

INTRODUCTION
Baseball’s popularity continues to expand across all levels of participation, including involvement at the collegiate level.1 According to the National Collegiate Athletic Association’s (NCAA) 2023-24 Sports Sponsorship and Participation Rates Report, up to 40,247 athletes play collegiate baseball.2 These high participation rates, in combination with early sport specialization, contributes to increases in baseball participation-related injuries.3,4 In addition, repetitive high-velocity movements required of baseball players place significant amounts of stress on the shoulder and elbow joints.5 These forces may contribute to the high rate of baseball injuries involving the upper extremity, with shoulder and elbow injuries accounting for 32% of all injuries in collegiate baseball players.1 These injuries are typically time-loss in nature and often require surgical intervention to adequately return the athlete to full prior level of performance.6 As such, screening for and identifying modifiable risk factors for injury development is a clinical necessity. One modifiable risk factor of interest is shoulder strength, as deficits in shoulder strength have been postulated to contribute to the development of upper extremity injuries both at the time of injury, and persist throughout post-operative recovery.7,8
The rotator cuff and scapular stabilizers have been a point of discussion in relation to injury in upper extremity athletes due to their dual role in overhead throwing in rotational torque production during acceleration and eccentric function contributing to deceleration of the arm.9 As a result, effort has been put forth by researchers to delineate factors that may diminish the working capacity of the rotator cuff. Of note, rotator cuff fatigue following a session of pitching has been demonstrated with isokinetic strength testing.10 While the potential exists for cumulative fatigue to occur with repeated bouts of throwing over time,11 only one previously identified study has assessed shoulder strength over the course of a collegiate baseball season.12 Additionally, an overwhelming majority of existing studies on shoulder strength in overhead athletes have focused on the rotational component of shoulder strength. However, a recent study established that normalized scapular abduction (SCAP) strength is a significant predictor of ball velocity in a cohort of youth baseball players,13 and SCAP has been specifically investigated in its relation to fatigue after a bout of pitching.11 To date, only one identified study has assessed scaption strength in a collegiate baseball population.12 Further research expanding on these previous findings with a larger sample size may have the potential to serve as clinical benchmarks that can be used before, during, and after a season of play. Moreover, there is a lack of data regarding normative musculoskeletal profiles of healthy collegiate baseball players over time utilizing clinically reproducible methods, leaving a gap in the current literature regarding the thrower’s shoulder and its response to baseball activity over time in a collegiate population.
In addition to objective strength measurements, an athlete’s self-perceived function of their upper extremity is of particular importance. Self-perceived shoulder and elbow function can be assessed in the overhead athlete with the Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow score, which has been shown to be a valid and responsive tool in the evaluation of overhead athletes.14 Studies involving the KJOC have shown that scores ranging between 90 and 95% are typical of healthy professional and collegiate baseball players.15–17 However, there is no true consensus on normative KJOC scores in a healthy collegiate population, as other studies have shown mean scores of 87% and 81% in healthy, asymptomatic baseball athletes.18,19 Additionally, while KJOC scores have been shown to be unchanged over the course of a professional baseball season,20 no known studies have assessed changes in KJOC scores throughout a season in collegiate baseball players.
Therefore, the two purposes of this study were: 1) to assess changes in shoulder strength over a competitive season, and 2) to assess self-perceived shoulder and elbow function changes over the course of a competitive season in healthy Division I collegiate baseball players. We hypothesized that both dominant and non-dominant shoulder strength would differ over four time points in a competitive season, and that there would be no significant differences in KJOC scores over four time points in healthy, participating collegiate baseball athletes.
MATERIALS & METHODS
Participants
This was a prospective study monitoring changes in musculoskeletal profiles of collegiate athletes. The University of Texas Health Science Center at Houston Institutional Review Board approved all research procedures prior to data collection (HSC-MH-22-0537). Male, collegiate baseball athletes from two Division I baseball programs who participated in four testing sessions over the course of a competitive season were included in this study. Participant demographics were collected via self-report (age, position, arm dominance). Data regarding participant height and weight were recorded at the time of data collection. Participants were included in this study if they met the following criteria: (1) between the ages of 18 and 24 years old, (2) the athlete had no history of elbow or shoulder surgery in the previous year that restricted athletic participation in all team activities at the time of testing, and (3) the athlete had no current shoulder or elbow injury or pain that limited or restricted participation in all team activities at the time of testing. Athletes were excluded from the study if they were unable to participate in all team activities due to an active, ongoing injury. Individual injury and participation status was verified with the team’s Athletic Trainer. Informed consent was collected on-site in the collegiate baseball athletic training room once they were confirmed to meet the inclusion and exclusion criteria by a member of the study staff.
