
INTRODUCTION
Knee extensor dysfunction on the operative side is a severe problem in rehabilitation after ACL reconstruction for return to sport. Lower knee extensor strength at six months postoperatively on the operative side is related to the return to sport1 and the risk of reinjury.2 Knee extensor strength is recommended to be measured using an isokinetic dynamometer for its reliability.3 However, the practice rate of isokinetic strength testing is low at 19.6% due to the high cost, limited space for setting up such devices, and the time required to measure.4 On the other hand, the Y-Balance test (YBT) is widely used to judge when to start jogging or modified sports activity, as the testing tools are low-cost, space-saving, and quickly measured.4
Specifically, the anterior reach distance within the YBT is related to knee extensor strength according to the results of previous studies.5,6 A cross-sectional study analyzed the relationship between YBT reach distance and isokinetic knee strength among patients who underwent ACL reconstruction, showing a significant positive correlation (r=0.591) between the anterior reach distance of the operative limb and operative knee extensor muscle strength.5 Another study analyzed the relationship between the anterior reach distance limb symmetry index (LSI) and isokinetic knee extension LSI at three months postoperatively among athletes who underwent ACL reconstruction, with the results showing a significant positive correlation between the two indexes.6 Thus, the anterior reach distance of the YBT may be helpful as a reference whenever isokinetic knee extensor strength cannot be measured.
However, limitations exist in predicting future knee extensor weakness from anterior reach at early postoperative periods in longitudinal studies. Giampetruzzi et al.7 analyzed the relationship between anterior reach distance, normalized by height, on the operative side at three months postoperatively and knee extensor strength on the operative side at three and six months postoperatively among patients after ACL reconstruction and showed a significant positive correlation (r=0.405) between them. However, the researchers concluded that anterior reach distance at three months postoperatively was not a positive predictor of muscle strength at six months postoperatively. In another study, the relationship between anterior reach distance LSI at three months postoperatively and isokinetic knee extension LSI at three and six months postoperatively among athletes who underwent ACL reconstruction was analyzed; the results showed a significant positive correlation (r=0.312) with muscle strength at three months postoperatively. This correlation was not a predictor of muscle strength at six months postoperatively.6 These findings indicate that anterior reach distance at three months postoperatively may reflect knee extensor strength. However, analyzing their association alone may not be sufficient to identify knee extensor weakness on the surgical side at six months postoperatively.
One reason for the difficulty in predicting impairment of knee extensor strength on the operative side longitudinally in patients who underwent ACL reconstruction based on asymmetry of anterior reach distance at three months postoperatively is the difference in the improvement rate between them. For patients who underwent ACL reconstruction, the LSI is commonly used to assess the functional impairment on the operative side.4 The LSI shows the percentage of improvement on the operative side based on the nonoperative value, so it is simple to identify functional impairment on the operative side, while for functions that improve early, they reach their upper limit early in the postoperative phase. Hallagin et al.8 reported composite YBT scores of 94.1±7.1 and 97.6±6.8 at 3 months after ACL reconstruction. However, in the same study, quadriceps strength showed substantial differences between the operative (67.9±27.4 ftlbs) and nonoperative (121.7±41.5 ftlbs) sides, despite the LSI not being calculated. Similarly, Mitomo et al.6 showed that the anterior reach distance LSI of the YBT at three months after ACL reconstruction was 91.8%±8.2%, compared with 65.8%±13.3% for isokinetic knee extensor strength. In these previous studies, anterior reach distance asymmetry improved in the early postoperative phase, suggesting the limitations of a simple analysis of the association between anterior reach distance and knee extensor strength asymmetry. Therefore, the hypothesis was formulated that, by setting a specific cutoff point of anterior reach distance LSI, the meaningfulness of its relationship with knee extensor strength could be determined.
