INTRODUCTION
Anterior cruciate ligament (ACL) injuries constitute a significant portion of major knee joint injuries sustained by young, active individuals. Post-traumatic muscular dysfunction is characteristically observed following ACLR1 and is associated with poor outcomes,2 making the recovery of muscle function a primary clinical concern. Persistent hamstrings dysfunction is predominant in patients who undergo ACLR with hamstrings tendon (HT) autograft,3,4 which can take years to recover.5,6 Compounding this scenario, evidence-based treatment approaches to guide recovery of the hamstrings after this procedure are sparse, as the scientific literature has historically focused on the quadriceps,7 creating a substantial knowledge gap.
Hamstrings atrophy or lesser muscle volume has been widely reported following ACLR with HT.3–6 Reductions in total hamstrings volume appear to be driven by large magnitude deficits in the semitendinosus,4 which rapidly declines after ACLR (>30% volume loss pre-to-post-surgery)8 due to graft harvesting. Failure to restore hamstrings volume, particularly the semitendinosus, likely contributes to the persistence of multiplanar strength deficits, which threaten dynamic knee stability and promote high-risk patterns of joint loading.9 From a neuroanatomical perspective, the ACL-hamstrings reflex arc further contributes to knee stability by allowing changes in joint loading to reflexively activate the hamstrings, yet the presence of muscle weakness and volume loss may impede their ability to do so effectively.
Neither traditional rehabilitation approaches nor the resumption of physical activity appear to fully resolve muscle atrophy, as volumetric deficits have been observed beyond five10 and ten5 years following ACLR with HT with no discernable differences based on time from surgery noted in a recent meta-analyses.3,4 Compelling evidence supports the ability of eccentric exercise to enhance both peripheral and neural aspects of muscle function to a greater extent than concentric exercise,11 which appears necessary to overcome post-traumatic atrophy.12 The Nordic hamstring exercise (NHE) is a challenging, but clinically accessible form of eccentric exercise commonly used in team-based sports as a means to decrease risk for hamstring strain injuries.13 While NHE protocols have yielded improvements in hamstrings size (thickness and volume) in uninjured individuals,14,15 little is known about its use as an intervention after ACLR. Only one recent study16 has incorporated NHE with traditional rehabilitation during post-operative weeks 7-24. Although the parameters of exercise employed in that study are unclear, less asymmetry in thigh circumference was observed between limbs compared to a usual care group, suggesting the possibility of improvement in muscle size. The NHE is reported to preferentially recruit the semitendinosus,17 particularly the distal musculature,18 making it well suited for individuals who undergo ACLR with HT given that variable semitendinosus tendon regeneration and restoration of muscle volume is observed in this population.6
When considering individuals recovering from ACLR, the NHE has been largely used to evaluate hamstrings function (i.e., strength and activation).19–21 The lack of investigations using it as a defined intervention limit the ability to develop evidence-based treatment guidelines for hamstrings recovery in this population. Therefore, the primary aim of this study was to describe changes in hamstrings volumes following an isolated NHE protocol among individuals with a history of ACLR via HT. The secondary aim was to compare hamstrings volumes to historical data of a demographically similar cohort to appreciate the nature of baseline impairments. For ease of contextualizing these findings with previous investigations, the final aim was to describe changes in eccentric strength between the first and last sessions of the NHE protocol.
MATERIALS AND METHODS
Study Design
A prospective case series design was used to investigate responses in hamstrings volumes and eccentric strength to a four-week NHE protocol. Three-dimensional muscle volumes of the total hamstrings, biceps femoris long head, biceps femoris short head, semimembranosus, and semitendinosus were quantified before and after the protocol in the ACLR limb only. Hamstrings eccentric force was quantified in the ACLR limb during the first and last session.
Participants
A convenience sample of individuals with a history of primary, unilateral ACLR with HT were recruited for this study from a larger clinical trial (registration number
NCT05738200). Individuals between the ages of 18-35 who were not participating in a formal rehabilitation program at the time of enrollment were eligible to participate. As morphological impairments are reported beyond return to activity,3,4 enrollment was limited to individuals discharged from rehabilitation to minimize the potential impact of competing exercise interventions. Those with a history of ACLR via non-hamstrings graft source, additional lower extremity surgery, lower extremity injury within six months, known osteoarthritis, concussion within six months, cardiopulmonary disorder, neurological or psychiatric disorder, implanted biomedical device, or use of medications that could alter neural excitability were excluded. The University of Toledo Biomedical Institutional Review Board approved this study and all participants provided verbal and written informed consent.
