

Introduction
The rectus abdominis (RA) is a prominent superficial muscle of the anterior abdominal wall, contributing to motions such as trunk flexion, stabilization of the pelvis, and maintenance of intra-abdominal pressure. Creating intra-abdominal pressure is required for physical functions such as coughing, vomiting, and defecation. Given its functional relevance, the RA has been the focus of investigations in a variety of fields such as orthopedics, sports medicine, and rehabilitation, as well as general surgery and obstetrics. Both structural and functional alterations of the RA are implicated in many conditions, including abdominal wall hernia, diastasis recti, and post-surgical complications, underscoring the need for accurate and reproducible assessment methods.
Musculoskeletal ultrasound (MSKUS) has become an increasingly utilized tool in the evaluation of abdominal wall musculature due to its capacity for real-time, dynamic imaging. Compared to magnetic resonance imaging (MRI) or computed tomography (CT), MSKUS provides a cost-effective, non-ionizing, and readily accessible method for quantifying muscle morphology, thickness, and contraction dynamics. Moreover, the ability to perform serial measurements without exposing patients to radiation makes MSKUS particularly valuable in longitudinal research and clinical monitoring. Despite its advantages, methodological variability in transducer placement, operator dependence, and image interpretation remain challenges that warrant further investigation.
Anatomy of the Rectus Abdominis
The RA consists of two long muscles that run superficially along both sides of the linea alba (LA) along the ventral abdominal wall. The linea alba is a thick band of connective tissue that divides the two muscles vertically. The RA is commonly known as the “six-pack” muscle in individuals with lower body fat levels. The horizontal intersections that give the appearance of the “six-pack” are 3 tendinous intersections that are located at the level of the umbilicus, the xiphoid process, and the last midway between the two. The RA runs from the mid to lower rib cage (ribs 5-7 and the xiphoid process) distally to form two tendons that attach to the pubic symphysis and the pubic crest. The RA lies within the rectus sheath, which is a connective tissue that is formed by the merging of several abdominal muscles, including the transversus abdominis, the external and internal oblique muscles. Having a good grasp of the abdominal muscle anatomy is essential for accurate MSKUS assessment to determine which muscles are injured, the injury type, and severity.
RA injuries from activity are rare in the average clinical practice; however, they can be more common in those who perform frequent and strenuous exercise.1 Rectus muscle strains have been reported in many sports, including tennis, soccer, baseball, and weightlifting.2–6 Although there is no true consensus on what is injured in athletic pubalgia or a “sportsman’s hernia,” this injury can comprise the RA and other muscles, including the pubic symphysis enthesis, the inguinal canal, the conjoint tendon or myotendinous junction, and the adductor muscle attachment site.7,8 Complete RA rupture is rare, but has been reported during weightlifting, handball, tennis, paratrooping, and blunt force trauma to the abdomen.4,9–16
Another common mechanism of injury is pregnancy, in which diastasis rectus abdominis can occur. This condition is a connective tissue impairment resulting from a separation of the two RA muscles during and following pregnancy.17 Diastasis rectus abdominis tends to resolve after about 6 months; however, about a third of cases are still affected after an entire year.18–20
The Role of MSKUS in Evaluation of the RA
Advantages
- Real-Time Imaging: MSKUS allows dynamic evaluation of muscle and tendon integrity while contracting the abdominal muscles or simply breathing.
- High-Resolution Visualization: MSKUS provides detailed images of soft tissue structures, including the RA muscle, tendon, and attachment to ribs and pubic bones.
- Accessibility and Cost-Effectiveness: MSKUS is portable, widely available, and less expensive than MRI.
Limitations
- Operator Dependency: MSKUS requires skill and experience for accurate interpretation of findings. The ability to sonograph tendons is to a large extent influenced by the operator and the availability and technical considerations of state-of-the-art equipment.
- Depth Limitations: Visualization of the RA is very easy due to its superficial depth.
- Artifacts and Shadows: For most of the length of the RA, there are no bones or calcifications that will create any artifact. There are bony attachments at the ribs, xiphoid process, and pelvis.
