSPRO-YF includes six items from negative mood questionnaires, six items from fear-avoidance questionnaires, and five items from positive affect/coping questionnaires. It assesses eleven psychological constructs across three psychological domains of self-efficacy and acceptance, negative pain coping, and negative mood.14 Based on the responses the subject gives, the screening tool generates a score estimate for each construct. Scores above the 75th percentile in negative pain coping or negative mood constructs or below the 25th percentile in self-efficacy/acceptance constructs are marked with a yellow flag. The summary OSPRO-YF score for a subject is a count of the number of constructs with yellow flags.13
On the subject-reported outcomes (PROs) given during the post-operative evaluation, the subject reported increased upper extremity disability, psychological distress, and decreased satisfaction with shoulder function. During the physical therapy evaluation, the post-operative dressings were removed and replaced with new dressings. The incision site and sutures were clean and dry with no sign of infection. The subject was tender to palpation in the areas adjacent to the incision site. She reported 8/10 shoulder pain on the numeric pain rating scale during the evaluation. Due to strict postoperative range of motion precautions, objective measurements were limited to 90 degrees of passive shoulder flexion and 30 degrees of passive shoulder external rotation in the scapular plane. Strength testing was deferred due to acuity and postoperative precautions. The subject’s sensation was intact to light touch, and she exhibited adequate motor control of her wrist, hand, and fingers. The subject’s goal for physical therapy was to return to basketball practice and games without limitations in time for the season which was set to begin five months from the initial evaluation.
CLINICAL IMPRESSION
The subject presented to initial physical therapy evaluation with typical post-operative strength deficits, early range of motion precautions and limitations, and pain. Discussion between the orthopedic surgeon and rehabilitation team occurred prior to the start of formal post-operative rehabilitation. While there is no clear consensus in the literature to support a specific rehabilitation protocol for the Latarjet procedure in an basketball player (overhead athlete), general postoperative principles ensuring early pain control, stability, mobility, and strength adequate to support return to the subject’s desired level of activity can help guide the process.15 Early postoperative considerations include allowing for osseous fixation of the coracoid process while maintaining and gradually progressing shoulder range of motion. The available evidence and guidelines are less clear for the later stages of rehabilitation regarding return to sport.15 The proposed rehabilitation plan consisted of four phases: protective (Phase 1), intermediate (Phase 2), advanced strengthening (Phase 3) and return to activity (Phase 4) which are outlined in the protocol, found in Appendix A. The subject completed an episode of physical therapy care that included two visits per week in addition to a home exercise program to be performed independently.
OUTCOME MEASURES
RANGE OF MOTION
The subject at initial evaluation presented with 90 degrees of passive shoulder (glenohumeral) flexion and 20 degrees of shoulder external rotation with the shoulder placed in 0 degrees of abduction. Shoulder abduction and internal rotation range of motion were held in the early protective phase of rehabilitation to protect surgical repair, therefore shoulder external rotation and internal rotation with the shoulder in abduction were not obtained at the initial evaluation.
PERFORMANCE MEASURES
Isokinetic shoulder external rotation and internal rotation strength testing were measured at 60 deg/sec using the Biodex System 3 dynamometer with the shoulder starting in the scapular plane in neutral rotation. The shoulder was tested through full available internal and external rotation set by the Biodex system. A limb symmetry index (LSI) of 95%-100% for external rotation strength and 100%-110% for internal rotation strength assessed by isokinetic testing or hand-held dynamometry was established as the satisfactory target for overhead athletes, specifically throwers.16 Other key parameters established with isokinetic dynamometer strength testing includes ER/IR ratio of 72-76%, ER torque to body weight ratio of 18-23%, and IR torque to body weight ratio of 26-32% in this overhead athlete population.16 Additionally, an external rotation endurance test with the shoulder at 90 degrees abduction (Figure 1), a shot put test to measure power output (Figure 2), and an upper limb rotation test (ULRT) (Figure 3) were used to assess components of performance and return to sport readiness.