All data were collected using REDCap (Research Electronic Data Capture) electronic data capture tools hosted by UTHealth’s School of Biomedical Informatics. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external source.21,22
Isometric shoulder strength testing
Isometric shoulder strength measurements were taken bilaterally during each testing session. All procedures were performed in the university’s baseball athletic training room. All participants participated in measurements at the time of fall physicals (August 28th and August 30th), a preseason date (January 10th and January 17th), a midseason date (March 4th and March 18th), and a postseason date (April 29th and May 6th). Bilateral isometric external rotation (ER), internal rotation (IR), and scaption (SCAP) strength were measured with a hand-held dynamometer (HHD) (MicroFET 2, Hoggan Scientific, LLC) using a “make test” methodology.23 All shoulder strength measurements were taken by a single physical therapist (SMK) to ensure consistency. Intra-rater reliability was determined during pilot testing, including 10 subjects, and found to be excellent for all strength measures: (ER: ICC2,1 = 0.99, 95%CI [0.95-0.99], SEM = 0.03 N/kg, MDC95 = 0.07 N/kg; IR: ICC2,1 = 0.99, 95%CI [0.97-0.99], SEM = 0.05 N/kg, MDC95 = 0.14 N/kg ; SCAP: ICC2,1 = 0.98, 95%CI [0.95-0.99], SEM = 0.03 N/kg, MDC95 = 0.09 N/kg).
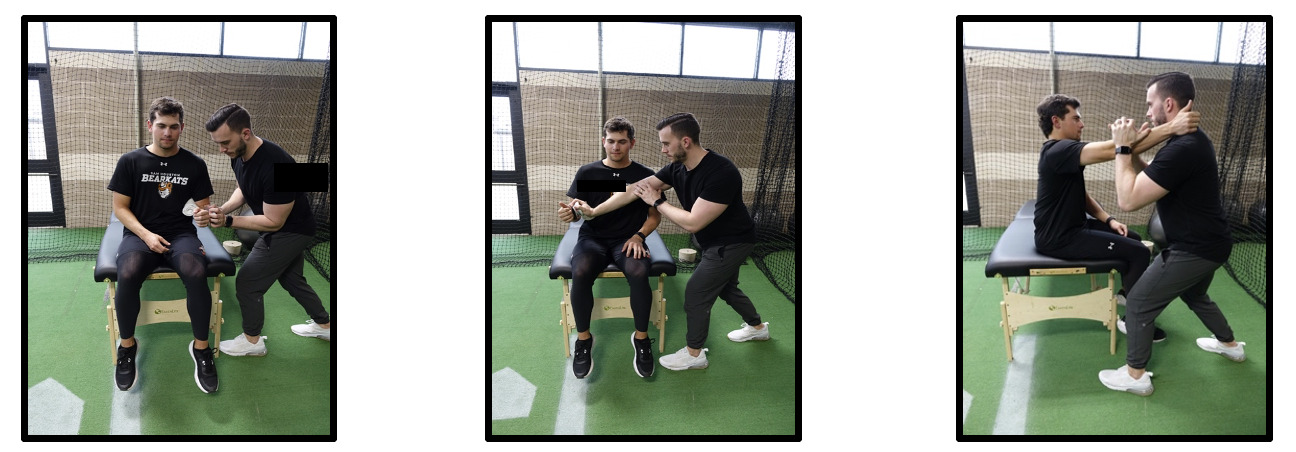
During isometric strength testing, the participant sat at the end of a treatment table in an upright seated position. For ER and IR strength testing, the participant sat with the arm positioned at the side (0° of shoulder abduction) and elbow fixed at 90°. A small towel roll was utilized under the testing arm to maintain a neutral position of the shoulder regarding the frontal plane and prevent compensation into glenohumeral abduction. Isometric rotational strength testing was measured using the HHD placed proximal to the dorsal surface of the wrist for ER and volar surface of the wrist for IR. The participant was instructed to rotate their arm outward (ER) or inward (IR) with maximum effort for up to five seconds in duration while maintaining the testing arm at the side with the elbow flexed to 90°. Tactile cueing, as necessary, was applied to the lateral aspect of the participant’s elbow to avoid compensation in the frontal plane. During SCAP strength testing, the participant sat with the shoulder positioned at 90° of elevation in the scapular plane, the elbow extended, and the forearm in a neutral position. The athlete began resting his wrist on the testing therapist’s shoulder. Isometric SCAP strength was measured using the HHD placed approximately 5 cm distal to the cubital fossa. The participant was instructed to lift their arm upward with maximum effort for up to five seconds in duration (Figure 1).
An average of two trials were taken for IR, ER, and SCAP and all measurements were taken bilaterally and recorded in pounds. If there was a wide discrepancy in measurement during one of the trials (>5.0lbs), an additional trial was recorded for consistency. Strength measures were converted to Newtons and then normalized to mass using the equation [shoulder strength measure (N) / mass (kg)]. This method has recently been shown to meet statistical assumptions for ratio normalization as it pertains to shoulder strength in baseball athletes, and has been previously used in conjunction with handheld dynamometry in professional baseball athletes.24,25 Additionally, participants completed the KJOC at each of the four testing sessions. The following verbal instructions were provided in a standardized script by one member of the study staff: “the following questions concern your physical functioning during game and practice conditions. Unless otherwise specified, all questions relate to the function of your shoulder or elbow.” Players were instructed to slide an interactive bar on a 0-10 visual analog scale for each of the 10 questions. The sum of the 10 questions were calculated to determine a final KJOC score, with a possible range of 0 to 100 points. Scores closest to 100 represent perfect function.
