INTRODUCTION
Upper extremity injuries are pervasive among baseball players,1–3 especially for pitchers whose throwing shoulder and elbow are subjected to significant repetitive stress from pitching.1,2 A study on high school-age baseball players demonstrated that pitchers have twice as many overuse-related injuries compared with position players.3 It has been reported that 15.7% of shoulder injuries and 25.3% of elbow injuries in high school baseball pitchers result in more than three weeks of missed participation.3 Despite various injury prevention efforts, the number of high school players suffering from pitching-related overuse injuries, including shoulder muscle strains and elbow ligament sprains, is gradually increasing.2,4 Since joint stress during pitching is directly associated with shoulder and elbow injuries sustained by pitchers,5,6 further research on pitching biomechanics is necessary to curb the increasing occurrence of injury.
Pitching is a complex whole-body motion initiated by the ground reaction force (GRF) acting on the drive leg (i.e., right leg for a right-handed pitcher) that propels the body forward.7 Once the pitcher plants the lead leg (i.e., left leg for a right-handed pitcher), the mechanical energy of the moving body is used to rotate the pelvis over the lead leg and towards homeplate.7,8 Subsequently, the proximal-to-distal sequencing of the pelvis and trunk movement and the hip-shoulder separation facilitates energy transfer from the pelvis to the trunk.7,8 The energy transferred from the trunk to the throwing arm ultimately generates ball velocity.9 Since pitching performance depends on the pitcher’s ability to harness the mechanical energy produced by the legs, pelvis, and trunk to produce ball velocity, any disruption in this intricate process may negatively affect their performance and increase the likelihood of shoulder and elbow injuries.10–13 This proposed effect is supported by the studies by Howenstein et al.7,8 that demonstrated smaller drive leg anterior impulse and smaller energy transfer from the trunk to the throwing arm are linked to higher joint moments.
The critical sequence of movement that leads to the transfer of mechanical energy from the lower extremity and trunk to the throwing arm is controlled by the lumbopelvic-hip musculature. The lumbopelvic-hip musculature includes muscles that provide spinal and segmental stability (i.e., transversus abdominis, pelvic floor muscles, diaphragm, multifidus, and quadratus lumborum) and muscles that produce powerful motion of the trunk and hips (i.e., hip, abdominal, and spinal muscles).14 Collectively, these muscles produce, absorb, and transfer mechanical energy from the lower extremity to the throwing arm.14,15 Therefore, it is not surprising that decreased function of the lumbopelvic-hip muscles has been linked to poorer pitching performance, greater joint loading during pitching, and higher injury risk in collegiate and professional pitchers.10,16–18
In prior studies, lumbopelvic-hip control was assessed using a single-leg standing balance task, which measured the amount of pelvic tilt displacement while a leg was actively lifted off the floor from a standing position.10,16–18 Chaudhari and colleagues reported that professional pitchers with small pelvic displacement during this test, indicative of better lumbopelvic-hip control, demonstrated better overall pitching performance,16 and had a lower likelihood of sustaining musculoskeletal injuries throughout the season compared to those with poorer lumbopelvic-hip control.17 Laudner et al.10 also demonstrated that decreased lumbopelvic-hip control while standing on the drive leg was associated with increased shoulder horizontal adduction and elbow varus moments during pitching in collegiate and professional baseball pitchers.
Previous studies on lumbopelvic-hip control have only been conducted on collegiate and professional pitchers. High school pitchers need to be studied separately from the college and professional pitchers since they are at different developmental stages,19 and various kinematic and kinetic differences have been found between high school and collegiate/professional pitchers.20 With the incidence of injury rising among high school pitchers,2,4 studying the relationship between lumbopelvic-hip control and joint loadings may help us better understand the injury prevention strategy in this population. Furthermore, the influence of lumbopelvic-hip control on drive leg push-off GRF, which is critical in generating mechanical energy, remains unknown. Therefore, the purpose of this study was to investigate if lumbopelvic-hip control was correlated with shoulder and elbow joint moments and drive leg GRF in high school baseball pitchers. The authors hypothesized that better lumbopelvic-hip control would be associated with lower shoulder and elbow joint moments and higher peak drive leg GRF.