For the external rotation endurance test, participants were instructed to stand up straight with their back against a wall. The involved arm was placed in a 90-degree forward flexion holding a 1-m long Theraband fixed at shoulder height. For standardization purposes, the subject in this study was asked to pull a red Theraband (1.7kg) on the basis of sex. This was determined from a previous study in which it was reported that 1.4-1.6kg of external load was used to fatigue the rotator cuff in females while 2.0-2.5kg of external load was used to fatigue the rotator cuff in males. Participants were asked to pull the Theraband from the starting position of 90-degree forward flexion to 90-degree external rotation and 90 abduction (90/90 position) at a cadence given by a metronome. Repetitions were performed until the participant was fatigued indicated by one of the following conditions: The inability to keep the pace or reach the ending position after 2 verbal cues or verbal report of the inability to continue. The cadence increased every 20 seconds starting from 60 beats per minute (bpm) to 150 bpm by increments of 30 bpm. At 150 bpm, the cadence remained the same until the end of the test.17 It is reported in the literature that the absolute reliability for this performance test is clinically acceptable with the relative reliability specific to the cited literature ranging from high to very high (ICC:0.78-0.93) and the standard error of measurement varying from 10.7s to 16.45s.17

The single arm seated shot-put test is conducted utilizing a 6-lb ball, while the participant is seated with their back against the wall. The participant is then required to push the ball from shoulder level maintaining contact with the wall behind them, minimizing the use of the legs and trunk. After two practice trials, the distances of three maximal effort trials are then recorded for a successful test session, with an average distance being used as the final test value. Literature has reported good test-retest reliability for the non-dominant (ICC:0.97) and dominant arm (ICC: 0.99) in young male and female subjects.18 Normative data was established in the literature for select populations including young males and females (average age 24.3 years).18 The mean limb-symmetry index was found to exceed 100% in male (108.7%) and female (104.4%) athletes in the following collegiate sports, men’s football, men’s baseball, women’s basketball, women’s lacrosse, women’s softball, and women’s volleyball.18

The ULRT is a physical performance test including a combination of open-kinetic chain, closed-kinetic chain and trunk rotation as well as 90°/90° shoulder position. The test involves the subject starting in a forward plank position on forearms and toes adjacent to a wall. The subject then rotates through the trunk pivoting on the involved upper limb while tapping the contralateral limb to the wall while it remains perpendicular to the floor. The ULRT showed moderate correlations with the closed-kinetic chain upper extremity stability test and seated medicine ball throw test. High relative reliability values (ICC: 0.76-0.78) for the ULRT are reported in the literature for dominant and non-dominant arms.19

INTERVENTIONS
Phase 1 - Protective Phase (Weeks 0-6)
The goals of this rehabilitation phase include protection of the surgical site, pain control, facilitation of tissue healing, and achieving and maintaining early range of motion (ROM) within postoperative limits. Educating the subject on the importance of adherence to sling immobilization for six weeks, as well as postoperative range of motion and weight-bearing precautions is imperative to protect the tissue repair and to allow for osseous fixation. During this phase, passive shoulder ROM was initiated to maintain the mobility of the glenohumeral joint. Elbow and wrist active ROM exercises were also prescribed to limit post-operative stiffness, atrophy, and to improve blood flow in adjacent, uninvolved joints. Active elbow ROM and loaded elbow flexion and supination is contraindicated in this phase due to the involvement of the biceps brachii and to avoid excessive forces on the coracoid process fixation to the glenoid. Passive external rotation of the shoulder was limited to 30 degrees in the scapular plane for the first three weeks due to the subscapularis muscle split. Passive shoulder external rotation was then progressed to tolerance in the scapular plane during weeks 4 through 6. Passive shoulder flexion was performed to tolerance progressing to full ROM by week 6.
In addition to ROM exercises, scapular exercises including protraction, retraction, elevation, and depression were given early in the first week to facilitate foundational neuromuscular control. Submaximal isometrics for shoulder external rotation, internal rotation, abduction, extension, and adduction were initiated in week 2. These exercises were performed to pain-free tolerance.
Advanced neuromuscular control exercises were introduced in week 3 including supine scapular protraction, short-lever rhythmic stabilization in supine, light banded rows, and light banded shoulder external rotation to available range of motion. Week 4 consisted of unweighted prone scapular retraction with horizontal abduction, unweighted side-lying shoulder external rotation, side-lying shoulder flexion, supine PNF D2 flexion, unweighted shoulder flexion in the scapular plane, serratus wall slides, banded internal rotation, and ball circles on the wall for progressed rhythmic stabilization. These exercises were progressed for the next two weeks by adding load and/or volume as indicated and as tolerated by the subject.