Sonographic Technique for Evaluating Triceps Tendon and Muscle
Equipment Setup
- Transducer Type: Because of the superficial nature of RA, a high-frequency, linear array transducer is normally used.
-
Patient Position: The patient is supine in a relaxed position. The transducer is placed in either the transverse axis (SAX) or longitudinal axis (LAX) beginning at the ribs and xiphoid process and working distally.
-
Dynamic Assessment: Dynamic movements, such as trunk flexion, can be performed during MSKUS to visualize muscle contraction and to quantify separation in diastasis recti.
Examination Protocol
Normal Sonographic Appearance
Typically, the transducer will be placed near the proximal portion of the RA perpendicular to the muscle fibers in the SAX. In this position, the transducer can be moved both proximally and distally and can examine the RA in the transverse plane. The cross-section of the RA will be seen as fibular hypoechoic muscle tissue. Additionally, the examiner should be able to easily discern the hyperechoic linea alba and rectus sheath.
For a view of the RA in the LAX, align the transducer parallel to the rectus fibers and then sweep medial and lateral to scan the entirety of the muscle belly and note the transition to the edge of the obliques. The rectus displays a linear fibrillar echo pattern of hypoechoic contractile tissue bounded by bright anterior and posterior sheaths. Tendinous intersections appear as thin echogenic bands that traverse the muscle at intervals. Above the umbilicus, the posterior sheath is typically present; below the arcuate line it is absent—a normal transition that should not be mistaken for a defect.
The addition of dynamic muscle contraction can be used to assess for normal or altered muscle contractile ability, demonstrating disrupted fibers, and also helps to examine the consistency of muscle tissue along the length of the RA.21,22
Pathologic Findings in Rectus Abdominus Injury
-
Intramuscular hypoechoic muscle tissue
-
Disruption of fibrillar pattern in partial tears and ruptures.
-
Associated hematoma.
Clinical Implications for Rehabilitation Providers
MSKUS provides real-time feedback for rehabilitation professionals, facilitating early diagnosis and intervention. Key applications include:
-
Early Detection of Injury / Accurate Injury Grading: MSKUS can quickly differentiate between a strain and a more severe rupture to help guide treatment planning.
-
Dynamic Functional Testing: Rehabilitation professionals can use MSKUS during physical therapy sessions to monitor recovery and assess muscle function dynamically. Serial MSKUS imaging aids in assessing ligament remodeling and readiness for rehabilitation progression.
- Guided Interventions: MSKUS imaging assists in precision-guided injections, such as dry needling or corticosteroids for inflammation.
- Patient Education: Real-time imaging serves as a visual aid to explain the nature of the injury and set realistic expectations for recovery.
Limitations and Challenges
Despite its advantages, MSKUS cannot entirely replace MRI for complex cases. Additionally, the expertise required for optimal imaging techniques limits its immediate adoption across all rehabilitation settings.
Conclusion
MSKUS has emerged as a valuable, non-invasive tool for assessing the RA muscle, offering real-time insights into its anatomy, function, and pathology. Its ability to provide dynamic imaging, high spatial resolution, and cost-effectiveness makes it particularly useful for evaluating abdominal wall injuries, hernias, diastasis recti, and post-surgical changes. By enabling accurate diagnosis and guiding treatment planning, MSKUS plays an important role in clinical practice and rehabilitation settings. As imaging technology advances, MSKUS will likely continue to expand its applications, reinforcing its position as a first-line modality for the evaluation of RA–related conditions.
Scan Demonstrations

Patient Positioning
The patient is positioned supine with a small pillow under the head and knees flexed 30–45° (hooklying) to relax the anterior abdominal wall. Ask the patient to breathe quietly; measurements are best taken at end expiration with minimal transducer pressure. Expose from the xiphoid to the pubis. For dynamic tasks (head-lift/curl-up, cough, Valsalva), rehearse cues before imaging to ensure consistent effort.