Procedures
Patient-reported Outcomes
To characterize the sample, subjective knee function and current physical activity level were quantified using the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation and Tegner Activity Scale, respectively.
Muscle Volume
Participants’ muscle volumes were assessed at a University Medical Center within one week prior to baseline and again within one week of completing the NHE protocol. Vigorous physical activity was avoided for 24 hours prior to volumetric assessment. Hamstrings volumes were obtained using a 1.5 Tesla MRI scanner (Siemens Magnetom Espree, Washington, DC) according to previously described parameters.22 Axial images were obtained from anterior superior iliac spine to tibial tuberosity. A deep convolutional neural network-based approach was used to automate the segmentation of individual muscles, as this technique has demonstrated a high degree of accuracy relative to ground truth values.22 Raw (cm3) and mass x height-normalized (cm3/kg*m) values were reported for total and individual hamstrings muscle volumes, as both metrics are reported in the literature.
Eccentric Strength and Exercise Protocol
All strength assessments and intervention sessions were completed at a university research laboratory. Moderate-to-large magnitude gains in eccentric hamstrings strength gains and morphological adaptations are reported to occur in as little as four to five weeks (8-10 NHE sessions)14,23 As such, participants were asked to complete 10 sessions of a standardized NHE protocol over a four-week duration. In brief, the protocol used in this study was adapted from prior work.13 Protocols using NHE as a means to reduce the risk of hamstring strain injuries, improve performance, or increase eccentric hamstrings strength vary considerably in terms of duration (4-17 weeks), frequency (1-3 days per week), and total volume (110-844 repetitions).24 To maximize compliance as a preliminary investigation, a truncated version of a previously described protocol that was effective in decreasing the rate of new or recurrent hamstring injuries was used. The protocol consisted of the following weekly schedule: week 1 (2 sessions, 2 sets per session, 5 repetitions per set), week 2 (2 sessions, 2 sets per session, 6 repetitions per set), week 3 (3 sessions, 3 sets per session, 6-8 repetitions per set), and week 4 (3 sessions, 3 sets per session, 8-10 repetitions per set). Therefore, this four-week, 2-3 days per week, 206 total repetition protocol reflected the lower end of exercise volume that has been described in the literature. A minimum of 24 hours was required between sessions to minimize fatigue. The feasibility of this protocol has recently been documented among a larger sample of individuals with ACLR.25
An athletic trainer (n=2) or physical therapist (n=1) trained in the protocol supervised each session using standardized instruction. The same investigator supervised a given participant through the duration of the intervention period. Participants performed the NHE on a NordBord device (VALD Performance, Charlotte, NC) and were instructed to use their hamstrings equally between limbs to resist a forward-falling motion for as long as possible (minimum of 3 seconds), while maintaining a neutral trunk/hip position.13 The supervising investigator provided verbal encouragement during each repetition to maximize effort. Immediately following each repetition, the investigator provided feedback to participants based on their technique to correct any deviations from their standardized instructions (e.g., too much trunk/hip flexion, too fast). The investigator visualized force tracings from each limb on a tablet in real-time and provided additional feedback based on the force distribution between limbs to promote symmetry as they deemed necessary (e.g., increase force on left leg). Peak eccentric force was obtained at the end of each set of exercise completed. The average peak force (N) was quantified for the first and last exercise sessions. Torque was derived from force data using the knee position (representative of external moment arm) on the NordBord device and mass-normalized torque (Nm/kg) was reported. The number of sessions, sets, and repetitions completed were recorded for descriptive purposes.
Perception of Exercise Protocol
Participants rated their level of exertion at the end of each exercise session using the Borg Rating of Perceived Exertion (RPE) scale (6-20). The magnitude and location of pain or discomfort to either limb associated with the exercise performed was assessed using a 10 cm visual analog scale (VAS) and body diagram. To understand participants’ intrinsic motivation and perception of the protocol, their interest or enjoyment in performing the exercise and their perception of how valuable or useful it was to their leg function was assessed using the Intrinsic Motivation Inventory with modified subscales of interest/enjoyment and value/usefulness (7-49)—higher values indicated greater perceived enjoyment and value. Lastly, participants reported the degree of change in their knee condition upon completion of the protocol using a 15-point global rating of change (GROC) scale.