The subject’s pain was well-controlled during the first six weeks, and she demonstrated the ability to achieve the goals set in this phase without an increase in pain. It was determined at this point that the subject was ready to advance to Phase II of the rehabilitation program.
Phase 2 - Intermediate Phase (Weeks 7-11)
The goals of this phase of rehabilitation are to progress neuromuscular control of the shoulder complex, maintain full passive range of motion while initiating, progressing, and normalizing active range of motion, and improving muscular endurance. Isotonic exercises were prescribed early on with low load, high repetitions and decreased rest times. Repetitions in reserve (RIR) were utilized as a method of assessing exertion levels and for dosing and progressing exercises. Progressive resistance exercises (PRE) were prescribed in sets of 2-3 with repetitions in the 12-15 range and targeted scapular stabilizers with row variations, prone flexion in the scapular plane, prone horizontal abduction, and loaded side-lying external rotation as this demonstrated the highest rotator cuff activation when compared to other shoulder exercises.20 In addition to these open-chain scapular and rotator cuff strengthening exercises, closed-kinetic chain exercises were initiated at week 8 to advance neuromuscular control, increase co-activation of shoulder musculature, and address joint proprioception.21 The closed-chain exercises were advanced through a progression that started with weight bearing holds first on a wall, then plinth, to the floor in a modified tall plank position, and finally to a full tall plank position on the floor. Once the subject completed this progression without compensatory strategies and shoulder discomfort, the progression was repeated from the wall to the floor while adding in weight shifts and shoulder taps for advanced single-arm weight bearing activities.
The rehabilitation sessions between weeks 8 and 11 continued to progress the load, volume, intensity, and duration of progressive resistance exercises (PREs) challenging muscular strength, endurance, and control. The load and volume progressed to 3-5 sets of 8-12 repetitions per exercise. These parameters were utilized to drive desired muscular and strength adaptations.21 The subject returned to non-contact, on-court conditioning drills with the strength and conditioning staff at 9.5 weeks post-surgery while continuing physical therapy sessions two days per week. Early basketball specific drills consisted of ball handling drills, seated initially progressing to standing, keeping all activities chest level and below. All activities were kept to below shoulder level. Early, light plyometric exercises were initiated at week ten in addition to PREs including two-hand wall dribbles for time to address endurance with dynamic activity and light chest passes to re-introduce sport-specific activity.