Statistical analysis
To test the hypotheses of this study, a 2X4 repeated measures multivariate analysis of variance (RM MANOVA) was executed to determine differences in strength across four different time points and between player position. The independent variable or within-subjects variable in this study was time: fall physical, preseason, midseason, and postseason. The second independent variable, or between-group variable, was player position. Player position was defined as pitchers compared to non-pitchers. There were six dependent variables consisting of dominant arm and non-dominant arm shoulder ER, IR and SCAP strength. The assumption testing was conducted to check for normality, outliers, linearity, and multicollinearity. Normality was confirmed using the Shapiro Wilk test. All dependent variables were normally distributed except for non-dominant arm scaption and internal rotation at the fall physical measurement session. Outliers were defined as 3 standard deviations below and above the mean for each of the time points across all of the dependent variables. No outliers were found within the data set confirmed by Mahalanobis Distance. None of the variables showed multicollinearity as depicted by a Pearson Correlation of >0.90. While there were a few violations in the normality of the data the MANOVA is robust to moderate violations in normality. Wilk’s Lambda was used to interpret the results of the RM MANOVA as this statistic is robust to violations of normality.26 Mauchly’s Test of Sphericity was used to determine if a sphericity violation was present. If a violation was present, the Greenhouse-Geisser statistic was used for interpretation of the analysis. Effect sizes were reported as partial eta squared and values of 0.01, 0.06, and 0.14 were utilized to determine a small, medium, and large effect.27 Follow-up pairwise comparisons were conducted to determine significant differences between time-points and between position groups utilizing a Bonferroni correction. All data were analyzed using statistical package SPSS version 29 (IBM Corp. Armonk, NY, USA). Alpha was set a prior at p < 0.05.
A priori power analysis (G*Power 3.1) was performed to determine the requisite sample size needed to detect significant findings in this study. An observed medium effect size (d = 0.62) was observed from a previously established study investigating changes in rotator cuff and periscapular strength in collegiate baseball athletes over time.12 As such, we anticipated a similar medium effect using partial eta squared (0.06) for sample estimation. For clarity, the authors input the following variables: effect size (f = 0.25, calculated directly from a “medium” partial eta squared effect size), α error probability (0.05), power (0.80), number of groups (2), and number of