Statistical Analyses
As this was a descriptive case series, a formal power analysis was not conducted. The changes in raw muscle volumes and average peak force were quantified as percentage change scores and reported with 95% confidence intervals (CIs). Cohen’s d effect sizes with 95% CIs were also used to quantify the magnitude of change in each outcome and interpreted as large (≥ 0.8), moderate (0.5-0.79), small (0.3-0.49), or trivial (< 0.3). Normalized muscle volumes were secondarily compared to a previously reported database26 of uninjured males and females using z scores. In this way, muscles were classified as extremely larger (z ≥ 3 SD), moderately larger (3 > z ≥ 2 SD), slightly larger (2 > z ≥ 1 SD), normal (1 > z > -1 SD), slightly smaller (-1 ≥ z > -2 SD), moderately smaller (-2 ≥ z > -3 SD), or extremely smaller (z ≤ -3 SD) than normal before and after the intervention. Summary statistics were used to report patient-reported outcomes and those related to participants’ perception of the exercise protocol. An exploratory correlational analysis was conducted to evaluate the potential of confounders (age, time from surgery, activity level, subjective knee function, motivation [interest/enjoyment, value/usefulness], baseline strength, and baseline muscle volume) to the magnitude of percentage change in total hamstrings volume. All analyses were performed in Microsoft Excel (v. 14.4.7).
RESULTS
Participant demographics are reported in Table 1. In total, three females and four males participated (age: 22.0 ± 2.3 years, time from surgery: 53.6 ± 29.5 months). The database26 of uninjured individuals referenced for normative data consisted of eight females and 16 males (age: 25.5 ± 11.1 years, height: 1.7 ± 0.1 m, mass: 71.8 ± 14.6 kg).
Muscle volumes
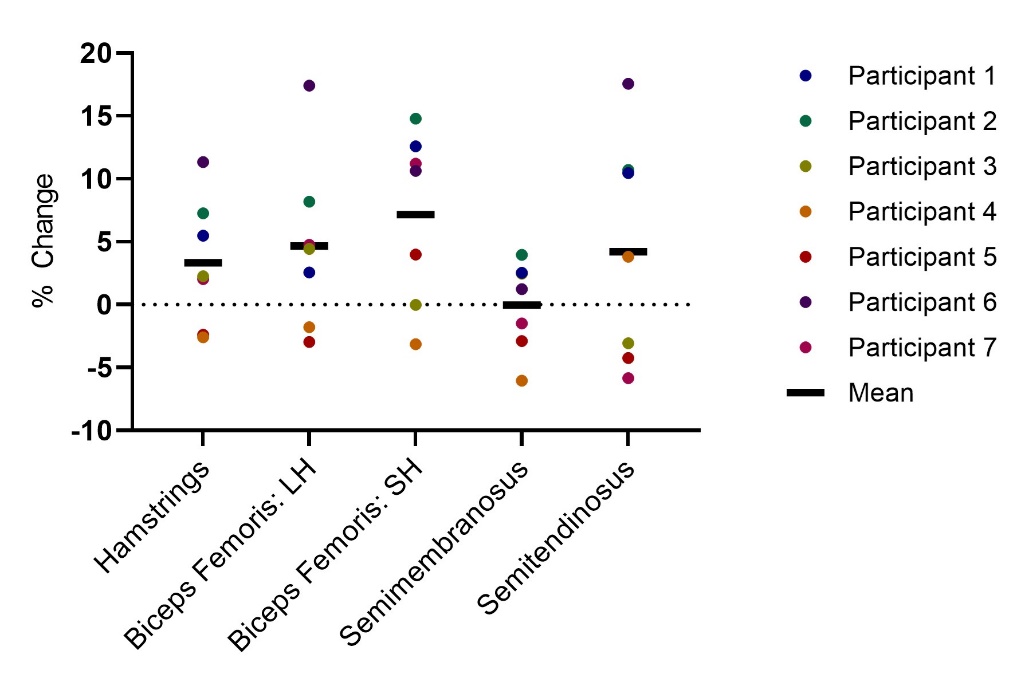
On average, muscle volumes were assessed 3.3 days (range: 1-7) after the final NHE session. Changes in muscle volumes ranged from -6.0 to 17.6% across all participants and muscles (Table 2, Figure 1). At the individual level, in a simple majority of the participants, increased volumes were observed for the total hamstrings (n=5; participants 1, 2, 3, 6, 7), biceps femoris long head (n=5; participants 1, 2, 3, 6, 7), biceps femoris short head (n=5; participants 1, 2, 5, 6, 7), semimembranosus (n=4: 1, 2, 3, 6), and semitendinosus (n=4: 1, 2, 4, 6). On average, trivial-to-moderate magnitude increases in muscle volumes were observed for the total hamstrings (Δ 3.3% [-0.4, 7.1%], d = 0.27 [-0.78, 1.33]), biceps femoris long head (Δ 4.7% [-0.4, 9.7%], d = 0.32 [-0.73, 1.38]), biceps femoris short head (Δ 7.2% [2.1, 12.2%], d = 0.53 [-0.53, 1.60]), and semitendinosus (Δ 4.7% [-2.5, 10.9%], d = 0.12 [-0.93, 1.17]). Semimembranosus volume did not change on average (Δ 0.0% [-2.7, 2.6%], d = 0.01 [-1.03, 1.06]).