Figure 1A: Transducer Placement for Rectus Abdominis in Long Axis (LAX)
To obtain a LAX view of a rectus belly, place a high-frequency linear transducer parallel to the muscle fibers, centered ~2–3 cm lateral to the LA at the level of interest (e.g., 2 cm above the umbilicus). The transducer marker faces cranially. Slide cranio-caudally to visualize tendinous intersections and the anterior/posterior rectus sheaths (note posterior sheath disappears below the arcuate line). Optimize depth so the posterior border of RA sits in the lower third of the image; set focal zone at or just deep to the posterior sheath.
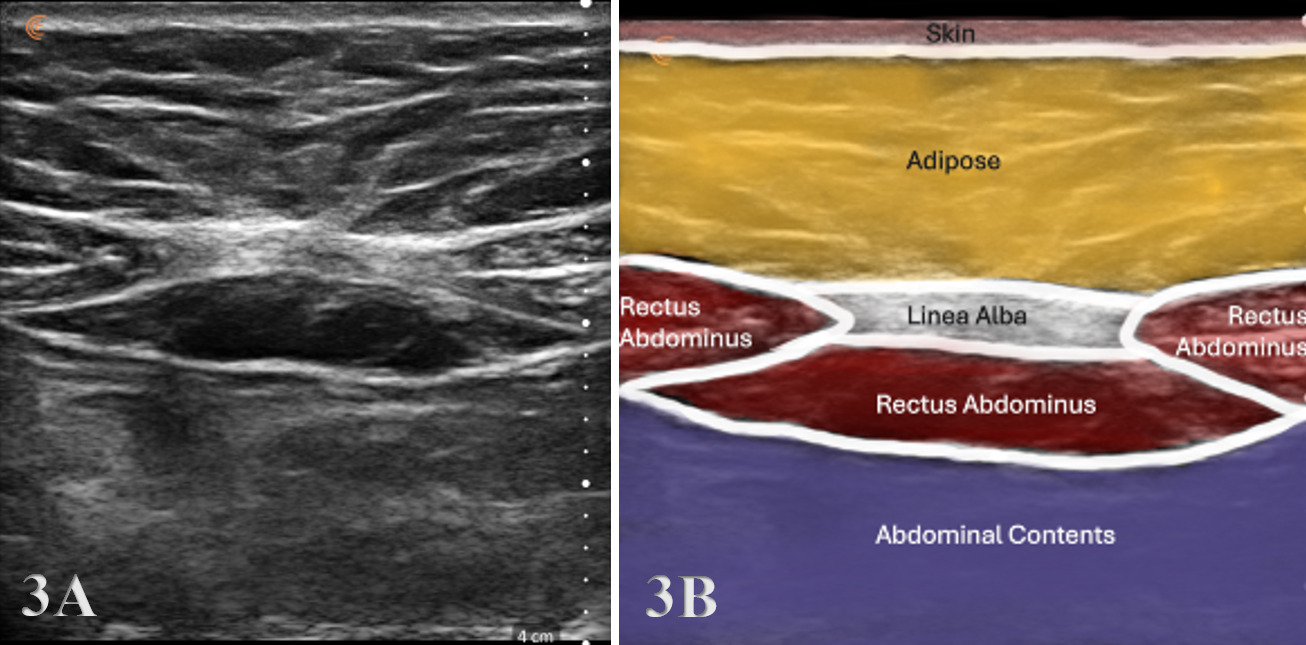
Figure 1B: Transducer Placement for Rectus Abdominis in Short Axis (SAX)
To obtain a SAX view, rotate the transducer 90° with the marker toward the patient’s right and center over the LA at the chosen level (−2/0/+2 cm relative to the umbilicus). Identify the echogenic linea alba midline, paired RA bellies on either side, and their sheaths.