measurements (4). An estimated sample of 34 players was determined to be necessary to detect difference in shoulder strength between position groups, and a minimum of 48 players to detect statistically significant differences in strength over time.
RESULTS
A total of 49 healthy collegiate athletes were available for testing at all four timepoints and consented to participate in this study. Descriptive statistics for each participant can be found in Table 1.
There was a significant effect of time on shoulder strength across four time points, Λ = 0.14, F (18,30) = 10.67, p < .001. η2 = 0.87. There was no significant effect of position group (Λ = 0.85, F (6,42) = 1.28, p =.888 η2 = .15), nor a significant interaction effect between time and position group (Λ = 0.67, F (18,30) = 0.83, p =.655, η2 = 0.33).
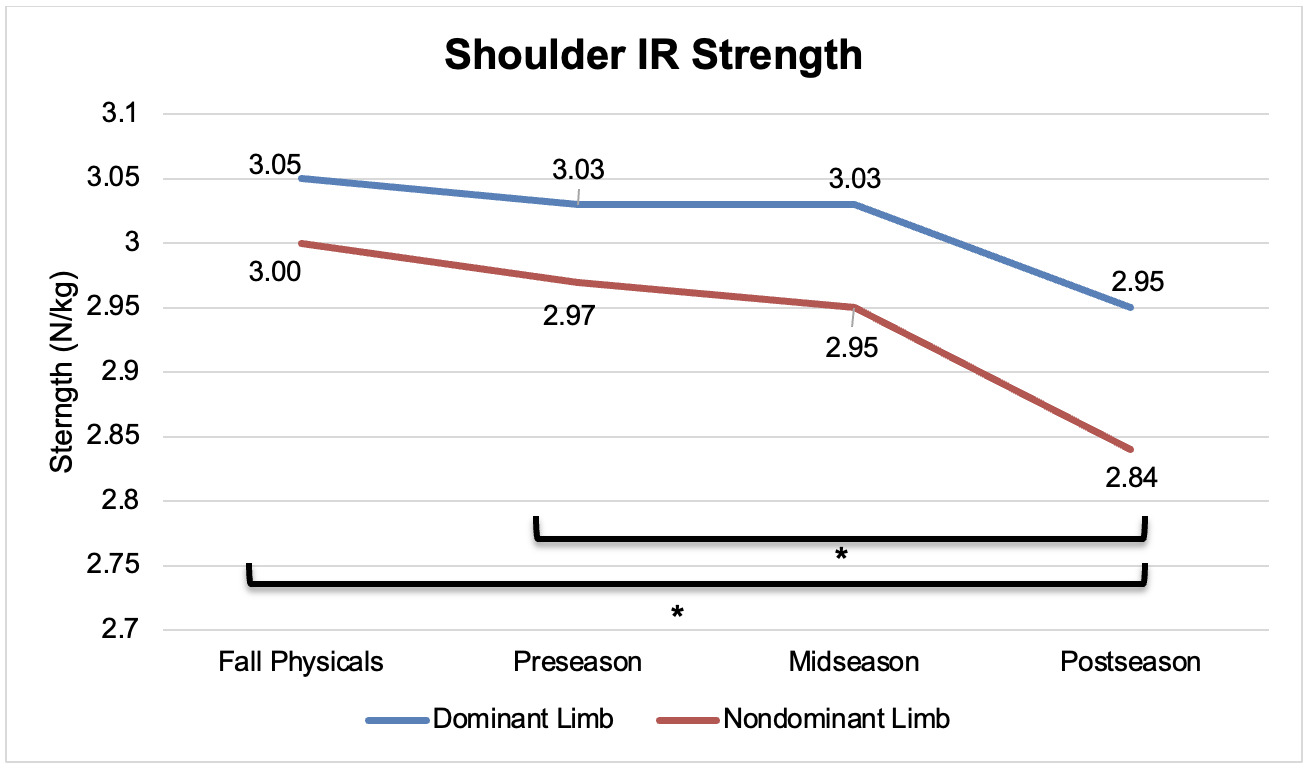
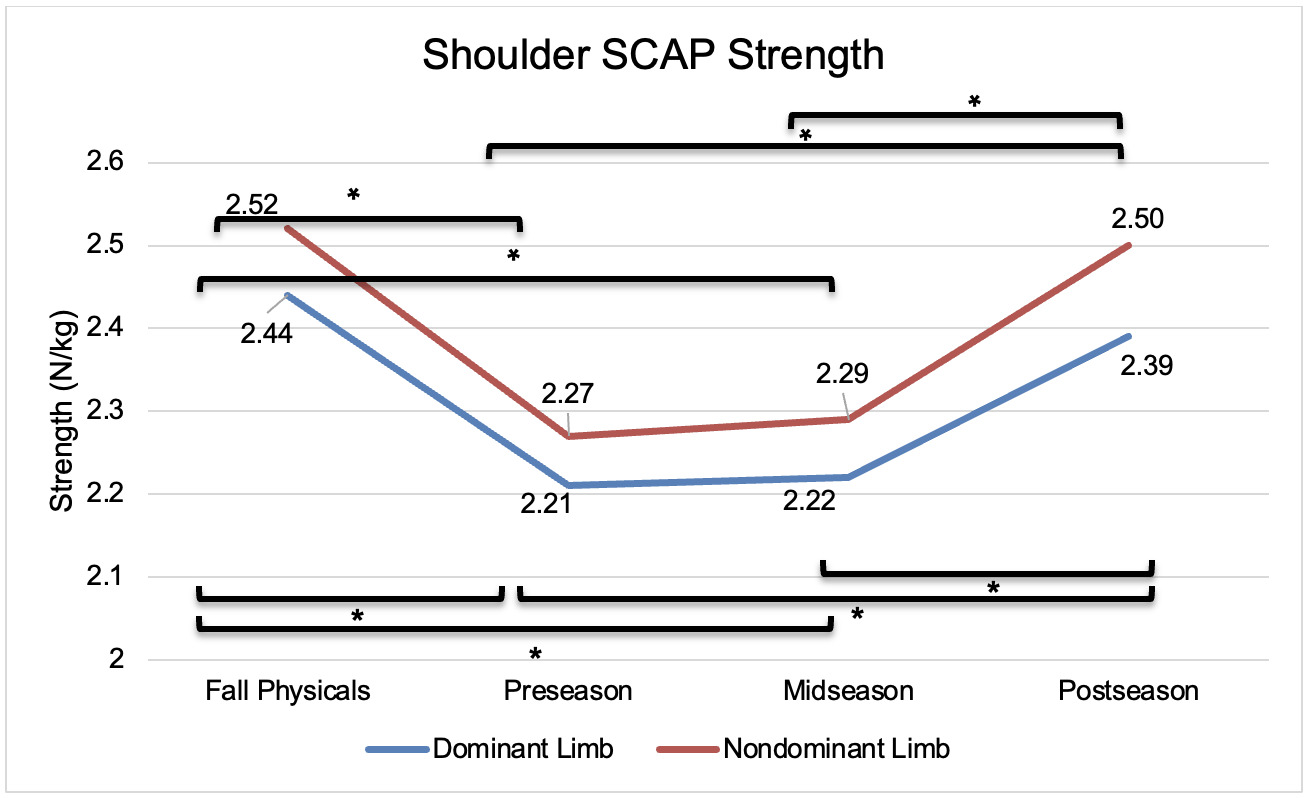
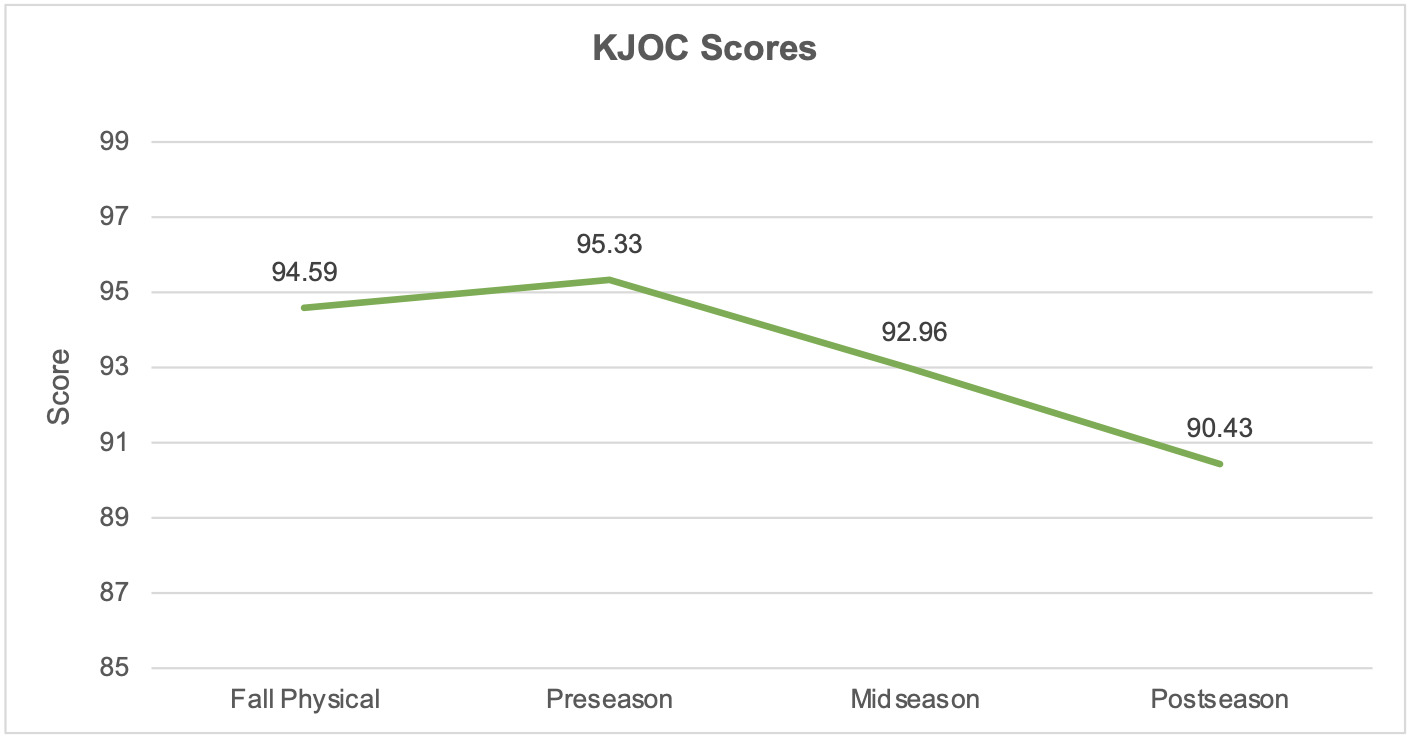
Over the four measured timepoints, dominant limb ER (F = 4.28, p = 0.01, η2 = 0.08), dominant limb SCAP (F = 9.46, p = < .001, η2 = 0.17), non-dominant limb ER (F = 2.39, p = 0.002, η2 = 0.11), non-dominant limb IR (F = 4.92, p = .004, η2 = 0.10), and non-dominant limb SCAP (F = 26.30, p < .001, η2 = 0.26) were found to statistically change over the course of the four timepoints. A non-significant effect of time on dominant limb IR strength (F = 1.94, p = .131, η2 = 0.04) and KJOC scores (F = 2.06, p = 0.154, η2 = 0.04) were observed. Normalized strength values for all measures and limbs, as well as KJOC scores, across all four time points are in Table 2.