To reduce stress on the glenohumeral joint, treatment addressed the entire kinetic chain, including thoracic spine mobility and trunk endurance to facilitate improved movement quality. The subject demonstrated tolerance for all PREs without exhibiting compensatory patterns. PROM and AROM were maintained throughout the duration of this phase. The subject showed a readiness to progress to the next phase of the rehabilitation program.
Phase 3 - Advanced Strengthening Phase (Weeks 12-15)
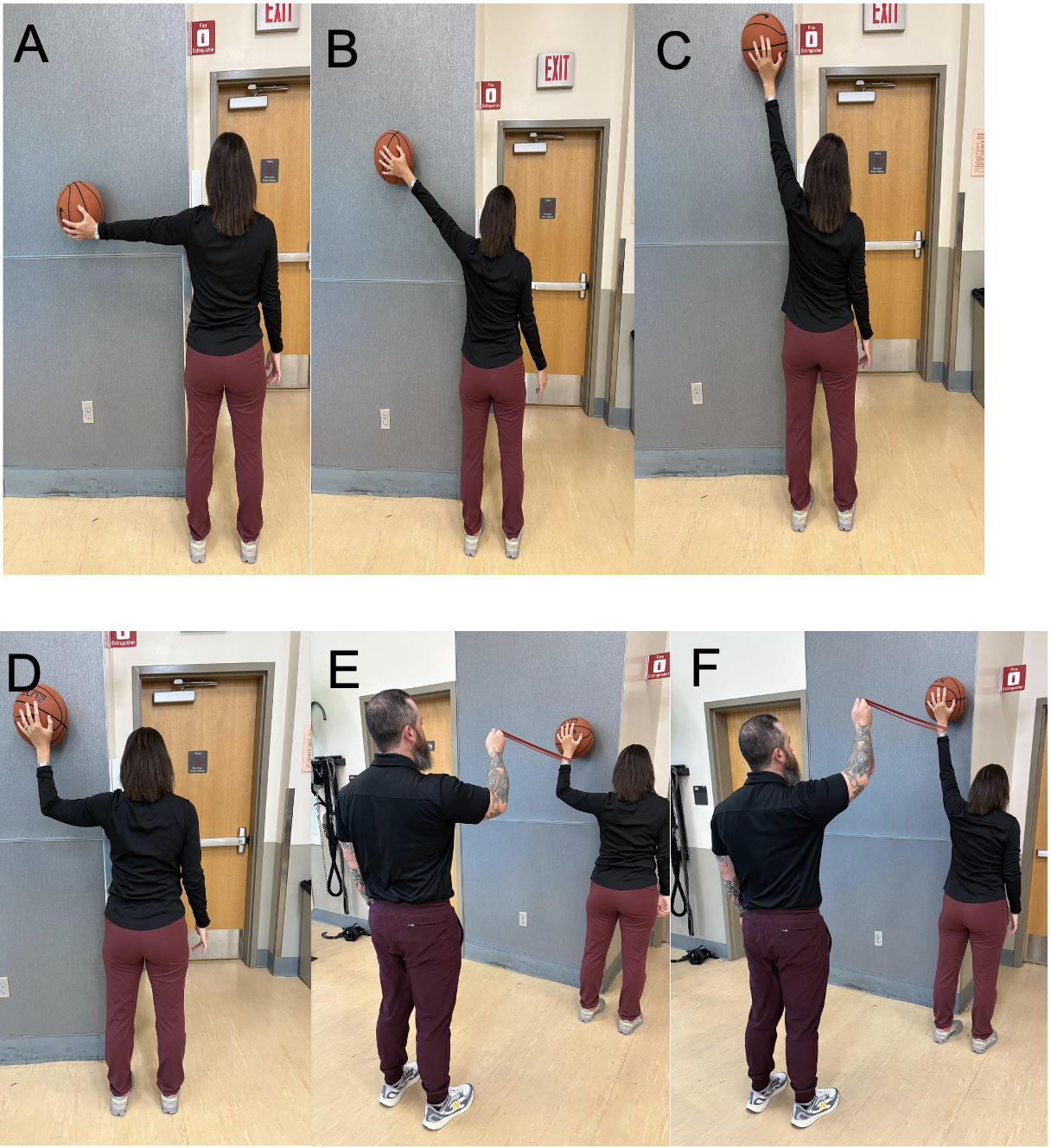
The goal of this rehabilitation phase was to normalize strength, motor control, endurance, and power to prepare the subject for basketball activities. PREs continued and progressed in load, intensity, and volume. Global upper extremity strengthening was initiated and integrated into the rehabilitation program in addition to continued isolated shoulder strengthening including narrow grip push-ups, partial range bench press, horizontal and vertical rows, and overhead press. Additionally, plyometric exercises were progressed to single arm wall dribbles at various arm slots for time to improve endurance and stability at end range. The dribbles were performed at 90, 120, and 160 degrees of shoulder abduction with an extended elbow in addition to 90 degrees of abduction with the elbow flexed to 90 degrees. In this case, the various angles were utilized, as this subject specifically experienced shoulder instability during the late cocking phase of a single-arm, overhead basketball pass with the shoulder in abduction and external rotation. (Figure 4 A-F)

Plyometric exercises were then progressed to higher intensities, decreased volume, with increased rest time to improve power output. Plyometric exercises were also progressed to include a multiplanar approach including the sagittal, frontal, and transverse planes to prepare for sporting activity. Examples include two-handed medicine ball catch and throws at chest level, overhead medicine ball slams, rotational medicine ball throws and catches, and progressive plyometric pushups starting from the wall and progressing to the floor.
The subject continued non-contact, on-court activities with the strength and conditioning staff to improve overall conditioning levels prior to clearance for return to practice. It was during this phase that the subject also began an on-court shooting progression under the supervision of the strength and conditioning staff. Initial shooting progression began three feet from the basket with five spots marked and set up around the basket in an arc. The athlete was instructed to take all shots with “form shooting” (no jump shots). Jump shots were initiated at 16 weeks and typical Division 1 women’s basketball players can “form shoot” to about 12-15 feet without jumping. The athlete was instructed to take 5-10 shots at each spot and move to the next spot. Their instructions were to make 50 successful baskets per session (successful baskets not total shots). The subject was instructed to move back three feet every week working their way to the free throw line.
