
INTRODUCTION
The Olympic Games are the largest sporting event in the world, with thousands of athletes competing during the Summer Games. The occurrence and nature of injuries in elite athletes, as well as the sports in which they suffer these injuries during major sporting events have been extensively reported.1–5 The total injury rates at the recent Summer Olympic Games were reported in Rio de Janeiro 2016 (8%),3 Beijing 2008 (10%),1 and London 2012 (11%).2
Injury epidemiology is crucial because it provides the scientific base for preventing and mitigating injuries by identifying risk factors, describing patterns of injury, and evaluating treatments effectiveness. For these reasons, several countries have conducted epidemiological studies during major sporting events. Yoon et al.6 characterized the injuries suffered by athletes from the Korean delegation who participated in the Rio 2016 Olympic Games. Two hundred and four athletes competed in 24 sports and suffered 150.9 injuries, with boxing being the sport that presented the most injuries. Furthermore, they found that 51.9% of the injuries occurred in the lower limbs and 24.0% occurred in the upper limbs. Another epidemiological study carried out among elite South Korean rowing athletes, who participated in high-level international competitions and were prepared by the Korean National Training group, revealed that more than half of all the injuries were considered minor and severity of injury varied according to the body region, with the lower extremities being the most injured region. In both male and female athletes, injury incidence rates and severity of injury were associated with weight class.7 Grim et al.8 documented the injuries that occurred in athletes from the German delegation who participated in the Rio 2016 Olympic Games. Lower limb injuries accounted for 56.5% of the total, while upper limb injuries accounted for 14.8% of the total. Lopes et al.9 studied the profile of treatments performed at the Physical Therapy Department of the Brazilian Olympic Committee during the 2007 Pan American Games through a study of 434 athletes referred by the Medical Department to the Physical Therapy Department. The majority of athletes in the Brazilian delegation required physical therapy treatment (65.7%). The main complaints observed were spinal injuries (low back pain, back pain, and neck pain) (n=89, 25.3%), tendinopathies (n=79, 22.4%), and muscle tension (n=43, 12.2%). A total of 2,523 physical therapy treatments were performed, and the most commonly used procedures were exercises (n=969, 24.9%), ultrasound (n=757, 19.4%), and cryotherapy (n=670, 17.2%). The comparison of injury rates between Olympic and Paralympic Team USA athletes competing in the Tokyo 2020 Summer Games showed that there were no differences in injury incidence (IRR, 1.18; 95% CI, 0.84-1.68) between Olympic and Paralympic athletes.10 However, when the team injury incidence at the 2022 Beijing Winter Olympic and Paralympic Games was analyzed, Olympic athletes had significantly lower injury (IRR=0.56 (95% CI 0.37 to 0.87), p=0.009) risks compared with Paralympic athletes.11 These studies reveal specific epidemiological data for the athletes representing their countries and statuses which may facilitate more focused approaches for injury prevention programs and selection of the best techniques for their treatment.
It is interesting to point out that some recently published studies have analyzed the incidence of injuries in elite athletes over several competition seasons and not just at one season. For instance, a total of 111 British Olympic track and field athletes were followed prospectively for three consecutive seasons between 2015-201823. Overuse injuries (56.4%) were more frequent than acute injuries (43.6%). The thigh was the body region most frequently injured (0.6 per athlete year), followed by the lower leg (0.4 per athlete year) and foot (0.3 per athlete year). Muscle and tendon were the most commonly injured tissues, while the most commonly detected pathologies were strains and tears. In another study, the incidence of injuries in Summer and Winter Canada Games athletes was analyzed during Canada Games competitions from 2009-201924. The injury incidence was 362.8 and 389.9 and per 1000 male and female athletes, respectively. Female athletes had 1.12 greater odds of injury compared to male athletes. Overall, injury (399.31 vs. 360.31; p < 0.001) incidences was higher in Winter Games, compared to Summer Games, per 1000 athletes. It was found that there are sex specific differences in the pattern of injuries when comparing male and female athletes participating in similar sports. All these data could be utilized for the development and implantation of injury prevention programs and injury mitigation strategies in elite athletes during major sporting events.
However, few studies have described the use of physical therapy services at major multisport events, those that did highlighted only the type of services provided by the Physiotherapy Department and the reason why athletes seek care.9,12–15 The association between athletes’ injury types and the choice of physiotherapy treatments applied was studied at the Polyclinic Tokyo 2020. Chronic injuries affecting the lower limb muscles and/or tendons were the most prevalent issues treated by physiotherapists in that study.16 The treatments preferred by Japanese physiotherapists to treat athletes were manual therapy, taping, exercises and ultrasound therapy.16 During the 2018 PyeongChang Olympic Winter Games two polyclinics that provided physiotherapy services for injured athletes were described.17 The mountain-site polyclinic was designated for outdoor sports as alpine skiing, cross-country, bobsled-luge-skeleton, snowboard, biathlon, freestyle-skiing, and ski-jump. The city venue was designated for indoor winter sports: ice-hockey, figure skating, speed-skating, curling, and short-track indoor events. The comparison between the treatments carried out in the one clinics revealed differences in the athletes’ recovery and in the frequency and percentage distribution of injuries by anatomical area. Each polyclinic attended to different populations of athletes, providing important information regarding the types of injuries and the different physiotherapy treatments used.17 Therefore, information on procedures, most commonly utilized conduct, and main injuries still lacks clarity.
Epidemiological data can contribute to planning for athlete care and contribute to the development of measures to prevent or mitigate injury.