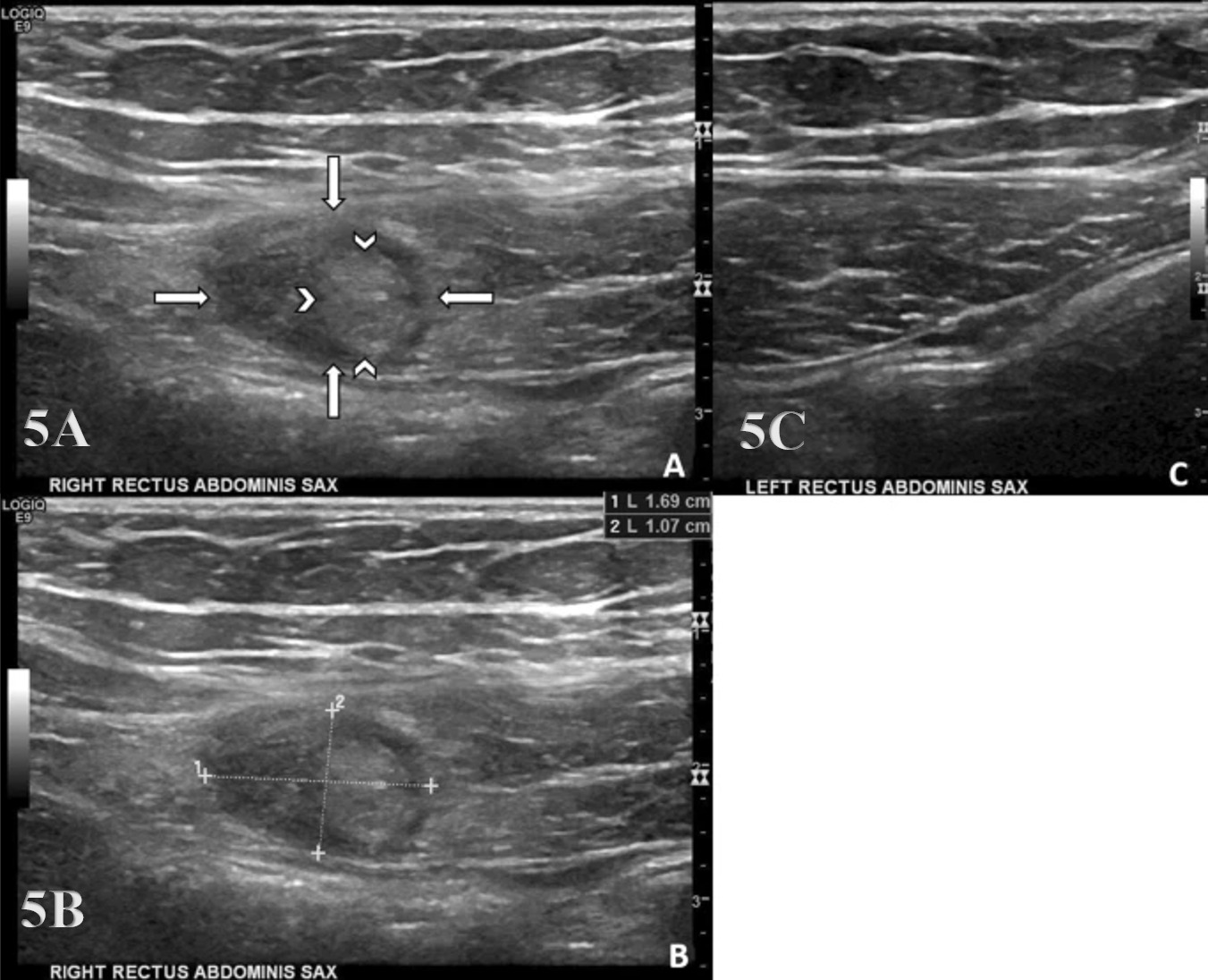
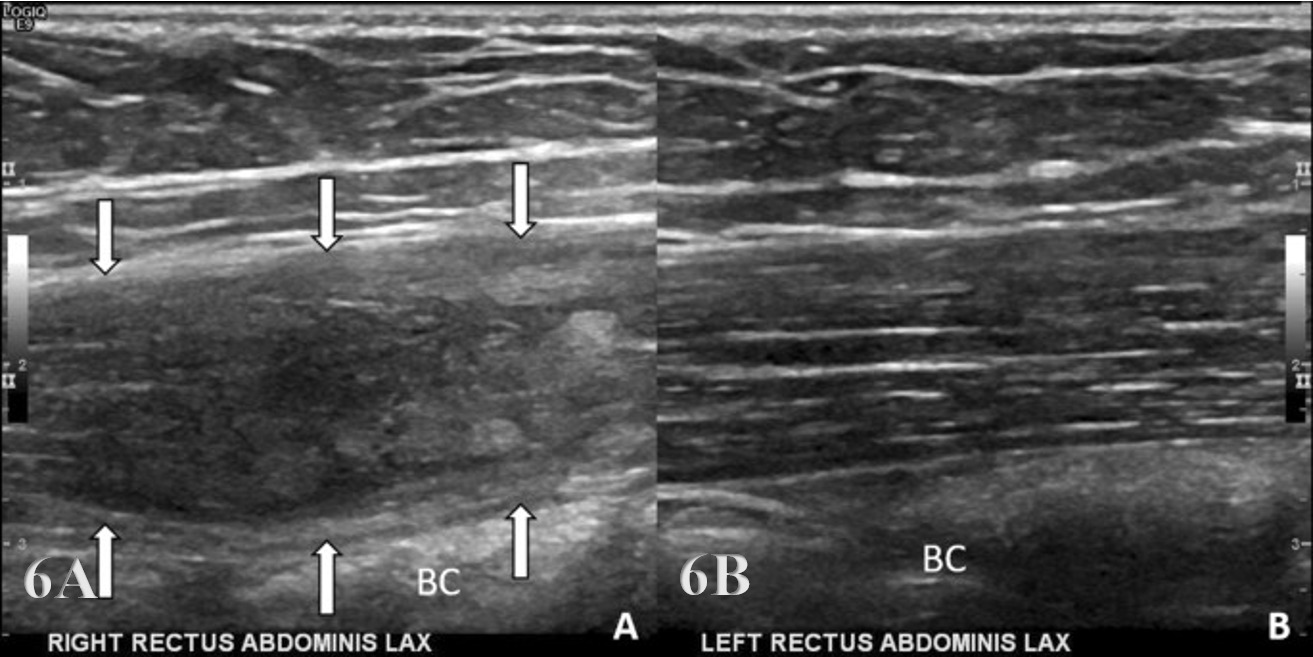