METHODS
Subjects
Data from all high school baseball pitchers (n=60) who participated in a larger study were used for this study. The larger study included both high school and collegiate pitchers. Only the data from high school pitchers were used for this analysis. All pitchers had at least one year of pitching experience and were actively participating in baseball on an organized team without any injuries at the time of data collection. Informed consent and assent were obtained before participation. The study followed the protocol approved by the Institutional Review Board at the University of Texas at San Antonio.
Instrumentation
Kinematic data were captured using an eight-camera three-dimensional motion capture system (Model: T10s, Vicon Inc., Centennial, CO) at a sampling frequency of 600 Hz and a high-speed video camera (Model: Bonita) at a sampling frequency of 200 Hz. Two force platforms (Model: OR6, AMTI Inc., Watertown, MA) were embedded inside a custom-made pitching mound. The surface of the force plate was lined with a thin rubber material to prevent athletes from slipping. The platform on top of the mound was used to obtain GRF data as the pitchers pushed off the mound, and the second platform on the slope of the mound was used to identify the timing of lead foot contact with the ground. The force plate data were collected at a sampling rate of 1200 Hz and electronically synchronized with the kinematic data. The origin of the global coordinate system was set on the back-right corner of the force plate on top of the mound. The +x axis pointed towards the direction of the pitch; the +y axis pointed leftward; the +z axis pointed upward. Ball speed was recorded using a radar gun that was placed behind the net (Jugs Inc., Tualatin, OR).
Procedures
The participants wore indoor shoes and spandex shorts and were shirtless for all data collection using the motion capture system. After measuring the participant’s height and body mass, a sports specialization scale was used to assess the participant’s level of specialization.21 For the motion capture, reflective markers were placed and secured over their anatomical landmarks. The specific anatomical landmarks were the spinous process of the seventh cervical vertebrae, sternal notch, xiphoid process, acromion processes, medial and lateral elbow epicondyles, radial and ulnar styloid processes on the wrist, head of the third metacarpal on the throwing hand, anterior-superior iliac spines (ASIS), greater trochanters, medial and lateral epicondyles of the knee, medial and lateral malleoli, heel, and the tip of the shoes.13 In addition, three-marker clusters were secured over the spinous process of the eighth thoracic vertebrae, sacrum, and lateral thighs.22,23
Before the biomechanical analysis, participants were instructed to warm up using a method of their preference (e.g., gradual throwing, band exercises, jogging) and to take as much time as needed to feel comfortable pitching with a max effort in a game. Since the preferred method of warm up vary greatly from pitcher to pitcher, the warm-up time ranged between five and 15 minutes. After capturing a static trial, each participant threw 15 fastballs from the pitching mound into a net approximately 9 m (30 ft) from the pitching rubber. The kinematic, kinetic, and ball speed data were recorded for every pitch. The three fastest pitches with complete biomechanical data were used to calculate biomechanical variables.
After completing the pitching trials, the participants’ lumbopelvic-hip control was assessed using a single-leg lift test (SLLT) as described in previous stuides.10,16–18 The SLLT test was used in this study as it was used in previous studies10,16–18 to evaluate lumbopelvic stability in collegiate and professional baseball pitchers and allows assessment of lumbopelvic control in a standing position. Participants were instructed to stand erect with hands on hips, raise one leg 10 cm off the ground while flexing the hip forward and allowing the knee to flex naturally. During a wind-up, a pitcher’s lead leg is typically lifted much higher than 10 cm. The intent of the test was not necessarily to replicate this motion, but rather to assess the pitcher’s ability to maintain lumbopelvic stability in a single-leg stance. After keeping the leg up for two seconds using the verbal count guided by the timer on the computer screen, the participants lowered the leg to the starting position. The participants lifted the leg three times with a brief (2-3 second) pause in between while standing on each leg. The instruction for the SLLT was given by the same investigator for all participants. The participants practiced the test with the investigator holding a ruler beside them to ensure the leg was lifted 10 cm off the ground. The movement of the pelvis was recorded using the motion capture system during the task. For each lift, the pelvis angular displacement was calculated as the absolute difference between the maximum and minimum anterior-posterior pelvic tilt angle during the single-leg lift test.