Phase 4 - Return to Activity Phase (Weeks 16-24)
The goal of this last phase of rehabilitation was to facilitate a gradual return to full participation in basketball-related activities and to maintain strength and ROM gains achieved over the course of the rehabilitation program. The interventions during this phase continued to address the foundational pieces of strength, ROM, neuromuscular control, while maintaining flexibility and monitoring shoulder soreness and discomfort as the subject’s participation in non-contact practices and weight training program with the strength and conditioning staff increased. The subject was allowed to initiate jump shots and non-contact basketball drills. Initially, all drills began at half court and then progressed to full court. At 20 weeks, the subject progressed to half court, full contact 1v 1 drills, then 2 v 2 drills at 21 weeks, 3 v 3 drills at 22 weeks, 4 v 4 drills at 23 weeks, and finally 5 v 5 drills at 24 weeks. The subject was progressed to a full court, scrimmage at five months post-operative. The subject underwent strength and performance testing at 16 weeks post-surgery. A limb symmetry index (LSI) of 95%-100% for external rotation strength and 100%-110% for internal rotation strength was established as the satisfactory target.16 Additionally, >90% LSI during endurance, power, and closed-chain stability test was established as the satisfactory target. The subject satisfied all strength and performance criteria at return-to-sport testing (Table 2) and received physician clearance to return to all basketball-related activities without limitations. The subject continued participating in physical therapy after clearance to return to sport for maintenance of ROM and strength while also participating in practices and team lifting sessions.
OUTCOMES/RESULTS
The subject completed 30 sessions of physical therapy over 16 weeks. Subject-reported outcomes were utilized as one of the tools to assess subject progress over the course of the post-operative rehabilitation program (Table 1). At discharge, the subject exhibited an overall improvement in glenohumeral flexion of 90 degrees to 167 degrees and external rotation at 0 degrees of abduction of 20 degrees to 70 degrees.
The subject’s functional recovery through rehabilitation is reported in Tables 2 and 3. The tables highlight which outcomes display change greater than clinical important values. At the end of Phase 4 the subject’s score on the PSS, QuickDash, and SANE improved 62.5%, 50%, and 93% respectively. The improvement in the subject’s PSS score from the initial post-operative evaluation to the time of discharge exceeded the MCID of 11.4 points indicating significant improvement in the subject’s satisfaction with shoulder function. The improvement in the subject’s SANE score from the initial post-operative evaluation to the time of discharge exceeded the MCID of 15% and indicates that the subject had a perception of being 93% of her pre-injury and pre-surgical baseline. The improvement in the subject’s QuickDASH score from the initial post-operative evaluation to the time of discharge exceeded the MCID of 15.91 points exhibiting significant improvement in the subject’s reported disability of the upper limb.12 Lastly, the OSPRO-YF improved from 10 yellow flags at initial postoperative evaluation to two yellow flags at the time of discharge. The OSPRO-YF was collected at the nine-month follow-up and decreased to one yellow flag. PSS score increased 58 points (minimal clinically important difference [MCID] = 11.4 points), QuickDASH score decreased 43.75 points ((MCID) = 15.91 points), SANE score increased by 52.9% (MCID = 18%), and OSPRO-YF count decreased from 10 yellow flags to 1.9–12
Strength and performance testing was completed at the 16-week post-op to guide return to play decision-making and again at nine months post-op (Table 3). The subject at 16 weeks post-op demonstrated a 10.5% peak torque to bodyweight ratio for shoulder external rotation on the surgical shoulder, 12.6% internal rotation peak torque to bodyweight on the surgical shoulder, and an external rotation to internal rotation strength ratio of 83.5%. The three additional tests in the battery of performance tests assessed and compared bilateral rotator cuff endurance, closed-chain upper extremity stability, and upper extremity power. The subject’s surgical limb outperformed her non-surgical limb in strength, endurance, and closed chain stability tests while exhibiting a 2.3% deficit in the seated single arm shot put test.
DISCUSSION
The purpose of this case report was to outline a rehabilitation and return to sport progression for a female, collegiate overhead athlete who underwent a Latarjet procedure following a failed anterior Bankart repair. Current literature largely omits gender information, primarily includes male cohorts, or does not specifically analyze gender-specific complication rates.22,23 This case report provides an example postoperative rehabilitation program that addressed the athlete’s sport-specific demands prior to returning to basketball. In this case, the female athlete favorably responded to the open Latarjet procedure and successfully completed a formal course of rehabilitation to return to sport at her prior level of function.