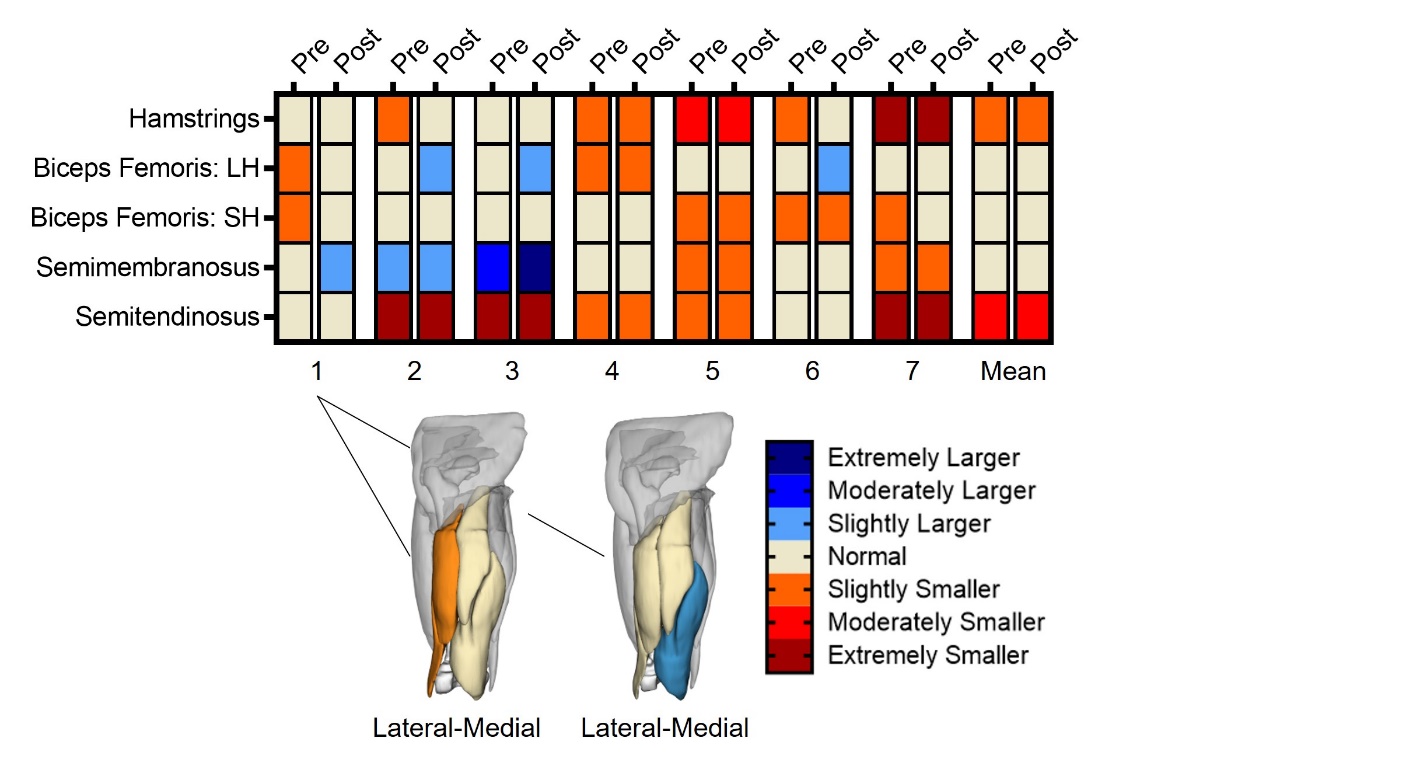
Each participant demonstrated smaller than normal muscle volumes before the intervention (Figure 2). However, a consistent pattern was not observed at baseline or in response to the NHE protocol. At the individual level, improvements in z score classifications were observed for the total hamstrings (n=2; participants 2, 6), biceps femoris long head (n=4; participants 1, 2, 3, 6), biceps femoris short head (n=2; participants 1, 7), and semimembranosus (n=1; participant 1), but not semitendinosus (n=0). On average, the total hamstrings remained slightly smaller and the semitendinosus remained moderately smaller than normal after the intervention.