The number of trials (i.e., lifts) each participant performed was not mentioned in the previous studies that used the same task.10,16–18 In our study, the lifts were repeated three times on each side. Based on the marker coordinate data, the lifts were considered invalid if the participant’s foot was not lifted high enough off the floor (>10 cm). The average pelvis angular displacement was calculated from the valid lifts, and the tests with at least 2 valid lifts were included in the analysis. The intrasession reliability of the pelvis angular displacement was calculated based on the three lifts from 15 participants. The intraclass correlation coefficient (ICC2,1) and standard error of measurement of the pelvis angular displacement during the leg lifts were .83 and 1.1°, respectively.
Data Processing
Raw marker coordinate data from the pitching trials were filtered using a fourth-order Butterworth low-pass filter with a cut-off frequency of 17 Hz.24 The filtered data were used to define the segmental coordinate systems. The segmental coordinate systems and the inertial parameters of the body segment, estimated using the method described by Clauser et al.,25 were used to calculate the shoulder horizontal adduction and internal rotation moments and elbow varus moment using standard inverse dynamics. The joint moments were normalized to the participant’s body weight and height. The peak anterior component of the GRF during the push-off was identified using the force plate data. Additionally, the anterior impulse generated by the pitcher during the push-off was calculated by integrating the anterior GRF generated between the max knee height and the time the drive leg left the mound. All GRF variables were normalized to the participant’s body mass.
Pelvis orientation during the single-leg test was calculated based on the pelvis segment coordinate system defined by the reflective markers. The y-axis was directed to the left, running from the right ASIS to the left ASIS, and the intermediate axis extended from the right ASIS to the right PSIS markers. The x-axis was the cross-product of the intermediate and y-axis, pointing anteriorly, and the z-axis was the cross-product of the x-axis and the y-axis, pointing superiorly. The anterior-posterior tilt of the pelvis corresponded to the rotation of the pelvis around the y-axis.
Data Analysis
The Shapiro-Wilk test for normality demonstrated that the pelvis angular displacements were not normally distributed (p<0.001). Therefore, correlations between anterior-posterior pelvis displacement during the single-leg lift tests and the biomechanical variables during pitching (i.e., shoulder horizontal adduction moment, shoulder internal rotation moment, elbow varus moment, peak anterior ground reaction force, and anterior impulse during the push-off) were examined using Spearman rho correlation coefficients. An α priori alpha level of 0.05 was set for all data analyses. The correlation coefficients above 0.1, 0.3, and 0.5 were considered to represent weak, moderate, and strong relationship, respectively.26 The statistical analyses were conducted with SPSS Statistics version 27 (IBM, Armonk, New York).
RESULTS
Data from two participants with incomplete biomechanical data were excluded from the study. Five single-leg lift trials while standing on the drive leg and seven trials while standing on the lead leg were excluded from analysis because the leg was not lifted at least 10 cm off the ground in at least two of the three lifts. The ruler used to provide feedback on leg height was not available to participants during testing, due to concerns that it might obstruct camera views for the markers. As a result, some trials with insufficient leg lift height were excluded. As a result, data from 52 pitchers were included in the analysis for the drive leg and data from 50 pitchers for the lead leg. Of the 54 pitchers included in the data analysis (age: 15.8 ± 1.3), 41 (76%) were right-handed and 13 (33%) were left-handed. Additionally, 36 (67%) were highly specialized and 18 (33%) were moderately specialized in baseball. The overall means and standard deviations for the participants’ demographics, pelvis angular displacement and biomechanical variables are presented in Table 1.