In reviewing range of motion measurements reported in a recent systematic review for shoulder flexion, abduction, external and internal rotation in subjects having undergone the Latarjet stabilization procedure, it was determined that this subject demonstrated adequate and functional shoulder range of motion at discharge.24 Additionally, the subject demonstrated external rotation and internal rotation strength limb symmetry index of 106.8% and 94.1% respectively. Within the current body of literature, there appears to be a lack of consensus on the relevant criteria and the return-to-sport standards in regard to strength and performance measures.24 The subject displayed a limb symmetry index of greater than 90% for all strength and performance tests and measures indicating readiness to return to practice and sport.16,24 The subject met MCID values for all subject-reported outcome measures including the PSS, QuickDASH, SANE, and OSPRO-YF when comparing scores and values at initial evaluation to discharge.
The Latarjet procedure which is described as having recurrent instability rates of as low as 3%, in this case, served as an effective procedure for addressing recurrent shoulder instability or shoulder instability involving significant bone loss, in a high-level female, overhead athlete. An evaluation of post-operative and return to sport outcomes following the Latarjet procedure was performed in contact athletes, overhead athletes, and athletes with failed Bankart repair and <20% glenoid bone loss.5 Of the athletes included in the study, 94% return to sports and 84% returned to sports at prior level of function.5 The total reported complication rate reported at the 53-month follow up was 10.8% with a revision rate reported at 1.5%.5
This case describes the unique rehabilitation considerations including tissue healing time frames, soft tissue involvement, and criteria for progression that come with the Latarjet procedure in an overhead athlete. The rehabilitation program for this athlete was designed with consideration for both the unique demands of collegiate basketball and the biomechanical implications of the Latarjet procedure. Compared to Bankart rehabilitation, progression was delayed for passive abduction and external rotation as well as progressive resistance exercise to ensure graft incorporation while minimizing shear stress on the coracoid transfer. Bankart protocols may allow more aggressive range of motion restoration, whereas external rotation in the scapular plane was limited in this subject to thirty degrees for the first three weeks and then began range of motion as tolerated of external rotation in abduction at six weeks for the aforementioned reasons. Progressive resistance strengthening exercises in Bankart repairs can typically begin around four weeks, whereas they were postponed until six weeks fin this case, after a routine follow up radiograph to ensure graft integration. The athlete returned to sport at five months post-operatively, which is generally earlier than the typical return-to-play timeline following a Bankart repair, which often ranges from six to nine months depending on the level of sport, shoulder stability, and strength recovery. The earlier return in this case likely reflects the enhanced mechanical stability provided by the Latarjet procedure, particularly the bony augmentation and dynamic sling effect of the transferred conjoint tendon. There remains a need for high quality evidence and a consensus return to sport testing battery for overhead athletes, particularly following surgical intervention. This is crucial to ensure that an athlete who has undergone this procedure is physically and psychologically prepared to meet and perform the demands of their specific sport safely while mitigating re-injury risk and improving long-term outcomes.
CONCLUSION
This case report provides an example of an open Latarjet rehabilitation protocol used to facilitate the return to sport process for a female NCAA Division I basketball athlete. The purpose of this case report was to provide additional evidence to assist physical therapists, athletic trainers, and surgeons with the appropriate rehabilitation guidelines and criteria for subjects undergoing an open Latarjet procedure. The subject reported an increase in upper extremity function as noted subjectively and by clinically meaningful improvements in patient reported outcomes and was able to demonstrate a limb symmetry index of greater than 90% for all strength and performance tests and measures. The subject was able to resume and return to sport at 16 weeks. There is an opportunity for future research studies to explore Latarjet outcomes in female subjects both in the short and long-term as current available literature does not focus on female athletes.
Conflict of interest statement
This case report was completed during the University of Florida Health Sports Residency approved by the American Board of Physical Therapy Specialties (ABPTS). The authors report no conflicts of interest.
Subject Consent
Subjects were informed prior to treatment that data concerning the case would be submitted for publication.
Acknowledgements
Marisa Hawkins, DPT, PT, SCS, OCS, Maria Rademacher, DPT, PT, SCS, and Joe William Cavazos - Department of Rehabilitation, University of Florida Health