Eccentric strength
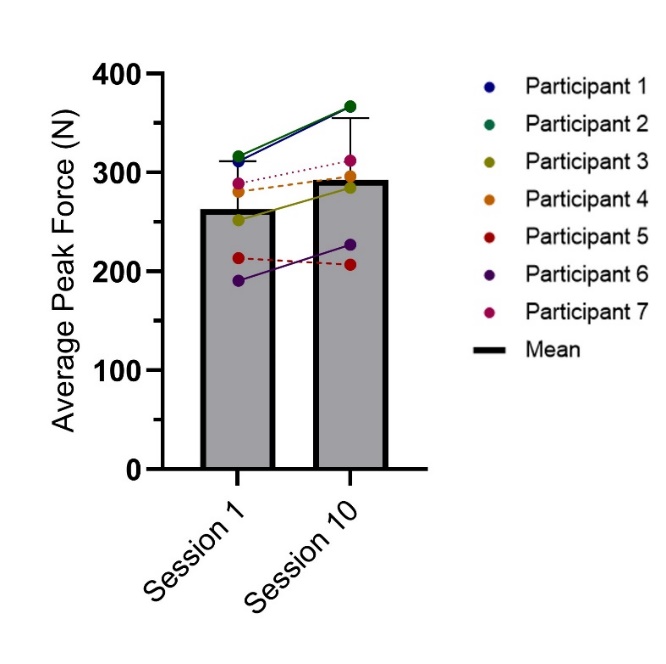
Changes in average peak eccentric force ranged from -3.2 to 19.4% across all participants (Table 3, Figure 3). At the individual level, the majority of participants (6 of 7; participants 1, 2, 3, 4, 6, 7) demonstrated an increase in strength from Session 1 to Session 10. On average, a moderate magnitude increase in strength was observed (Δ 11.0% [5.1, 17.0%], d = 0.53 [-0.53, 1.60]).

Perception of exercise protocol
All participants completed the intervention as intended (10 sessions, 26 sets, 206 repetitions). Session RPE is plotted relative to exercise volume through the duration of the intervention for descriptive purposes (Appendix 1). Participants reported a median session RPE of 11.6 (interquartile range: 10.8-14.9), which ranged from 6 (no exertion) to 17 (very hard). Six of 7 participants reported discomfort associated with the intervention at least once during the intervention period, with an average rating of 0.4 cm (range: 0-2.5 cm) across all sessions. Discomfort was largely isolated to the hamstrings (83.3%), with several reports of calf (6.7%), low back (6.7%), and pes anserine (3.3%) discomfort. Participants’ interest or enjoyment (median: 28, interquartile range: 9-34.5) in performing the exercise and their perception of its value (median: 40, interquartile range: 7-48) to their leg function was relatively high. However, a consistent bimodal response was observed for each measure of intrinsic motivation (low: n=3, range: 7-9; high: n=4, range: 28-49). On average, self-reported knee condition improved by +4.3 (GROC range: +2-6).
DISCUSSION
The primary aim of this study was to describe presumable changes in hamstrings muscle volumes following a four-week isolated NHE protocol among a sample of individuals who had undergone ACLR with HT. Evidence of trivial-to-moderate increases in muscle volumes was observed, which align with reported deficits in this population.3,4 However, variable responses (-6.0 to 17.6%) to exercise indicate that some individuals may have experienced a greater benefit than others, suggesting a need to consider the individualized needs of patients. At the group level, total hamstrings and semitendinosus volumes remained smaller than normal following NHE, yet inconsistent volumetric profiles at baseline may further suggest a need for individualized exercise progression. Despite showing evidence of a moderate increase in eccentric strength, the collective volumetric response was more variable, which may reflect the nature of the exercise parameters.