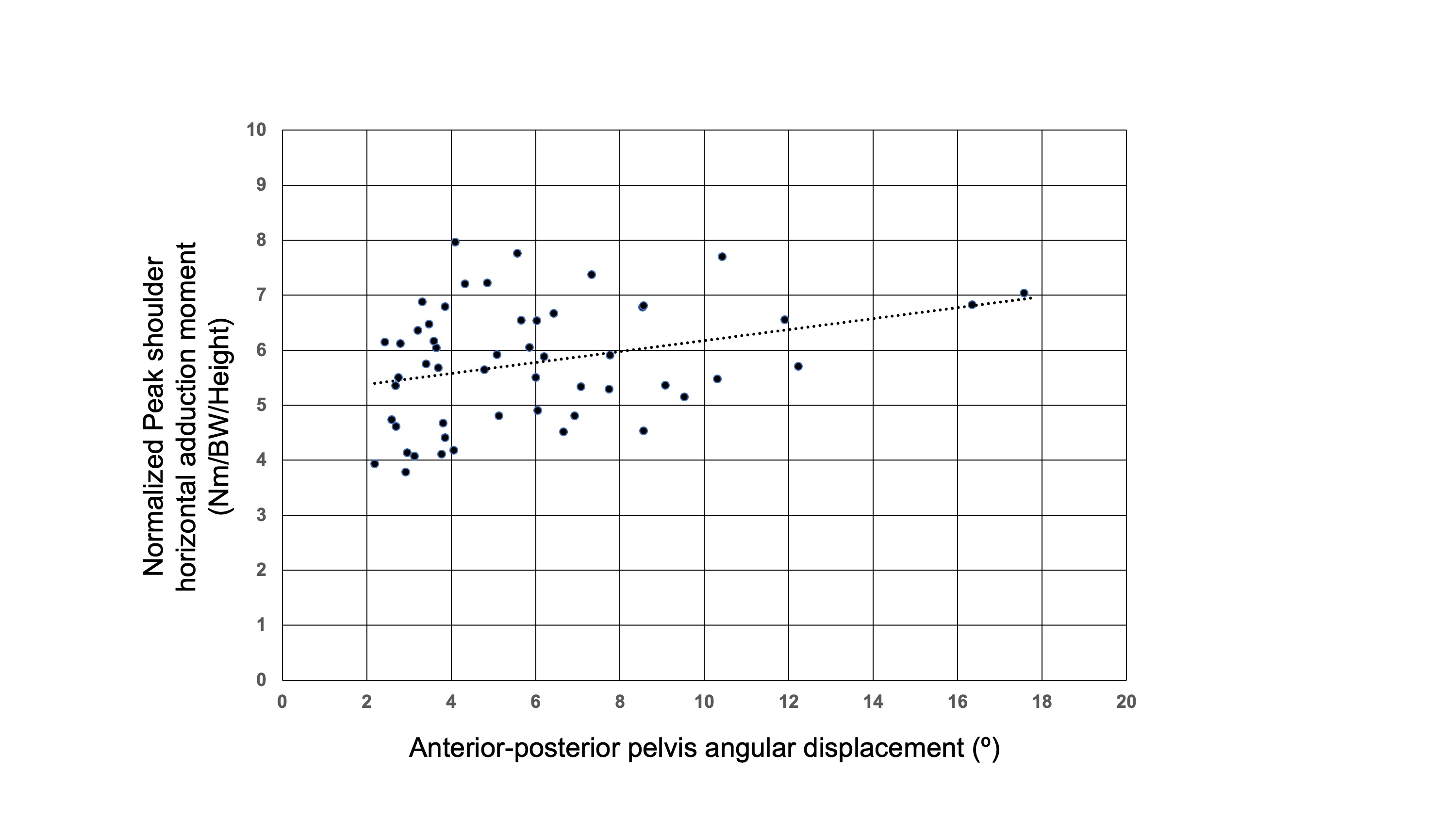
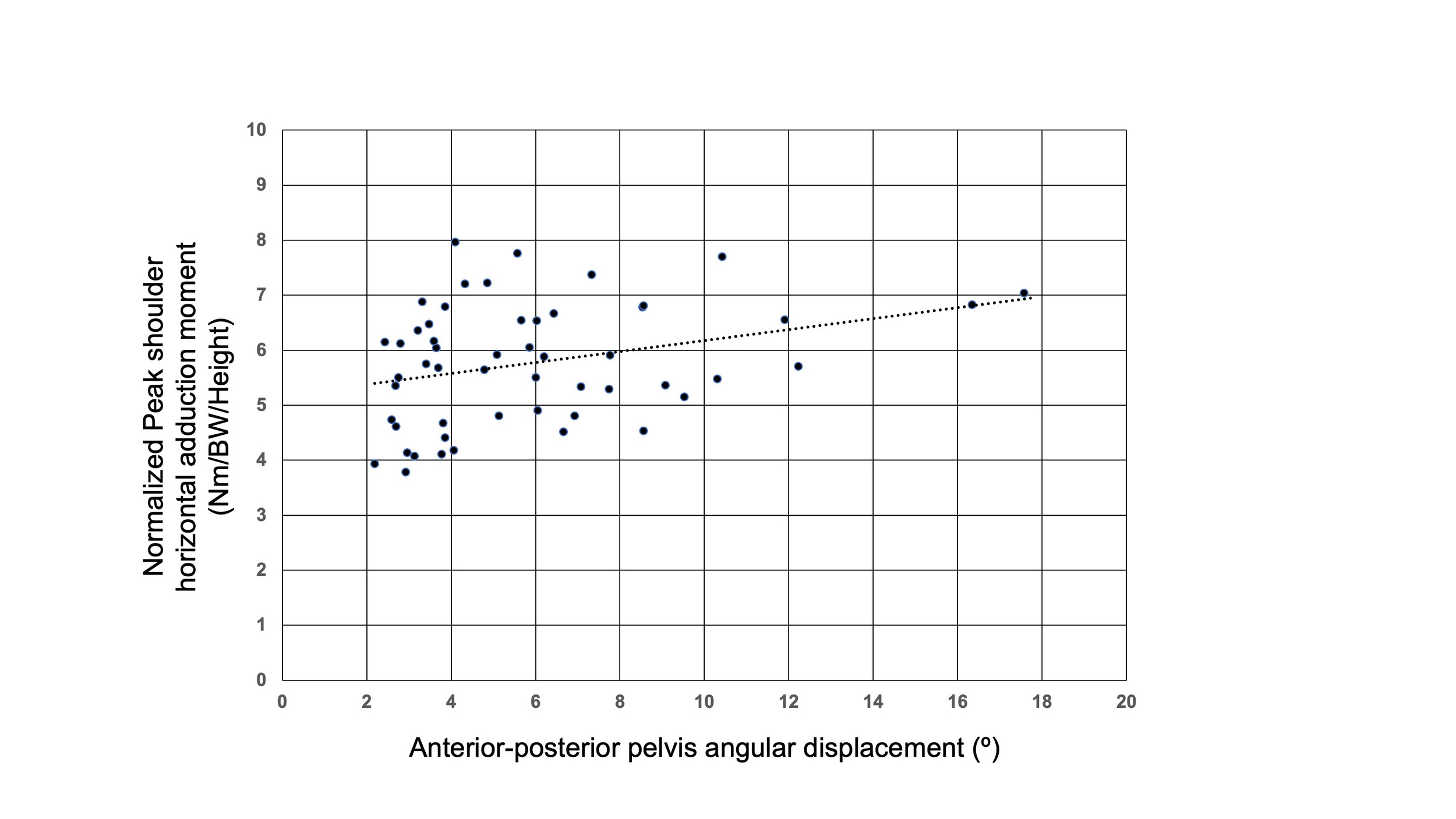
The anterior-posterior pelvis angular displacement while standing on the drive leg was moderately correlated with the peak shoulder horizontal adduction moment during pitching (r = .301, p = 0.03) (Figure 1), but not with peak shoulder internal rotation moment (p = 0.38), elbow varus moment (p = 0.46), peak anterior ground reaction force (p = 0.46), or anterior impulse during the push-off (p = 0.79) (Table 2). The anterior-posterior pelvis displacement while standing on the lead leg was not correlated with any biomechanical variables (p > 0.20).