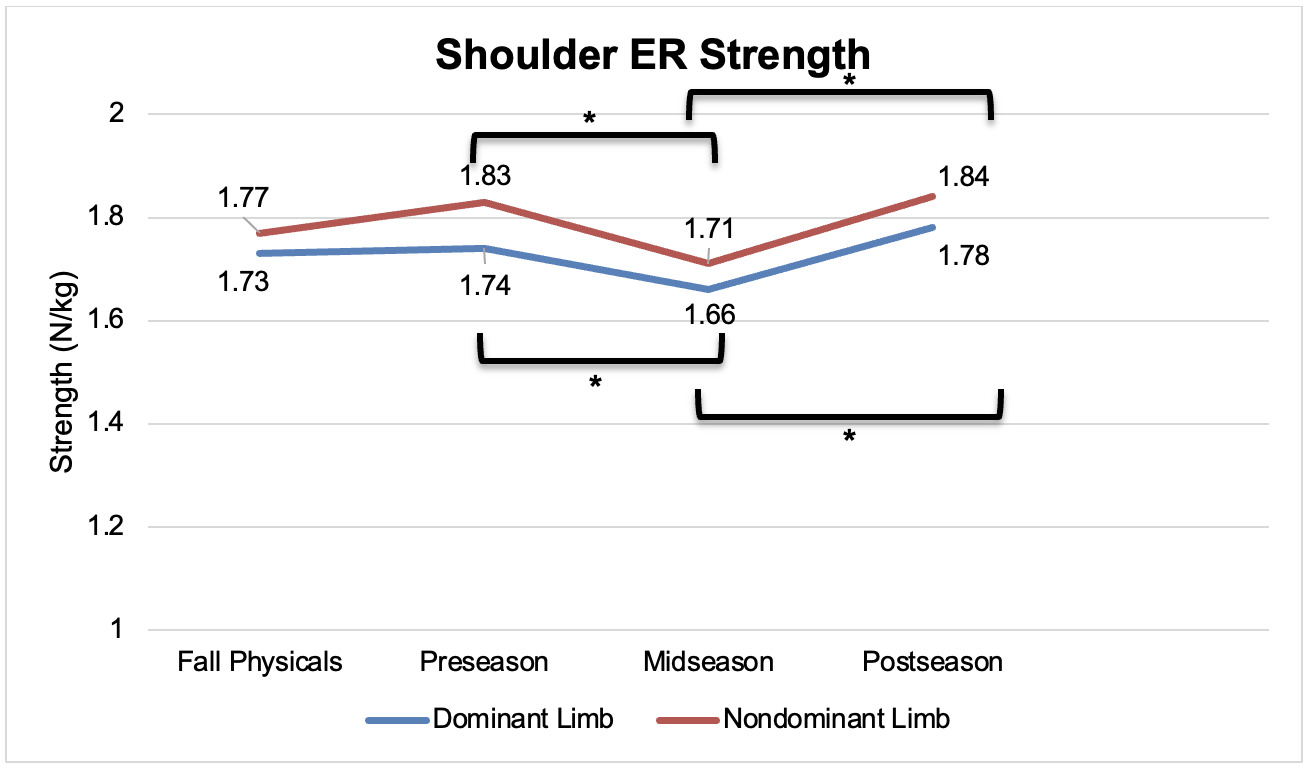
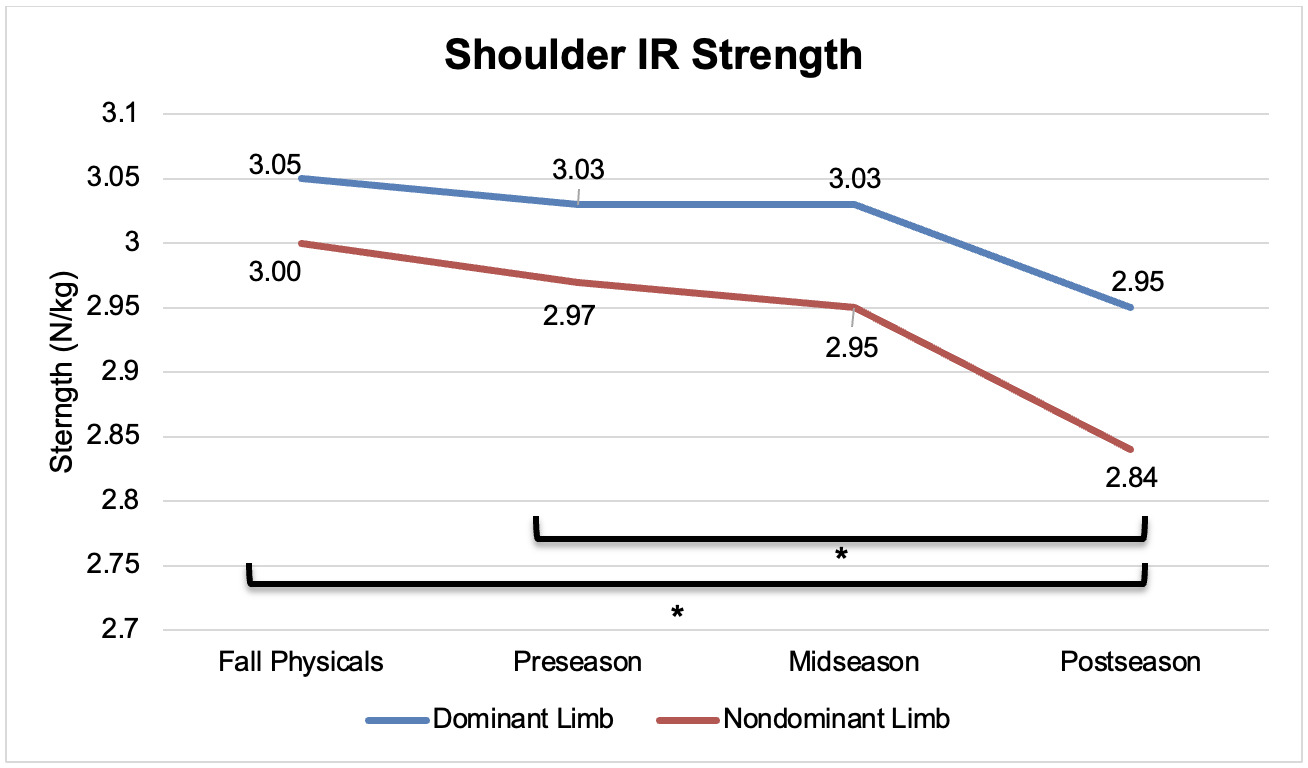
For the dominant limb, shoulder ER significantly decreased from pre- to midseason (mean difference = -0.08 N/kg, p = 0.031, 95% CI [-0.16, -0.01]) but significantly increased from mid- to postseason (mean difference = 0.12 N/kg, p = 0.019, 95% CI [0.01,0.022]). Each of these changes exceeded the established minimal detectable change value of 0.07 N/kg. Dominant shoulder SCAP also differed significantly between multiple points, including a significant decrease from fall physicals to preseason (mean difference = -0.22 N/kg, p = <0 .001, 95% CI [-0.35,-0.10]), a significant decrease from fall physicals to midseason (mean difference = -0.22, p <0 .001, 95% CI [-0.33,-0.01]), a significant increase from pre- to postseason (mean difference = 0.18 N/kg, p = .007, 95% CI [0.04,0.32]), and a significant increase from mid- to postseason (mean difference = 0.17 N/kg, p = 0.026, 95% CI [0.01,0.33]). Again, each of these observed changes in dominant limb SCAP strength exceeded established minimal detectable change scores (0.09 N/kg). Dominant limb IR shoulder strength did not significantly differ between any of the four timepoints.