Each participant in the sample presented with evidence of atrophy to at least one muscle at baseline based on a historical comparison to previously collected data among a demographically similar cohort of uninjured individuals.26 However, the presumptive volumetric response to NHE was bimodal, in which 4 to 5 participants (57.1-71.4% of sample) experienced an increase in hamstrings volumes (Figure 1). Researchers from a recent study16 integrated NHE into post-operative rehabilitation beginning at week 7 after ACLR, but the parameters of exercise intervention were not clear, leaving it difficult to inform clinical management. Regardless, those authors observed less asymmetry in thigh circumference between limbs at six months compared to a usual care group compared to the current results. Circumferential data may suggest that hypertrophy occurred, but do not offer insight on individual muscle adaptations. In contrast, large magnitude increases in semitendinosus (21%), biceps femoris short head (8%), and biceps femoris long head (5%) volumes have been reported among a sample of 10 recreationally active males following 10 weeks of progressive NHE relative to a control condition. Importantly, that study demonstrated consistency in measured muscle volumes (Δ within ± 1%) during the 10-week intervention period.14 Although the largest individual level changes were observed in the semitendinosus (17%), the biceps femoris short (7%) and long (5%) heads demonstrated the greatest increases at the group level.
Preferential semitendinosus activation has been reported during the NHE,17 yet the current findings suggest more consistent improvements in the lateral hamstrings. While anecdotal, participants often deviated from a neutral to an externally rotated foot position, which could have mechanically tensioned and activated the lateral hamstrings to a greater extent than the medial hamstrings,27 yet this has not been consistently reported to affect muscle activation. It may also be possible that the biceps femoris compensated for relative semitendinosus deficiency,10 as this neuromuscular and volumetric pattern has been reported in patients after ACLR with HT.6,28
While the majority of participants in this case series demonstrated greater muscle volumes following NHE, 2 to 3 participants (28.6-42.9% of sample) either did not change or experienced a decrease in volume (Figure 1). Several investigations have reported no change in the biceps femoris long head thickness of uninjured cohorts following four weeks (8 sessions)23 of isolated NHE or six weeks (12 sessions)29 of modified NHE combined with a unilateral, hip-dominant exercise. In this case series, participants 4 and 5 were the only to experience a net loss in total hamstrings volume. However, these participants differed in terms of their sex (male vs. female), time from surgery (65 vs. 5 months), and their interest in (34 vs. 7) and perceived value of (47 vs. 7) NHE, making it difficult to attribute their lack of response to the program itself versus these factors. Given that eight (16 sessions)15 to 10 weeks (20 sessions)14 of progressive NHE with or without the use of external loading is reported to increase hamstrings thickness and volume, it is possible that a longer duration and/or higher exercise intensity than used in the current protocol would yield more consistent improvements.
A moderate magnitude increase in peak average eccentric force of 11% was observed from the first to last NHE session completed. A recent meta-analysis24 demonstrated small-to-large magnitude improvements in peak eccentric force or torque following four, five, six, and 10 weeks of NHE in recreationally active individuals. Minimal detectable change (MDC) values for eccentric force are estimated at 27-29 N,30 suggesting that 4 of 7 (57%) participants in the current study experienced a true improvement in strength (Δ range: 33-56 N). Participant 7 fell close to the MDC (Δ: 23 N) suggesting a limited response to exercise, whereas participants 4 (Δ: 16 N) and 5 (Δ: -7 N) did not appear to demonstrate a strength response.
Previous investigations23,29 have reported improvements in strength with changes to muscle architecture following four to six weeks of NHE in the absence of changes to muscle size. The current data findings appear to support this by showing considerably larger changes in strength (Δ mean: 11%) relative to total hamstrings volume (Δ mean: 3%). However, the fact that a portion of the sample experienced both strength and volumetric gains in only four weeks’ time is encouraging. Considering best practice guidelines for hypertrophy-oriented resistance training, the use of external loading to increase exercise intensity over a longer duration (≥ 6-8 weeks) may be warranted to enhance gains in both muscle strength and size.31 Although higher exercise intensities (≥60% 1 repetition maximum) are recommended for resistance training, hypertrophy is possible at lower intensities (30-60% 1 repetition maximum) provided a greater volume of exercise is performed.31 This suggests that employing a repetition to fatigue strategy may be useful for lower intensity exercises, or those difficult to quantify, such as the NHE.