Understanding the services provided by physiotherapists and the resources they use, as well as the most frequent sports disciplines and types of injuries, can enable professionals and researchers working in the area of prevention and treatment of sports injuries to develop protocols based on previous experiences with the aim of minimizing the occurrence of these injuries and optimizing the planning and preparation of athletes for events of this size.
Therefore, the objective for this study was to describe the incidence of injuries, the sports disciplines most affected, the body regions most frequently injured, and the procedures performed for athlete recovery by the physiotherapy department of the Brazilian Olympic Committee (COB) during the Rio 2016 Summer Olympic Games. This study also aims to provide data to better understand the physiotherapy services provided during the Summer Olympic Games.
METHODS
This study used a descriptive, observational, and cross-sectional descriptive epidemiological design to assess injuries and to analyze the actions carried out by the physiotherapy department during the Rio 2016 Olympic Games, in 2016. During Brazil’s participation, the country’s official delegation, under the responsibility of the BOC, had an exclusive team of physiotherapists among its members working together with the Medical Department.
The team of physiotherapists responsible for the Brazilian delegation consisted of 28 professionals. Brazilian physiotherapists have been improving their skills through training courses organized by the Brazilian National Society of Sports Physical Therapy (SONAFE-Brazil).18 Of these, 14 physiotherapists, accredited by the confederations of their respective sports, were responsible for providing physiotherapy services in eight sports – basketball, football, handball, judo, rugby, volleyball, and beach volleyball. The remaining physiotherapists accredited by the BOC were divided as follows: a main base in the Olympic Village with ten physiotherapists, a second one with two physiotherapists responsible for treating athletes in the handball and sailing sports, and a third one with two physiotherapists responsible for treating athletes in marathon swimming, canoe sprint, triathlon, road cycling, and rowing.
The physiotherapy treatment area in the Olympic Village was approximately 100 m2, with eleven treatment stretchers (Figure 1). Two other bases had a treatment area of approximately 50 m2, with three stretchers each. The departments operated from 8:00 a.m. to 10:00 p.m., a period that could sometimes be extended to accommodate the demands of the athletes. The service area was divided into evaluation rooms and areas for individual treatments. Treatments were performed every day at the physiotherapy department in the Olympic Village, at two other bases, and at the training and competition venues between August 5 and 21, 2016, totaling 17 days of uninterrupted care. Athletes were allowed to receive more than one physiotherapy treatment per day.

Participants
Athletes referred by the Brazilian Olympic Committee’s Medical Department to the Physical Therapy Department were considered eligible to participate in the study. Athletes who were not referred by the Medical Department to the Physical Therapy Department were not included in the study.
Procedures
The athletes were informed in advance about the project. Data regarding the type of injury, anatomical region examined, sports the athletes participated in, and the physical therapy procedures performed on the athletes during the Rio 2016 Olympic Games were extracted from their medical records. No data that could potentially violate confidentiality or identify the participant was used.
All athletes underwent a medical evaluation and were evaluated by the Physical Therapy team Brazil before beginning treatment. A clinical examination and, when necessary, an imaging exam were performed to determine the diagnosis. The Brazilian doctors received a standard table, used and developed by the International Olympic Committee, with the numerical code for each diagnosis to facilitate subsequent data accounting.19 Information for all encounters were manually entered in Portuguese on a paper form, as required by Brazilian law.20
The diagnosis was determined by the physician, who completed a referral form to the Physiotherapy Department using these codes. With this referral, the athlete then underwent a physical therapy evaluation. The Physical Therapy Record, developed specifically for this event, was used for data collection. All treatment approaches and procedures, sports disciplines, and reasons for attendance were recorded in an Electronic Medical Record during the Rio Olympic Games.14 The data extracted from the database for analysis included: gender, age, sport, type of injury, injured body part, date and time, and physical therapy treatment performed. All this information was stored in the individual file for subsequent analysis. Sports injuries were considered to be any pre-existing or recurrent musculoskeletal complaint originating from competition and/or training that received medical attention, regardless of the possible absence of competition or training.21 The injuries considered were those reported by one of the Brazilian Olympic Committee physicians to ensure the validity of the information and a comparable data standard.
All professionals involved in these procedures underwent training sessions to complete the forms to ensure a uniform data recording standard. During these meetings, members were informed about the objectives of this study.
For data analysis, the physiotherapy procedures were grouped into manual therapy, electrophototherapy resources (microcurrent, laser, transcutaneous electrical nerve stimulation [TENS], functional electrical stimulation [FES], and ultrasound), pneumatic compression with ice (Game Ready®), dry needling, taping, and superficial heat. All procedures were performed by physical therapists. Dry needling was the physiotherapy technique used, performed by a physical therapist trained in the procedure. Exercises is operationally defined for this research as the systematic therapeutic use of movement - through active, passive, or assisted exercise - to rehabilitate athletes, restore motor function, strengthen muscles, improve joint mobility, and prevent injuries, with individualized application according to the sport and athlete’s profile.22 Each athlete was evaluated by a physician and referred for physiotherapy treatment, and each physiotherapist adopted the approach they considered most appropriate for that athlete.
Statistical analysis
A quantitative analysis of the results obtained regarding injuries, sports that athletes participated in and procedures and treatments used for the recovery of athletes was performed. The normality of the data was assessed using the Kolmogorov-Smirnov test and the statistical program used was SPSS 20.0, with continuous variables described as mean ± standard deviation and categorical variables described as number and percentage.
Confidentiality and ethical approval
This study was approved by the research ethics committee of Universidade Federal de São Paulo (approval number 3.006.632), and all members consented to participate in the study. This research was approved by the BOC. All the athletes were informed in advance about the project. No data that could potentially violate confidentiality or identify the participant was used.