Therefore, the purpose of this study was to analyze whether anterior reach distance LSI at three months postoperatively was significantly related to lower knee extensor strength on the operative side at six months postoperatively (unachieved LSI of ≥90%) and to set an optimal cutoff point for nonachievement. The anterior reach YBT can be regularly practiced in early postoperative treatment. Predicting lower knee extensor strength on the operative side at six months postoperatively based on anterior reach distance at three months postoperatively is clinically important. The hypotheses were that those with an anterior reach distance LSI of less than a specific cutoff value at three months postoperatively would be more likely to not achieve the knee extensor strength LSI ≥90% at six months postoperatively and that an anterior reach distance LSI at three months postoperatively would help predict those at risk of not achieving the criterion for knee extensor strength at six months postoperatively.
MATERIALS AND METHODS
Procedures
The study utilized a retrospective cohort design. Patient data, including demographics, surgical type, sports classification, and pre-injury level of activity, were collected from self-report questionnaires or medical notes. Anterior reach distance at three months postoperatively and isokinetic knee extension strength at six months postoperatively were obtained from the assessment chart. This study was initiated after obtaining approval from the ethics committee (approval number M2024-111). All patients were provided with the opportunity to opt out of participation in the study. Participants were allowed to obtain the information they required about the study from the authors’ website and to refuse to have their data utilized for the study.
Participants
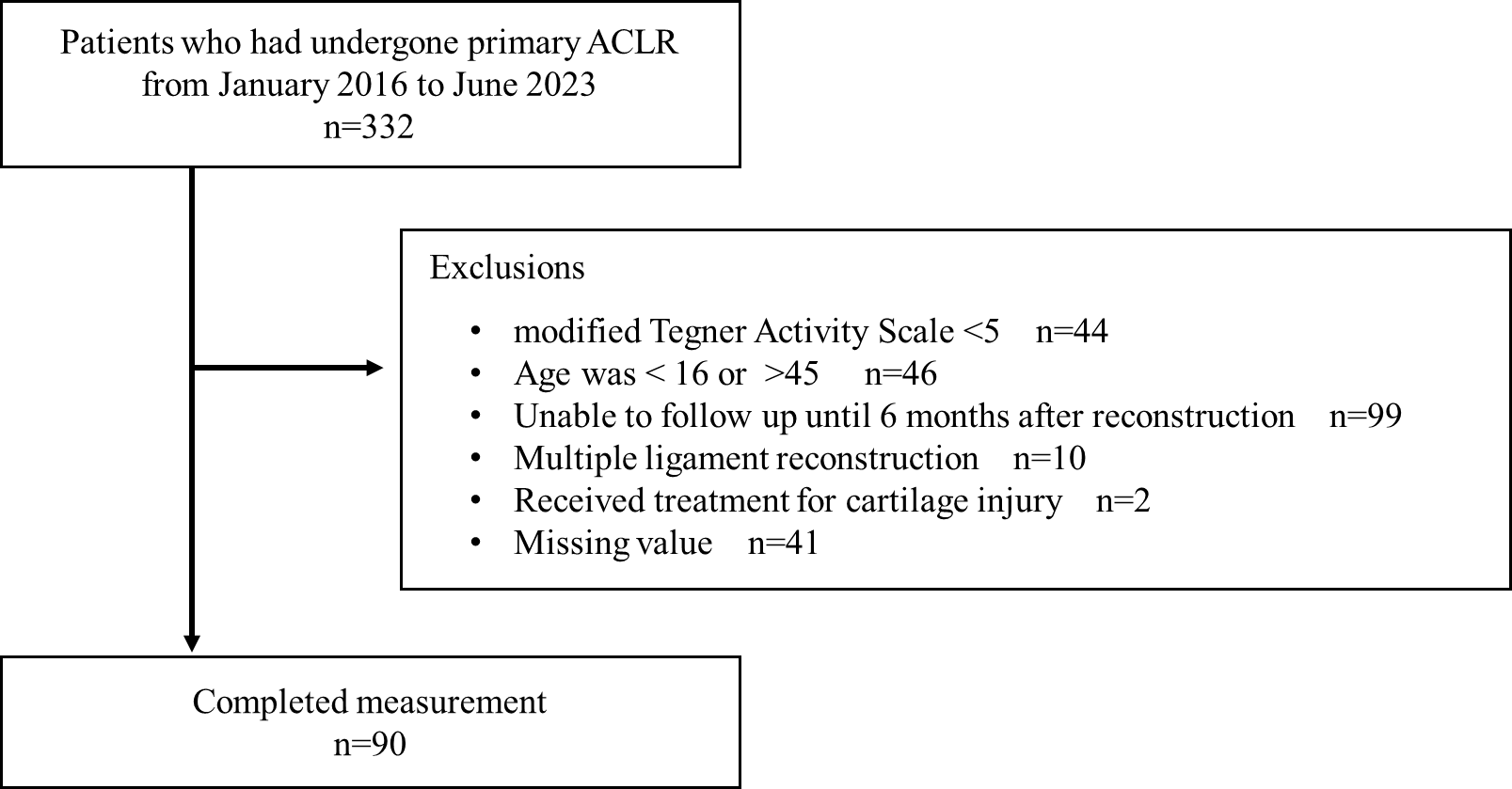
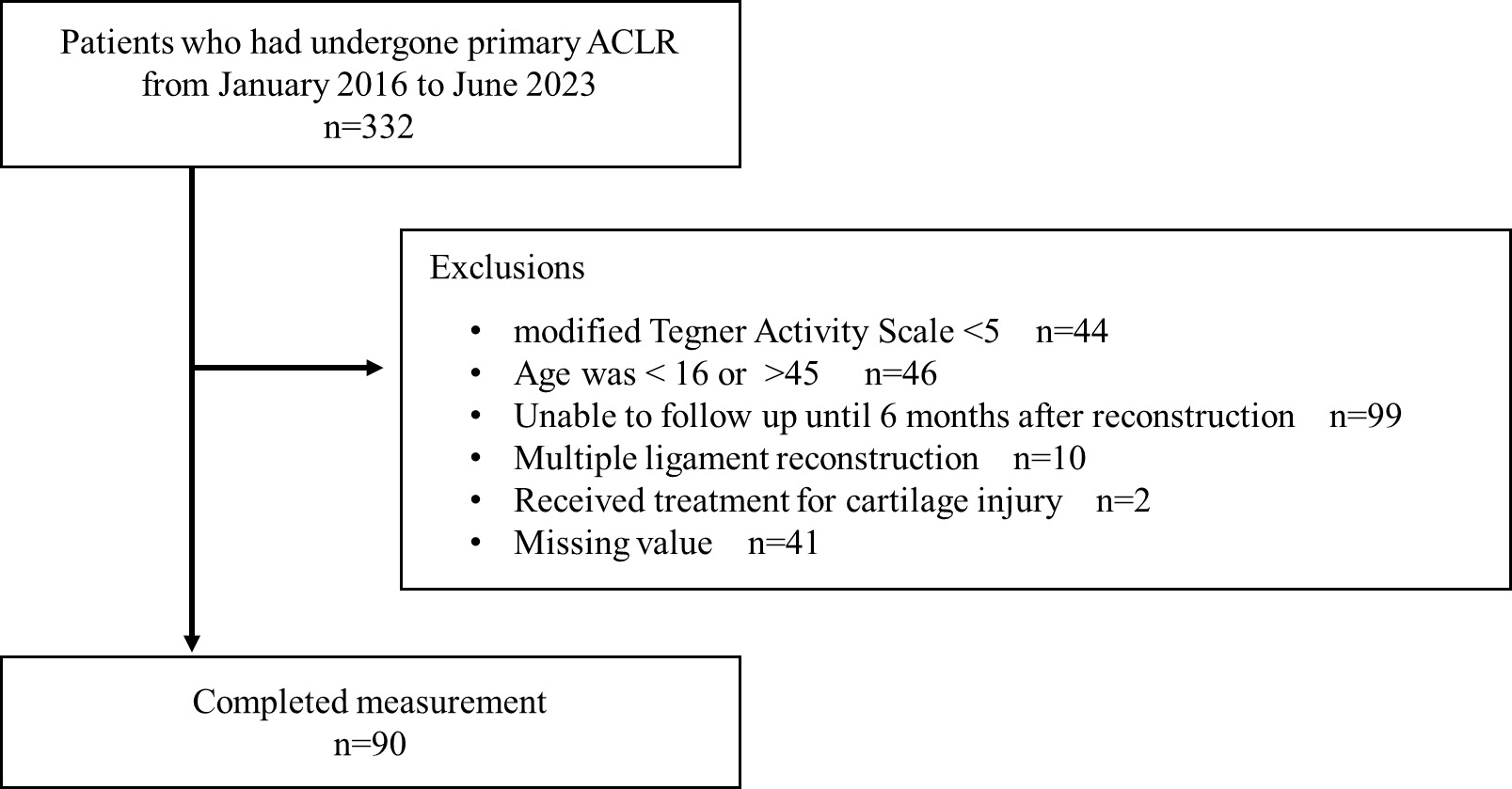
Participants included those who underwent ACL reconstruction with hamstring grafts between January 2016 and July 2023. The inclusion criteria were (1) participation in sports with a modified Tegner Activity Scale9 score of 5 or higher, (2) aged 16–45 years at the time of surgery, (3) follow-up occurring at least six months after surgery, and (4) having undergone a reconstruction with a semitendinosus graft or a graft with gracilis added to the semitendinosus. Participants were excluded if they met any of the following exclusion criteria: (1) a history of contralateral or ipsilateral ACL injury, (2) injured ligaments in the knee other than the ACL, (3) a cartilage injury requiring surgery, or (4) no participation in sports due to social reasons such as employment or pregnancy. The sample size was calculated using G*Power10 with effect size (w)=0.3, alpha=0.05, power=0.8, and a minimum sample size determined to be 88.
Surgical Technique and Postoperative Rehabilitation
All surgeries were performed by orthopedic surgeons specializing in the knee joint. Patients underwent anatomical double-bundle reconstruction with a semitendinosus graft. If the thickness and strength of the graft were insufficient for the semitendinosus alone, the gracilis was added. Postoperative criterion-based rehabilitation was based on a previous study,11 and all patients were provided with the same protocols. However, those who underwent meniscus repair were not permitted to squat with the knee bent at >90° until three months postoperatively. Rehabilitation was started on the third postoperative day. The patient was discharged from the hospital about a week after surgery and underwent outpatient rehabilitation at the hospital. Knee braces (Straight Position Knee Joint Immobilizer, Alcare Co., Ltd., Tokyo, Japan) and crutches were used for about four weeks postoperatively and gradually removed. Range of motion and isometric muscle strength exercises were started on the third postoperative day. The patient was instructed to avoid knee open kinetic chain exercises with resistance in the terminal extension range for three months postoperatively. Until then, closed kinetic chain exercises were primarily used to train knee extensor strength. Jogging was permitted after three months postoperatively, with speed and distance gradually increasing based on joint effusion and symptoms. Jumping, cutting, and agility exercises were gradually phased in at four to six months postoperatively.