DISCUSSION
The purpose of this study was to investigate if lumbopelvic-hip control, measured using a single-leg standing balance task, is associated with shoulder and elbow peak joint moments and drive leg GRF during the pitching motion in high school baseball pitchers. We observed that better lumbopelvic-hip control (i.e., smaller pelvis angular displacement) while standing on the drive leg was moderately correlated with lower peak shoulder horizontal adduction moment, but it was not correlated with other joint moments or the drive leg GRF variables. The lumbopelvic-hip control while standing on the lead leg was not correlated with joint moments or GRF variables.
Laudner et al.10 demonstrated that better lumbopelvic-hip control during the same single-leg standing balance task was associated with lower shoulder horizontal adduction and elbow varus torque in a group of collegiate and professional pitchers.10 In the current study of high school pitchers, better lumbopelvic-hip control while standing on the drive leg was associated with a lower shoulder horizontal adduction moment. However, the correlation between lumbopelvic-hip control and shoulder horizontal adduction moment was weaker than that reported for the collegiate and professional pitchers (r = .30 vs. r = .44), and the correlation between lumbopelvic-hip control and elbow varus moment was not observed. Body mass,6 height,6 and a number of pitching mechanics variables,27 and have been demonstrated to influence joint moments. The weaker relationship between lumbopelvic-hip control and joint moments may be reflective of the relatively greater influence of these other variables on joint moments among high school pitchers compared to adult pitchers. While the kinetic variables were normalized to participant’s height and body mass, height and body mass can influence non-normalized GRF and moment values, and thereby confound the relationship between lumbopelvic-hip control and the biomechanical variables.28 In a sense, observation of a modest, yet significant correlation between lumbopelvic-hip control and shoulder horizontal adduction moment despite the heterogeneity in the study population is noteworthy.
Although no study has directly linked higher shoulder horizontal adduction moment to baseball pitching injuries, shoulder horizontal adduction moment contributes to the production of shoulder internal rotation and elbow varus moments. During arm cocking, rapid trunk rotation toward the batter causes the arm to horizontally abduct.29,30 The shoulder horizontal adduction moment, which is produced to prevent the horizontal abduction, causes the forearm, hand, and ball to lag or rotate behind the arm due to inertia, thereby facilitates the elbow valgus and shoulder external rotation after the foot contact.29,30 Maintaining good lumbopelvic stability during the wind-up and stride phases, when the pitcher is in a single-leg stance, may help control the movement of the center of mass prior to lead foot contact, thereby influencing the sequencing of the pitching motion during the arm-cocking and acceleration phases. Lumbopelvic stability remains important during the arm-cocking phase, as it provides a stable base for trunk and arm rotation. Poorer lumbopelvic-hip control has been linked to higher elbow varus moment,10 injury risk,17,18 and poorer over all pitching performance16 in the previous studies on elite baseball pitchers. These studies collectively support the idea that poor lumbopelvic-hip control influences the pitching mechanics and the injury risk.