RESULTS
At the Rio 2016 Olympic Games, approximately 11,238 Brazilian athletes from 39 different sports took part in the following competitions: athletics, badminton, basketball, boxing, canoe slalom, canoe sprint, BMX, road cycling, mountain biking, track cycling, fencing, football, artistic gymnastics, trampoline gymnastics, rhythmic gymnastics, golf, handball, equestrianism, field hockey, judo, weightlifting, wrestling, open water marathons, synchronized swimming, swimming, modern pentathlon, water polo, rowing, rugby, diving, taekwondo, tennis, table tennis, archery, shooting, triathlon, sailing, volleyball and beach volleyball.
Brazil had the largest number of participants in the history of Brazil’s participation in the Olympic Games: 465 athletes. Of these, 209 were female (44.95%) and 256 were men (55.05%). The average age was 27.8 ± 5.8 years. The youngest female athlete, aged 16, played table tennis and the youngest male athlete was 18 years old and participated in archery. The oldest woman was 54 years old and the oldest man 53 years old, both competing in shooting sports. Among the 465 athletes who represented Brazil at the Rio 2016 Games, 422 were referred by the Medical Department of the BOC to the Department of Physiotherapy, representing 90.7% of the total number. Among the athletes treated, 188 were female (44.55%) and 234 were male (55.05%).
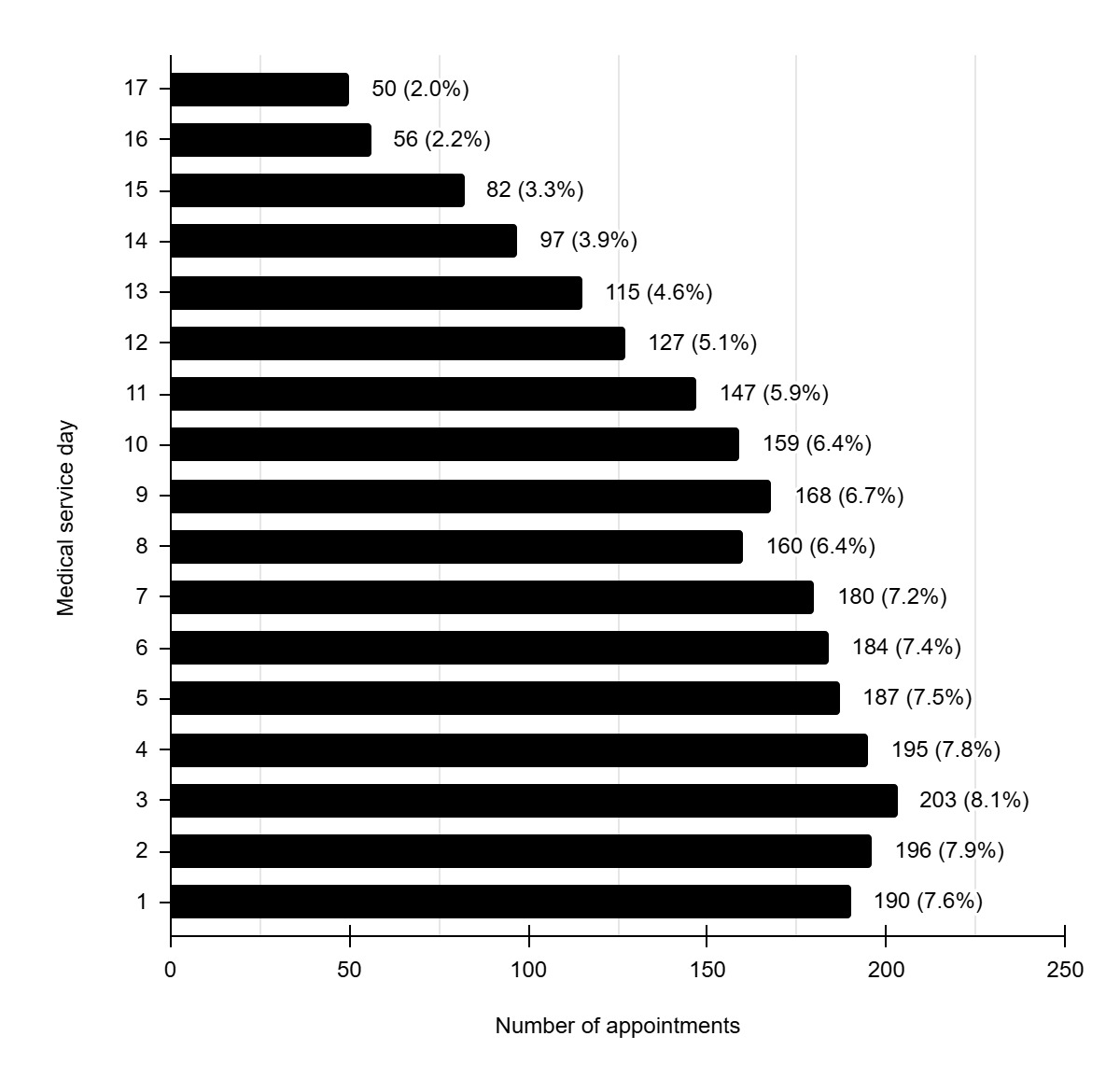
Treatments were carried out every day, between August 5 and 21, 2016, totaling 17 days of uninterrupted service, spanning more than 14 hours a day. The third day of the competition marked the peak in care (203 athletes – 8.1%). During the period in which the Brazilian physiotherapist team was working, 2,496 physiotherapy appointments were recorded, distributed throughout the 17 days of competition. The daily distribution of these services can be seen in Figure 2.