Anterior Reach Distance at Three Months Postoperatively
The anterior reach distance was measured using the YBT Kit™ (Functional Movement Systems, Chatham, MA, USA) at the three-month postoperative follow-up assessment, based on previous studies.12,13 The patients performed at least a three-minute warm-up comprised of stationary bicycling without resistance and light stretches. The initiation position was one-leg standing with socks or bare feet, keeping the toe just behind the indicator line of the platform. The patient was instructed to push the measurement box as far forward as possible along the measurement pipe with the unsupported leg and then return to the starting position. The following were defined as failure attempts: the reaching leg touching the floor during the task, kicking the measurement box, or putting weight on the measurement box. The patient performed at least four practices trials, and one reach trial was then recorded.14 Each distance of the operative and nonoperative side was measured using centimeters and analyzed. The inter-rater reliability of this method was high (intraclass correlation coefficient=0.83–0.96).15,16
Isokinetic Knee Extension Strength at 6 Months Postoperatively
Isokinetic knee extensor muscle strength was measured using an isokinetic dynamometer (Biodex System; Biodex Medical Systems, Shirley, NY, USA) at the six-month postoperative follow-up assessment, based on a previous study.17 The patients performed at least three-minutes of warm-up comprised of stationary bicycling without resistance and light stretches. The patients were seated with hip and ankle joints flexed at 85°. The axis of knee rotation was aligned with the dynamometer shaft, and the bottom end of the resistance pad was fixed to the top end of the medial malleolus. The thigh, pelvis, and trunk were fastened to the chair with straps. Angular velocity was set at 60°/s, which is standard for assessing knee muscle strength.6 Before measurement, at least two repetitions were practiced. The patient then performed five repetitions of knee extension and flexion at maximum strength. The measurements were for the nonoperative followed by the operative limbs. The peak torque of isokinetic knee extensor muscles was calculated in Newton meters and divided by body weight for the analysis. The inter-rater reliability of this method was high (intraclass correlation coefficient=0.82–0.97).18
Calculated Data
The dysfunction on the operative side was assessed using the LSI. The LSIs of anterior reach distance and isokinetic knee extensor strength were calculated, with LSI calculated using (operative maximal value/nonoperative maximal value) ×100 (%). For isokinetic knee extensor strength, an LSI of ≥90% was defined as “achieved”, and an LSI <90% was defined as “unachieved”.19
Statistical Analysis
The normality of all variables was tested using the Shapiro–Wilk test, and the descriptive statistics were calculated. The normalized data were listed as means and standard deviations; the non-normalized data were listed as medians and interquartile ranges. To set an optimal cutoff point for the anterior reach distance LSI at three months postoperatively to identify if knee extensor strength could be achieved at six months postoperatively, the minimum p-value approach was used. The minimum p-value approach is a method for finding the optimal threshold influencing the outcome among continuous variables.20 The anterior reach distance LSI was set for four different categories (100%, 90%, 80%, and 70%), and the patients were divided into two groups for each category (cutoff 100: ≥100% vs. <100%; cutoff 90: ≥90% vs. <90%; cutoff 80: ≥80% vs. <80%; and cutoff 70: ≥70% vs. <70%). Chi-square tests were performed on 2×2 contingency tables for the respective cutoff points of anterior reach distance LSI at three months postoperatively and the attainability of knee extensor strength at six months postoperatively. The category with the highest chi-square value and lowest p-value was set as the cutoff point. The phi coefficients, sensitivity, and specificity were calculated for each category set as cutoff values. Data were analyzed statistically using IBM SPSS Statistics for Windows Version 28 (IBM Corp., Armonk, NY, USA). The significance level was set at 5%.
RESULTS
A total of 90 patients who met the inclusion criteria were included in the study (Figure 1).
Descriptive data are shown in Table 1.
The median anterior reach distance LSI at three months postoperatively was 93.5% (11.2 interquartile range) (Figure 2).

The minimum p-value approach showed that a cutoff point of 90% for the anterior reach distance LSI resulted in the lowest p-value and the highest chi-square value (p=0.010, chi-square value=6.553). Setting the cutoff point for the anterior reach distance LSI at 90% revealed an association between the anterior reach distance LSI at three months postoperatively and knee extension strength LSI at six months postoperatively (φ=0.270), with 38.1% sensitivity and 88.9% specificity (Table 2).
DISCUSSION
This study showed that a limb with an anterior reach distance LSI of <90% at three months postoperatively was more likely to have a knee extensor LSI of <90% at six months postoperatively. The results of this study, therefore, partially supported the hypothesis.
In this study, the mean knee extension muscle strength LSI at six months postoperatively was 83.2%. Twenty-seven participants (30.0%) achieved the knee extension muscle strength LSI ≥90%. In a previous study involving 4,093 young athletes (28.3±10.7 years, 54.3% males) who underwent primary ACL reconstruction for return to sport, the mean isokinetic knee extension LSI at six months postoperatively was 84.4%, with 35.1% of the patients achieving an LSI of ≥90%.21 Another study reported that the mean isokinetic knee extension LSI at six months postoperatively for those who underwent primary ACL reconstruction for return to sport (n=6,344, 28.7±10.8 years, 55.5% males) was 84.4%, and the rate of those who achieved an LSI of ≥90% was 33.7%.2 Therefore, the results of the present study are similar to athletes of comparable age and activity level because the means of the knee extension muscle strength values at six months postoperatively of participants were similar to those of young athletes who underwent ACL reconstruction.