For the non-dominant limb, ER strength significantly decreased from pre- to mid-season (mean difference = -0.11 N/kg, p = 0.004, 95% CI [-0.20,-0.03]) and increased from mid- to postseason (mean difference = 0.12 N/kg, p = 0.021, 95% CI [0.01,0.24]), each of which exceeded established minimal detectable change scores. Non-dominant shoulder IR strength significantly decreased from fall physicals to postseason (mean difference = -0.16 N/kg, p = 0.009, 95% CI [-0.29,-0.03]) and from preseason to postseason (mean difference = -0.13 N/kg, p = 0.029, 95% CI [ -0.25,-0.01]). While statistically significant, the change from pre- to postseason may not be clinically meaningful as the difference in normalized IR strength did not exceed the minimal detectable change scores (0.14 N/kg). Finally, SCAP strength significantly differed between four timepoints: SCAP strength significantly decreased from fall physicals to preseason (mean difference = -0.26 N/kg, p < 0.001, 95% CI [-0.38,-0.13]) and from fall physicals to mid-season (mean difference = -0.24 N/kg, p < 0.001, 95% CI [-0.34,-0.13]). Non-dominant shoulder SCAP strength significantly increased from preseason to postseason (mean difference = 0.23 N/kg, p < 0.001, 95% CI [0.11,0.35]) and from mid- to postseason (mean difference = 0.21 N/kg, p <0 .001, 95% CI [0.08,0.35]). Each of these significant findings exceeded the minimal detectable change scores for shoulder SCAP strength (0.09 N/kg) Figures 2-4 graphically represent shoulder strength changes for each measure and changes in KJOC scores between the four timepoints (Figure 5).

_scores_over_time.png)
Regarding KJOC scores over the course of a competitive season, male collegiate baseball athletes demonstrated a slight increase of scores from fall physicals to preseason, followed by decreases at mid- and post-season. The mean difference from fall physicals to postseason scores was -4.90 points. These fall in a range of previously reported minimal detectable change scores for different versions of the KJOC utilized in baseball athletes (range 2.42-8.5 points).28–30 Due to a non-significant univariate test for KJOC scores, pairwise comparisons were not conducted.
Discussion
The results of the current study demonstrate changes in shoulder across the course of a season in healthy Division I collegiate baseball players. These findings add value to the existing literature by further detailing the expected changes a participating, uninjured collegiate baseball athlete will experience over time. Significant differences were found between at least one time point for all measures of shoulder strength with the exception of dominant limb IR strength. Dominant and non-dominant limb SCAP demonstrated the largest absolute changes in shoulder strength through a significant decrease in strength during the fall season, and near full recovery of fall physical strength from mid- to postseason. Dominant and non-dominant limb IR decreased over the course of a competitive season, and shoulder ER strength for both limbs demonstrated both significant decreases, followed by increases, throughout a competitive season. There were no significant differences in KJOC scores over the course of a competitive season. These collective results support the hypotheses: there were significant differences in shoulder strength over time, and there was a lack of significant change in KJOC scores throughout a competitive season in this cohort.
Limited data exists regarding prospective, normative values of musculoskeletal profiles of overhead collegiate athletes, including studies conducted on shoulder strength. Prior to fully understanding the role clinical objective measurements have on injury risk profiles, it is a clinical necessity to understand the normative and evolving musculoskeletal profiles of baseball athletes. Recently, an article was published by Pabian et al. investigating strength changes in the dominant limb of 18 collegiate baseball pitchers.12 While both studies utilized a cohort of Division I baseball athletes, differences in methodology (testing positions) and units reported (kilograms versus Newtons per kilogram) render the results difficult to directly compare. Both Pabian et al. and the results from the present study demonstrated non-significant decreases in dominant limb IR strength over the course of a competitive season.12 Additionally, both studies demonstrated decrease in dominant limb ER from pre-to-midseason, a finding in this study that is clinically relevant (change beyond MDC90 of 0.07), with a subsequent increase from mid-to-postseason.12 Alternatively, the results from this previously published study demonstrated significant decreases in dominant-limb scaption strength over the first and second half of a season.12 These findings are conflicting with the results of the present study, as no changes were observed from pre-to-midseason with a significant and clinically relevant increase from mid-to-postseason. The present study offers advantages when considering the methodology and sample obtained: the present authors utilized a statistically supported strength normalization method to better account for anthropometric differences in baseball athletes,13,25 and included a larger and more heterogenous sample size of baseball athletes, consisting of both pitchers and non-pitchers.
Regarding normative shoulder strength profiles in collegiate baseball athletes, our findings are consistent with previous studies for single timepoint investigations. Two previously published studies found an effect of limb dominance on throwing limb IR strength, demonstrating an increase in dominant limb IR strength when compared to the non-dominant limb.31,32 However, these studies did not specify the time of year the testing protocol took place, and one study included Division III baseball athletes.32 Likewise, previous studies have demonstrated equal or non-significant weakness of dominant limb ER strength in baseball populations.33,34 Clinicians are encouraged to consider differences in methodology when attempting to compare clinical findings to published data when delineating changes in shoulder strength.