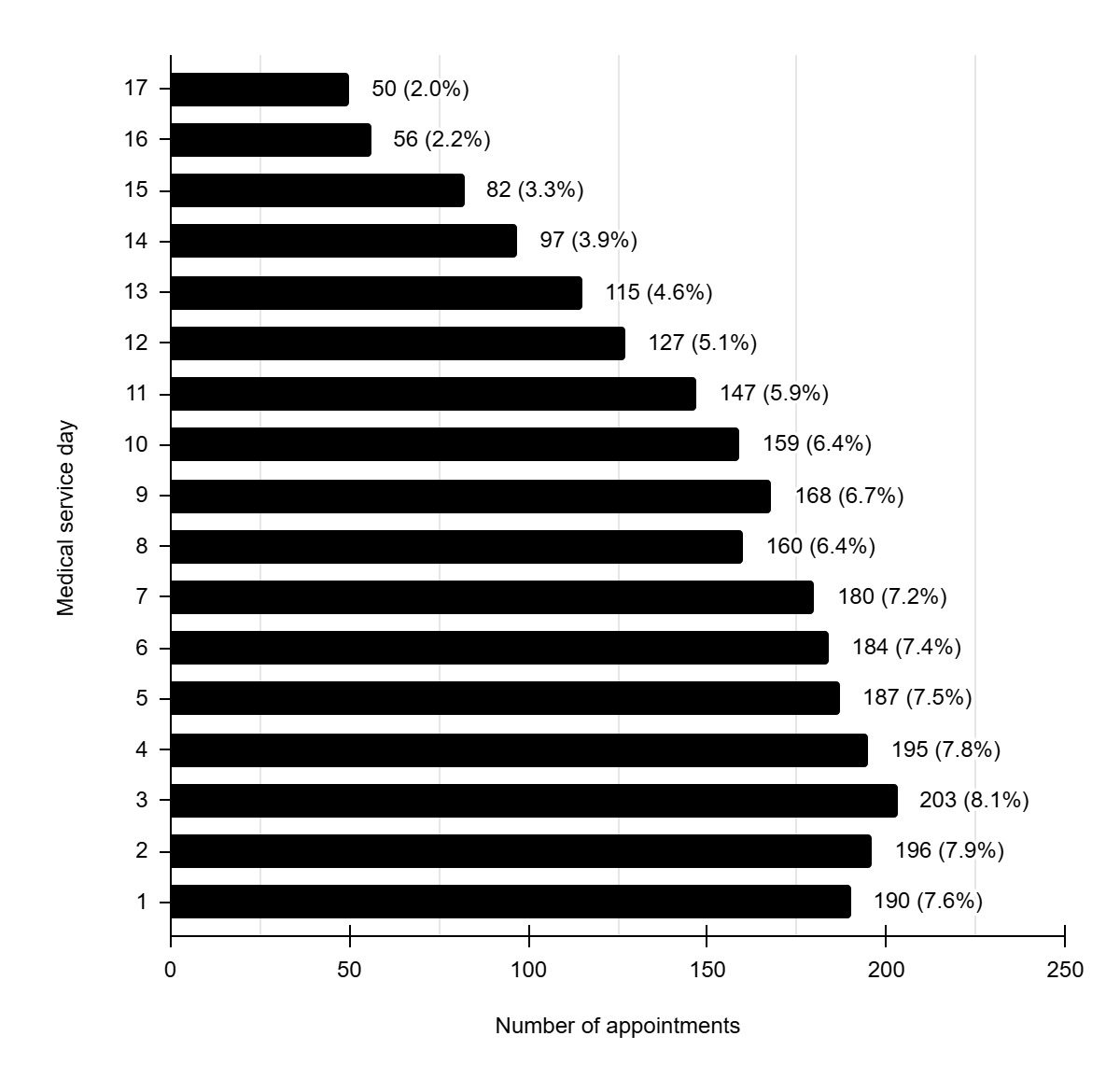
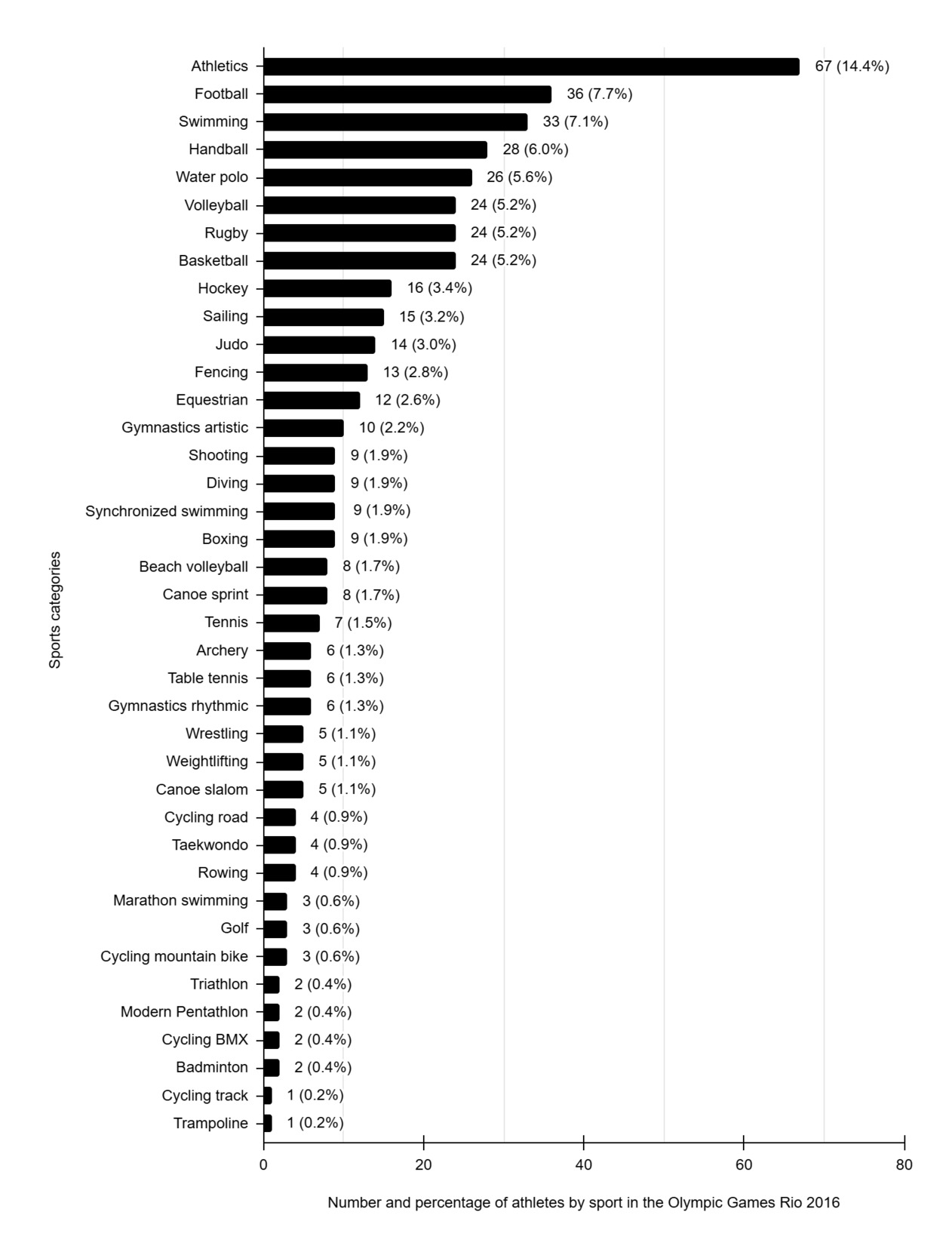
Figure 3 shows the total number of Brazilian athletes in each sport who participated in the Rio 2016 Olympic Games. The sport with the largest number of participating athletes was sports disciplines (n=67) and the sport with the smallest number of