In the current study, the analysis was conducted using the LSI as the functional impairment on the operative side. The mean knee extensor strength LSI at six months postoperatively was 83.2%, whereas the median anterior leg reach distance LSI at three months postoperatively was 93.5%. This indicates an earlier improvement in anterior leg reach compared to knee extensor strength on the operative side. The anterior reach distance is significantly contributed to by knee extensor strength, while other lower limb functions also influence it. In the anterior reach YBT, improvement is considered earlier because knee extensor strength can be complemented by other joints. However, when knee extensor weakness is significant, it is expected that improvement would be slower. For these reasons, analyzing their association alone may not be sufficient to identify knee extensors weakness on the surgical side at six months postoperatively; thus, a cutoff value was set to predict knee extension strength at six months postoperatively based on anterior leg reach LSI at three months postoperatively. A cutoff value for the anterior reach distance LSI at three months postoperatively was set to separate those who did not reach the criterion for knee extensor strength at six months postoperatively. The results indicated that, when the anterior reach distance LSI at three months postoperatively was set at 90%, the knee extensor LSI at six months postoperatively was significantly lower than 90% (p<0.010), with a specificity of 88.9%. This suggests that patients with an anterior reach distance LSI of <90% at three months postoperatively are at high risk of not achieving the knee extensor strength LSI of ≥90% at six months postoperatively. Conversely, with a sensitivity of 38.1%, an anterior reach distance LSI above 90% at three months postoperatively does not guarantee that the knee extensor strength LSI will be ≥90% at six months postoperatively.
No previous studies have set a cutoff value of anterior reach distance LSI at three months postoperatively to identify those at risk of not achieving the knee extensor strength LSI of ≥90% at six months postoperatively. A knee extensor LSI below 90% at six months postoperatively not only delays return to sports19 but also increases the risk of reinjury after return.2 The anterior reach YBT is widely used for daily measurements in clinical practice by therapists because it is more compact and cost-effective than the isokinetic knee strength test.4 At three months postoperatively, a simple prediction of the risk of muscle weakness of the knee extensor on the operative side at six months postoperatively might help prevent it or appropriately direct the rehabilitation plan.
Limitations
This study had some limitations. First, this study was designed for patients who underwent ACL reconstruction with hamstring grafts, so it is unknown whether it can be applied to patients who have undergone ACL reconstruction with extensor (patellar tendon or quadriceps tendon) grafts. Second, the effects of confounding factors that may be related to the anterior reach distance LSI could not be controlled for. The anterior reach distance LSI has been related to age,22 gender, sports activity,23 ankle motion,24 lower extremity function,25 and balance performance.26 To address these limitations, multivariate analyses should be performed using a sufficient sample size. Moreover, using the binary LSIs for the continuous variables, knee extensor strength, and anterior reach distance presents analytical challenges if other factors are considered. By binarizing continuous variables, interpreting data around the cutoff value may risk being disregarded. The authors believe that binarizing the results remains meaningful because the study’s hypotheses cannot be validated through analysis using continuous variables.
CONCLUSIONS
Patients with an anterior reach distance LSI of <90% at three months postoperatively have a higher risk of not achieving the return-to-sport criterion of an LSI of ≥90% in knee extensor strength at six months postoperatively. Using the anterior reach distance LSI in the early postoperative phase to predict the subsequent recovery of knee extensor strength on the operative side can be valuable in planning rehabilitation for recovery of knee extensor strength.
Acknowledgments
The authors thank all the participants who were included in this study. The authors would like to thank Editage [https://www.editage.jp/] for editing and reviewing this manuscript for the English language.