Previous studies by Chaudhari et al.16,17 and Laudner et al.10,18 that included the single-leg standing balance task used an inclinometer to assess pelvis angular displacement during the test, while an optical motion capture system was used in the current study. The authors do not believe the difference in instrumentation affected the study results. The optical motion capture system is considered the gold standard for motion analysis. The mean pelvis angular displacement during the single-leg lift test in the current study (6.2°) was comparable to the values reported in the previous studies.10,16–18 The median pelvic tilt in the study by Chadhari et al.17 was around 7º, whereas the average pelvic tilt in the study by Laudner et al.18 was 4-5º for the injured pitchers and 2-3º for the non-injured pitchers. Both studies were conducted on professional pitchers.
Contrary to the hypothesis, lumbopelvic-hip control was not correlated with the anterior GRF generated. Based on the idea that better lumbopelvic-hip control would facilitate greater activation and force generation by the drive leg hip musculature during the drive, the authors hypothesized that better lumbopelvic-hip control would be associated with a stronger anterior push-off force.14,31,32 Generating anterior GRF is important for pitchers. Greater peak drive leg GRF has been linked to higher ball velocity in professional pitchers,11 and greater anterior impulse has been associated with a greater transfer of energy to the pelvis, trunk, and arm in youth baseball pitchers.7 The current findings suggest that better lumbopelvic-hip control alone does not allow pitchers to push harder off the mound as they pitch. Greater lower extremity musculature strength and power,33 hip flexibility,34 and drive leg mechanics35 are suggested to play a significant role in the production of anterior force. These factors should be examined collectively to understand the physical factors contributing to the production of anterior force.
As expected, this sample of high school pitchers was shorter (1.77±0.07m vs. 1.84±0.05 m) and lighter (74.1±12.1kg vs. 82±9 kg) compared to the group of college pitchers in a previous study.20 Shorter limbs and smaller mass of the upper extremity result in lower joint moments compared to pitchers with larger arms. As the high school pitchers grow, however, the greater muscular strength and increased limb length and segment mass increases the joint moments and loading on the soft tissues surrounding the joints.20 Being in the middle of this transition makes high school pitchers vulnerable to injuries,2,4,36 which is why it is important to identify strategies to minimize joint moments in this population. The previous study demonstrated the link between lumbopelvic-hip control and joint moments in collegiate and professional pitchers.10 The current study adds to the previous study by providing evidence that the link between lumbopelvic-hip control and joint moments, though weaker, is also present in high school-age pitchers. This suggests that incorporating exercises that challenge balance and lumbopelvic-hip control while standing on the drive leg may help decrease the shoulder moment in high school pitchers. However, the effects of the exercise must be examined in an intervention study.
There are a few limitations to the current study that need to be acknowledged. Data collection was conducted in an indoor research laboratory, where pitchers threw into a net approximately 30 feet away. Although these testing conditions were standardized for all pitchers, this does not precisely replicate throwing on a standard baseball field in a game situation. Additionally, this study did not factor in physical characteristics variables, such as lower extremity muscular strength and power,33 hip range of motion,34 skill level,20 and musculoskeletal maturation level that may have obscured the relationship between lumbopelvic-hip control and biomechanical variables. Future studies using multifactorial regression analyses would allow deeper exploration into the potential relationships between dependent and independent variables.
CONCLUSION
Poorer lumbopelvic-hip control was moderately correlated with greater shoulder horizontal adduction moments among high school baseball pitchers. The study supports and extends the understanding of the influence of lumbopelvic-hip control on pitching kinetics in high school-aged pitchers. Exercises that challenge balance and lumbopelvic-hip control while standing on the drive leg may be recommended for high school pitchers. Better lumbopelvic-hip control was not correlated with the production of anterior force during the drive. Further research is needed to understand how pitchers can improve the anterior push-off force.
Acknowledgement
This study was funded by the National Athletic Trainer’s Association Research and Education Foundation (#1718GGP02). There is no other potential conflict of interest.