athletes was trampoline (n=1). These athletes attended at least one appointment at the Department of Physiotherapy. Injured athletes from track cycling (n=1), road cycling (n=4), triathlon (n=2), and football (n=36) were not included in this study since they were attended by physiotherapists who were team-accredited by the confederations of the respective sports.
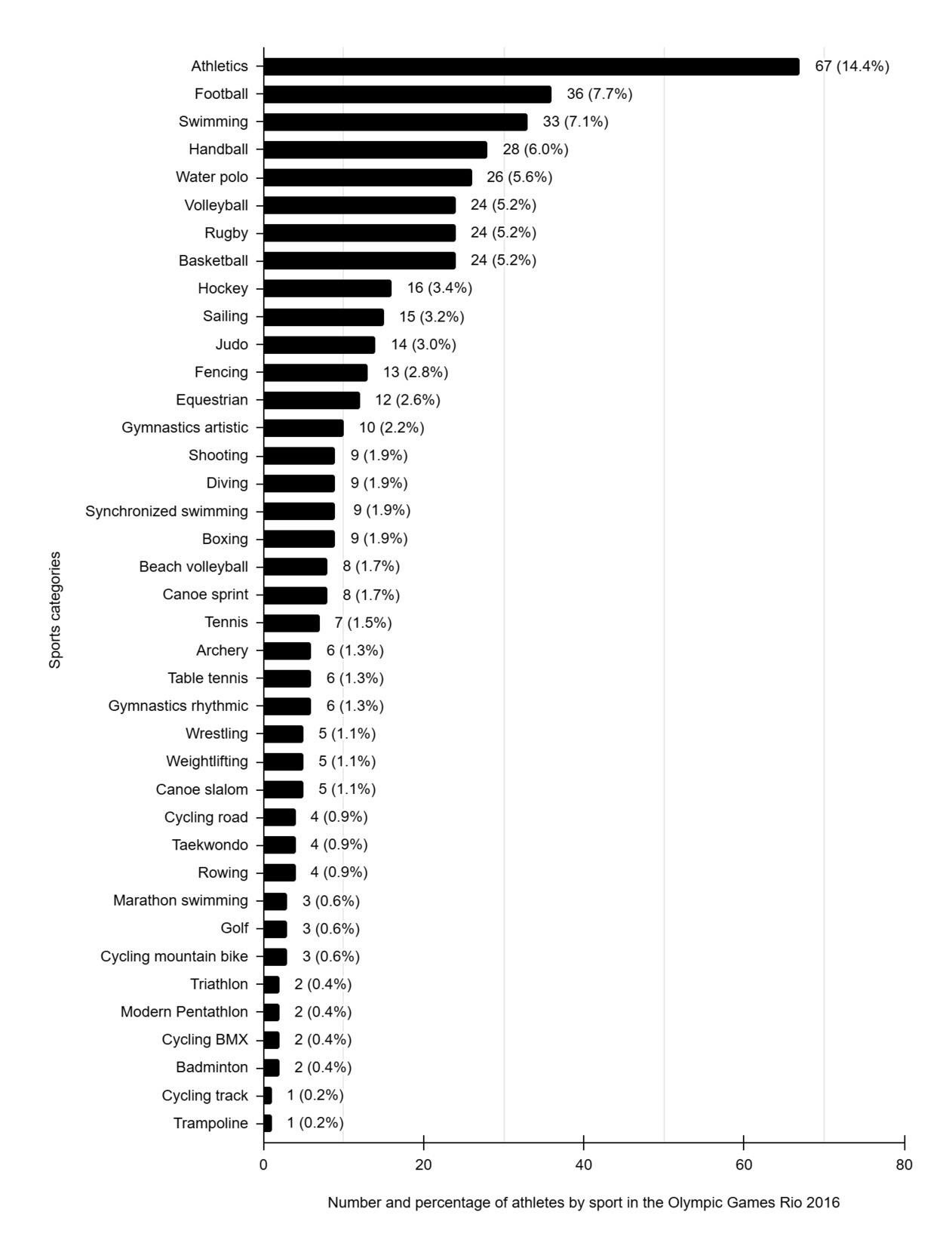
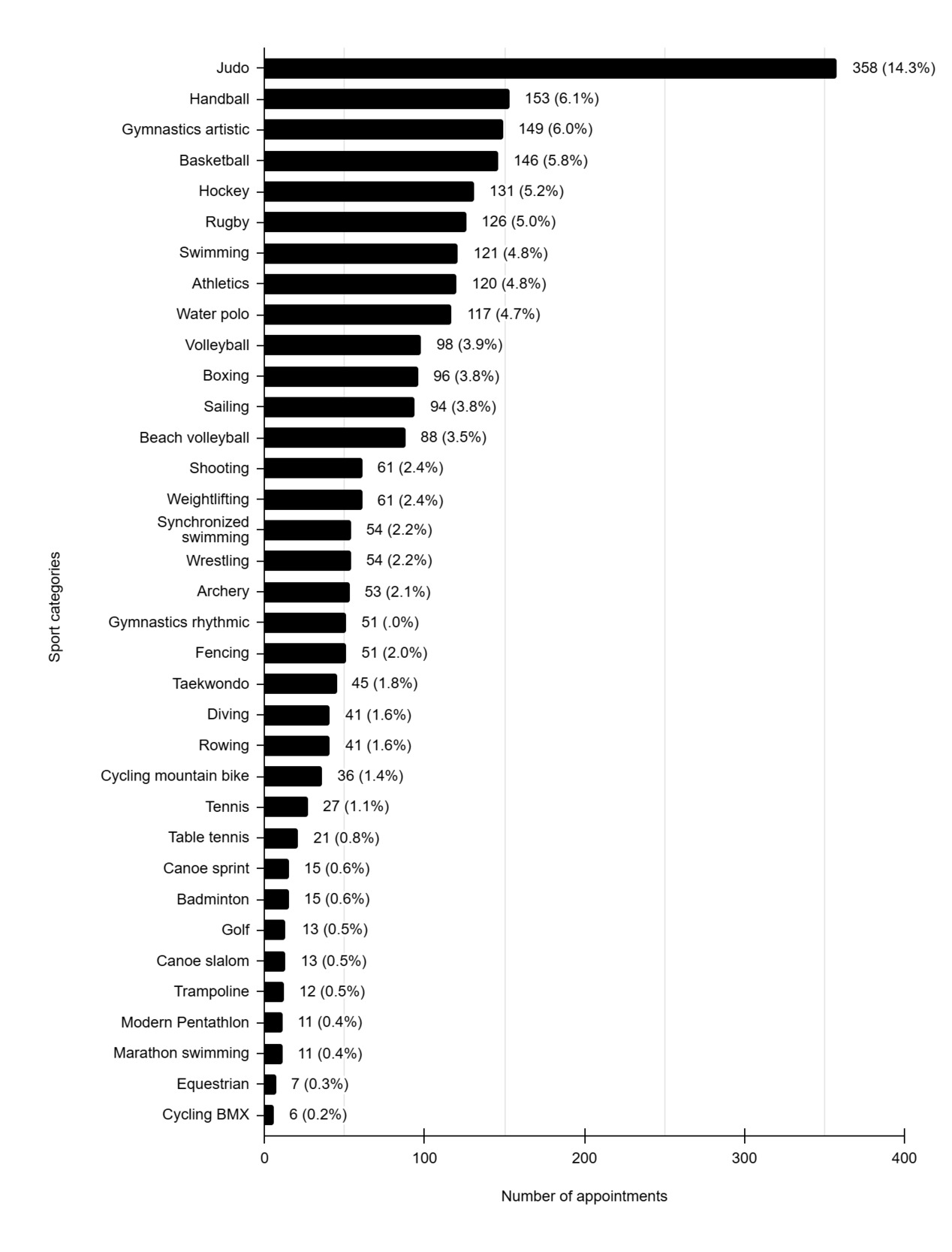
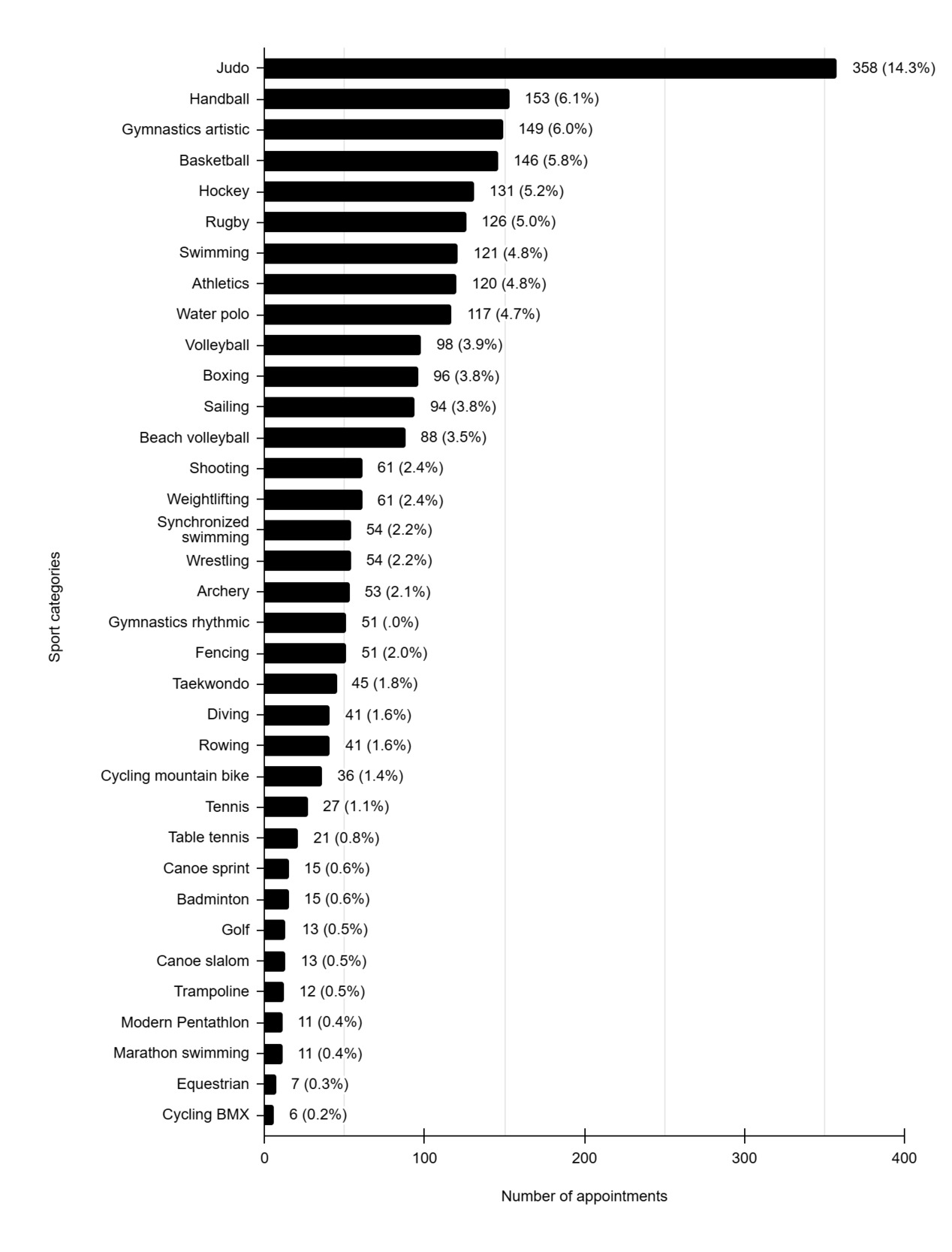
Figure 4 shows the incidence of injured athletes in each sport. The incidence of injuries was highest in judo athletes, with 358 treatments which corresponded to 14.3% of the