While the evidence surrounding the effect of time on shoulder strength measures in the collegiate baseball population is currently limited, the effect of time on shoulder strength has previously been investigated across a collegiate softball season.35 Softball position players demonstrate no significant change in shoulder IR strength on either side (dominant or non-dominant) over the course of the season.35 These results are in agreement with the present data for the non-dominant side, however, no significant differences were observed in dominant limb IR strength over time. In contrast to the results of the current study, a significant decrease in shoulder ER strength was seen bilaterally,35 whereas the current cohort observed a similar decrease from pre-to-midseason, followed by an increase in ER strength from mid-to-postseason. It is important to note baseball players and softball players should not be directly compared, however, the time-specific changes to overhead athlete’s shoulder strength profiles must be considered. The observed differences in results between the two populations may be related to anthropometric differences second to sex and differences in overhead throwing biomechanics.36–38 Additionally, training methodology and throwing volume may vary significantly between sports, which may further impact strength changes over a season.
Scaption strength is of particular interest in this cohort as only one previously identified study has investigated this measure in collegiate baseball athletes.12 SCAP weakness has previously identified as a risk factor for time-loss injuries in baseball pitchers necessitating surgery.39 SCAP strength in particular has been postulated to provide a global measure of dynamic shoulder stability, requiring activation of multiple periscapular and rotator cuff musculature as evidenced by increased maximal voluntary isometric contractions during isometric strength testing.40–42 During the overhead throwing motion, these muscles play a significant role in providing dynamic stabilization at the glenohumeral joint while simultaneously producing supraphysiologic rotation velocities and torque about the shoulder.43 Additionally, the posterior rotator cuff acts eccentrically to control arm deceleration and control glenohumeral distraction forces during the overhead throwing motion,44 leading to previously described morphologic changes in rotator cuff thickness and stiffness in collegiate baseball athletes.45–47 It is has been demonstrated that SCAP strength decreases over time in collegiate baseball,12 however, the current results show a peak in SCAP strength from mid-to-postseason. The present authors can only draw inferential rationale for this phenomenon, which may include a performance related adaption as these athletes experience a relative peak in competitiveness toward the end of the regular season as the season transitions to post-season play. While the time-dependent nature of rotator cuff morphology and, in turn, changes in shoulder SCAP strength have been previously studied in isolation, the presents results require further investigation into the evolution of rotator cuff morphology and shoulder strength over time.
The KJOC is a numeric score representing self-reported function of the shoulder and elbow specifically designed and validated for overhead populations.14 The results of the present study reveal a non-significant decrease in mean KJOC scores over the course of the competitive season. While no other study has investigated time-related changes in KJOC strength in healthy, competing baseball athletes, the current results are consistent with other single timepoint studies.16,21 Kraeutler et al. demonstrated a mean pre-season KJOC score of 94.82 in professional baseball pitchers, similar to the current findings of a score of 95.33 at preseason measures.16 Likewise, Franz et al. found a KJOC score ranging from 96.8-97.1 in healthy, professional baseball players without a history of arm injury.21 However, there is a paucity in the literature that details the psychometric properties of the English version of the KJOC and, although the present findings are non-significant, there are no known published minimal clinically important difference scores available to further analyze the interpretation of these changes.48 As the KJOC score is a responsive measure to detect changes in self-perceived function in baseball athletes, this tool, combined with the previously published scores for healthy, uninjured baseball athletes, the present data can be used as a reference to compare observed scores and potentially screen athletes who are perceiving deficits in perceived arm health.
This study is not without limitations. First, the current study included athletes from only local Division I collegiate baseball teams; results may not be directly applicable to similar athletes at other collegiate levels of play (Division II, Division III, etc.). Second, variations in training approaches across Division I baseball may influence shoulder strength changes throughout the course of a season; the present study did not include or monitor any strengthening interventions throughout the season; therefore, no definitive conclusions can be drawn on the effects of participation in an in-season shoulder strengthening program on shoulder strength testing. Testing positions for rotational shoulder strength varies across the literature. In this study, rotational shoulder rotational strength was measured isometrically in a seated position with the elbow flexed to 90° with the shoulder in neutral at 0° of abduction. This position allows for improved standardization of the measurement position but is not representative of a functional throwing position and may allow for increased recruitment of secondary muscle groups compared to other measurement positions. While the study staff continuously monitored the testing positions for substitutions (trunk lean, trunk rotation, etc.) during isometric strength testing, the results could be impacted by the methodology employed. Finally, the results of this study did not assess for differences between playing position, although significant variations in throwing volume and performance demands exist between these groups. However, no significant were found effect for position, suggesting that pitchers and position players demonstrate similar observed changes in normalized shoulder strength over time.
CONCLUSIONS
Collegiate baseball players demonstrate statistically significant changes in body mass normalized shoulder strength over the course of the competitive season without statistically significant changes to self-perceived function. No differences were detected between pitchers and non-pitchers, suggesting these changes over time are not position-specific despite differences in the throwing-related demands between pitchers and non-pitchers. The methodology employed, particularly the use of a normalization method to improve comparability between athletes of differing anthropometric profiles, can be reliably and readily reproduced by clinicians and researchers. These shoulder strength values can be used as clinical benchmarks when evaluating strength in similar populations over the course of a competitive collegiate baseball season.
Conflicts of interest
None of the authors have any conflicts of interest to disclose.