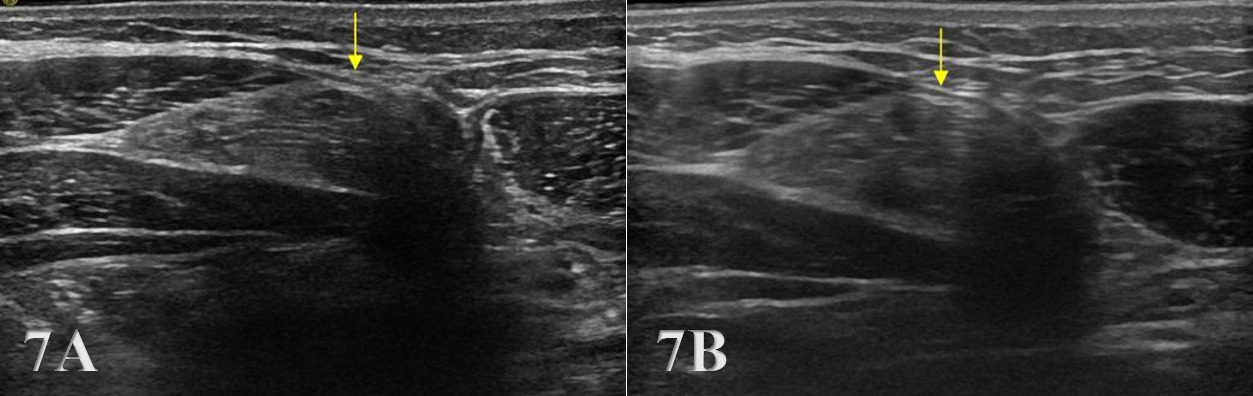
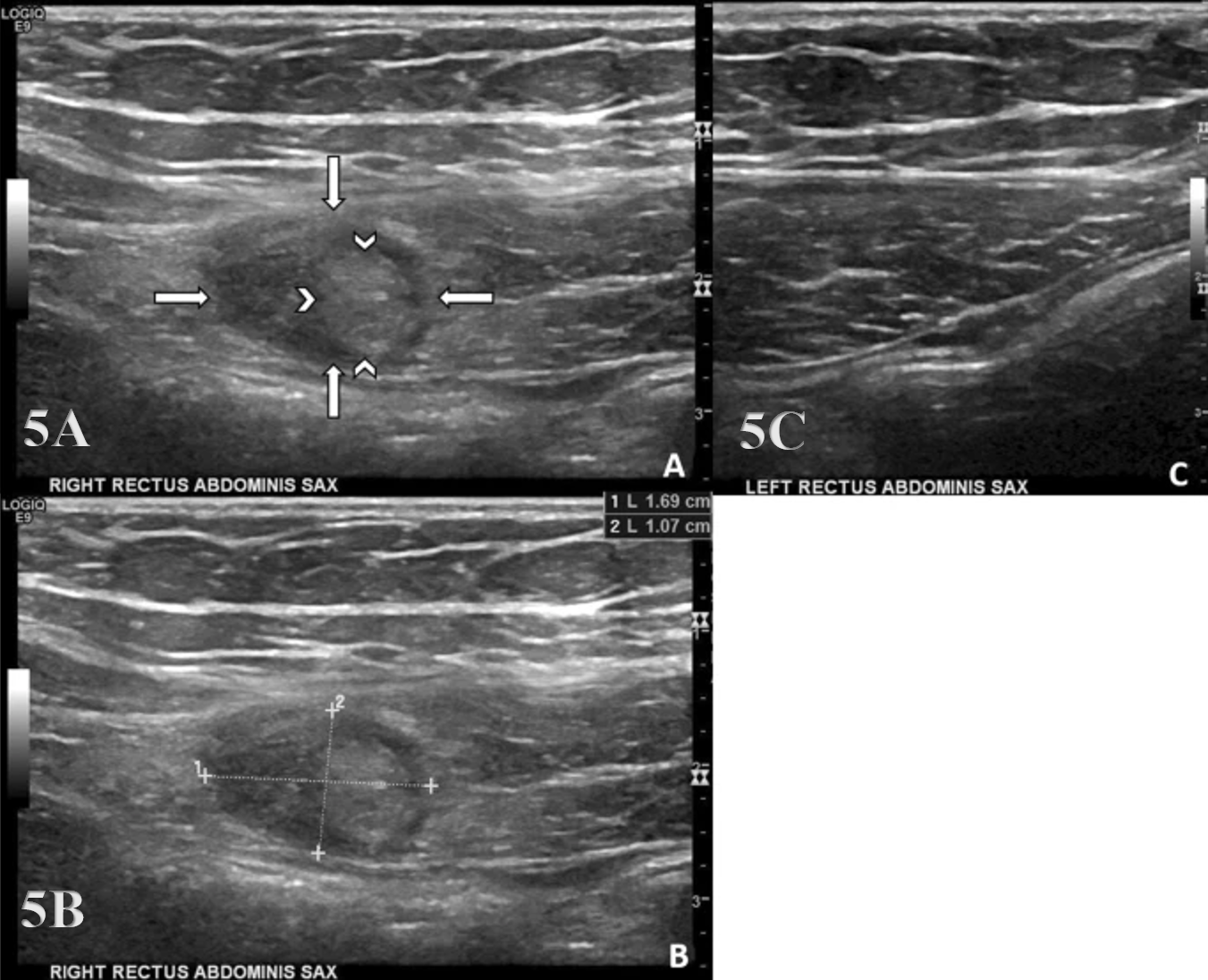
Normal Rectus Abdominis

Pathology of Rectus Abdominis
.png)