physiotherapy team activity, followed by handball (n=153; 6.1%), artistic gymnastics (n=149; 6.0%) and basketball (n=146; 5.8%). The lowest incidence of injuries was observed in BMX cycling (n=6; 0.2%), equestrian (n=7; 0.3%), marathon swimming (n=11; 0.4%), and the modern pentathlon (n=11; 0.4%).
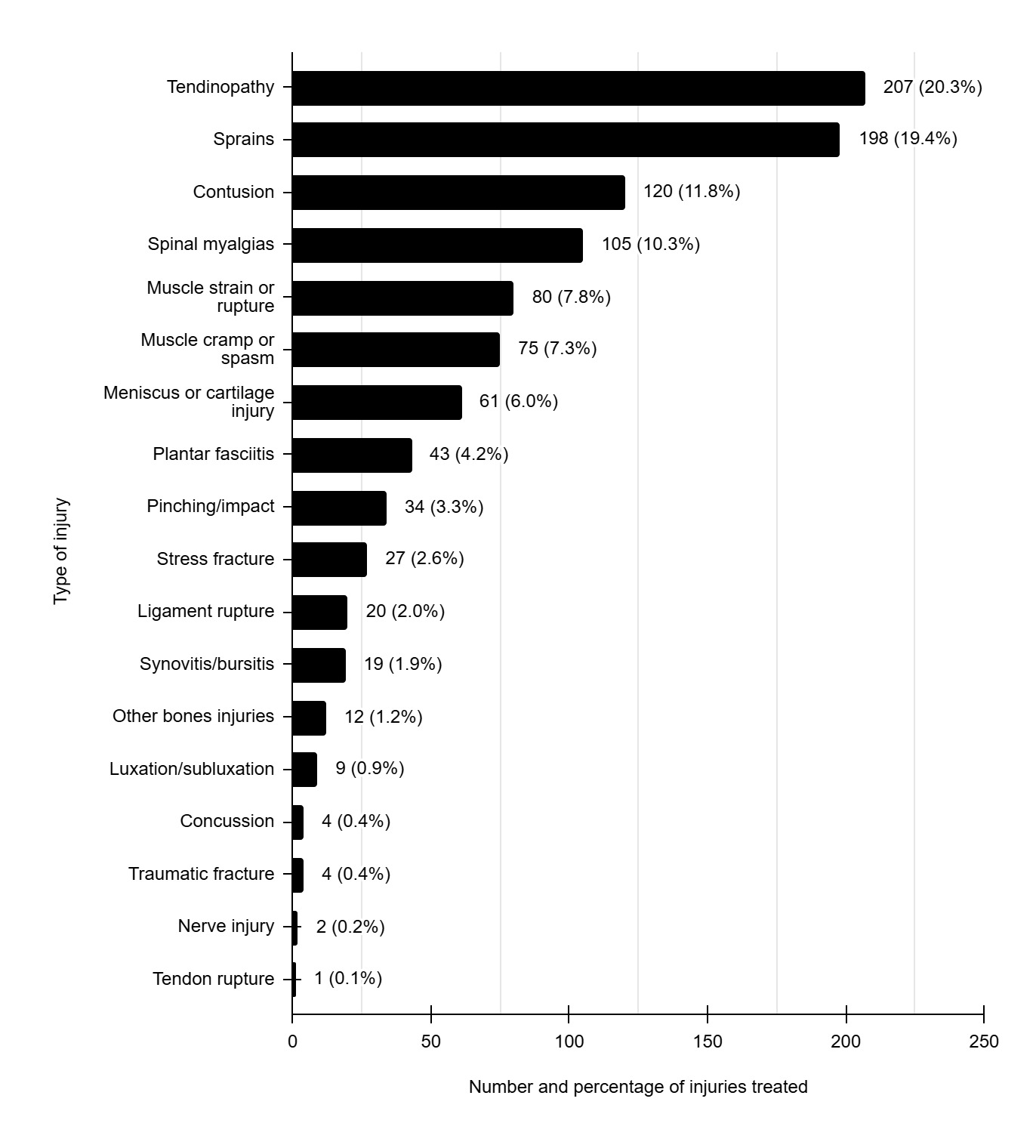