The NHE protocol used in the current study was viewed favorably by four participants and resulted in clinically meaningful improvements (minimal clinically important difference ≥ +332) in perceived knee condition for all but one. However, three participants reported low ratings of both enjoyment and value. Poor perceptions of isolated NHE have been previously reported among athletic cohorts32 and may suggest that including it as a component of a more robust (e.g., multimodal knee- and hip dominant exercises) program could positively influence participant buy-in, which becomes increasingly important for longer duration trials. It is possible that relatively moderate ratings of perceived exertion and minimal exercise-related discomfort contributed to the perfect adherence observed, despite mixed perceptions. Interestingly, session RPE did not appear to increase with the stepwise increase in exercise volume (Appendix 1), which may suggest this group of subjects was not sufficiently challenged at the group level. While a condensed, yet standardized, protocol was adopted based on prior investigations using NHE to reduce injury risk, individualizing exercise progression via session RPE, performance, or force-based metrics has the potential to improve the consistency of outcomes and perceptions of exercise value.
Limitations and Future Directions
The current findings must be considered in the context of several limitations. Although a prospective case series design was used, the lack of a true control group inherently limits inference of causality. Historical data26 were used to gain some appreciation of baseline volumetric impairments and whether muscle volumes appeared more normal following the intervention. MRI-derived muscle volumes of the hamstrings are reportedly stable (Δ within ±1%) over a 10-week period among a small sample (n=10) of recreationally active males who were instructed to continue regular exercise, but to avoid lower extremity resistance training.14 The similarity of instruction we provided in terms of avoiding additional strength training and the trivial magnitude of change in muscle volumes over a longer duration supports, but does not confirm, the notion that participants in the current study experienced true volumetric change. While a small sample limits the generalizability of findings, other studies have used small cohorts (n=6,33 n=8,34 n=10,35 n=1337) to investigate MRI-derived changes in muscle volume due to the cost and practicality of employing MRI in large-scale. The processing methods used have previously yielded low volume errors (<5%) relative to ground truth,22 with unpublished test-retest percentage differences of <2%.
Despite the accuracy of volumetric measurements, tissue composition or the region of muscle affected by exercise were not quantified. As greater hamstrings intramuscular fat content has been observed in the years following ACLR with HT,5 and greater eccentric exercise-induced changes in size have occurred in the distal musculature,18 these factors may be relevant to consider in future investigations. It was not possible to rule out the presence of intramuscular edema as a confounder to volumetric assessment. However, a brief evaluation of Participants 4 (one day, total hamstrings Δ-2.6%) and 5 (seven days, total hamstrings Δ-2.4%) suggests that a shorter time between the final NHE session and MRI assessment may not have artificially inflated total hamstring volumes.
As the current study included a small sample and was preliminary in nature, a full evaluation of potential confounders was not possible. However, exploratory correlational analyses did not reveal associations between the percentage change in total hamstrings volume and age, time from surgery, activity level, subjective knee function, interest/enjoyment, value/usefulness, baseline strength, or baseline hamstrings volume (Appendix 2). Additionally, the magnitude of change in hamstrings volume did not appear to differ by sex (female=3.7±7.0%, male=3.0±4.3%, p=.878). As improvements in total hamstrings volumes were observed in 5 of 7 participants in parallel with strength gains despite the heterogeneity in demographics, these findings may be considered encouraging hypothesis-generating data as a foundation to build on in larger efficacy trials.
CONCLUSION
The majority of participants who had undergone primary ACLR with HT demonstrated trivial-to-moderate magnitude increases in hamstrings muscle volumes in parallel with a moderate magnitude increase in eccentric force after four weeks of isolated NHE. Inconsistent patterns of baseline volumetric impairments relative to a demographically similar uninjured cohort and variable responses to exercise appear to support the need for individualized exercise prescription in this population.
Sources of Funding
This work was funded by the Great Lakes Athletic Trainers’ Association
Conflicts of Interest
None
Acknowledgements
We would like to thank Noah Fiala for their assistance with data collection