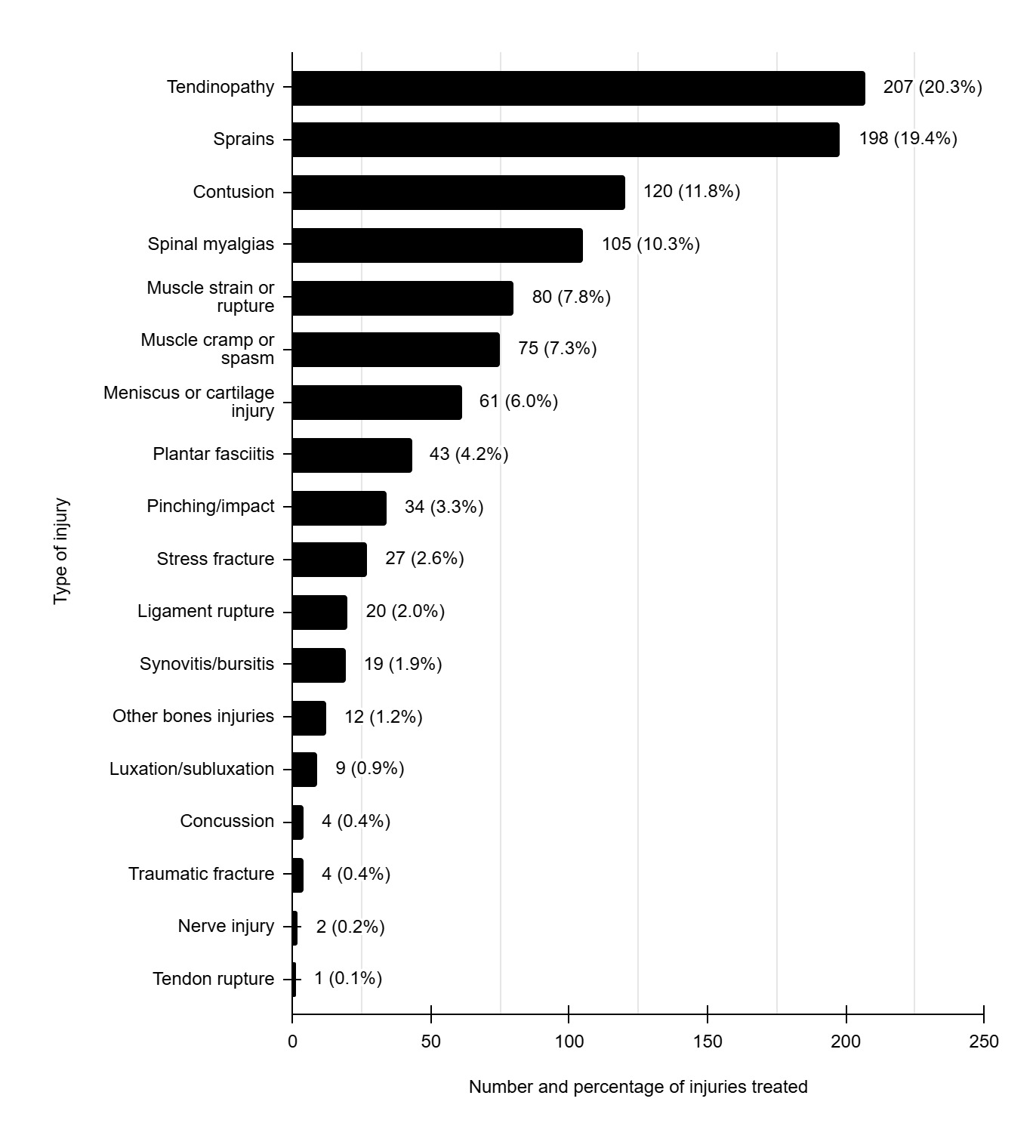
The most frequent types of injuries and the percentage of injury occurrence are presented in Figure 5. The data revealed that tendinopathies were the most common type of injury (n=207; 20.3%), followed by sprains (n=198; 19.4%), contusions (n=120; 11.8%), and spinal myalgias (n=105; 10.3%).
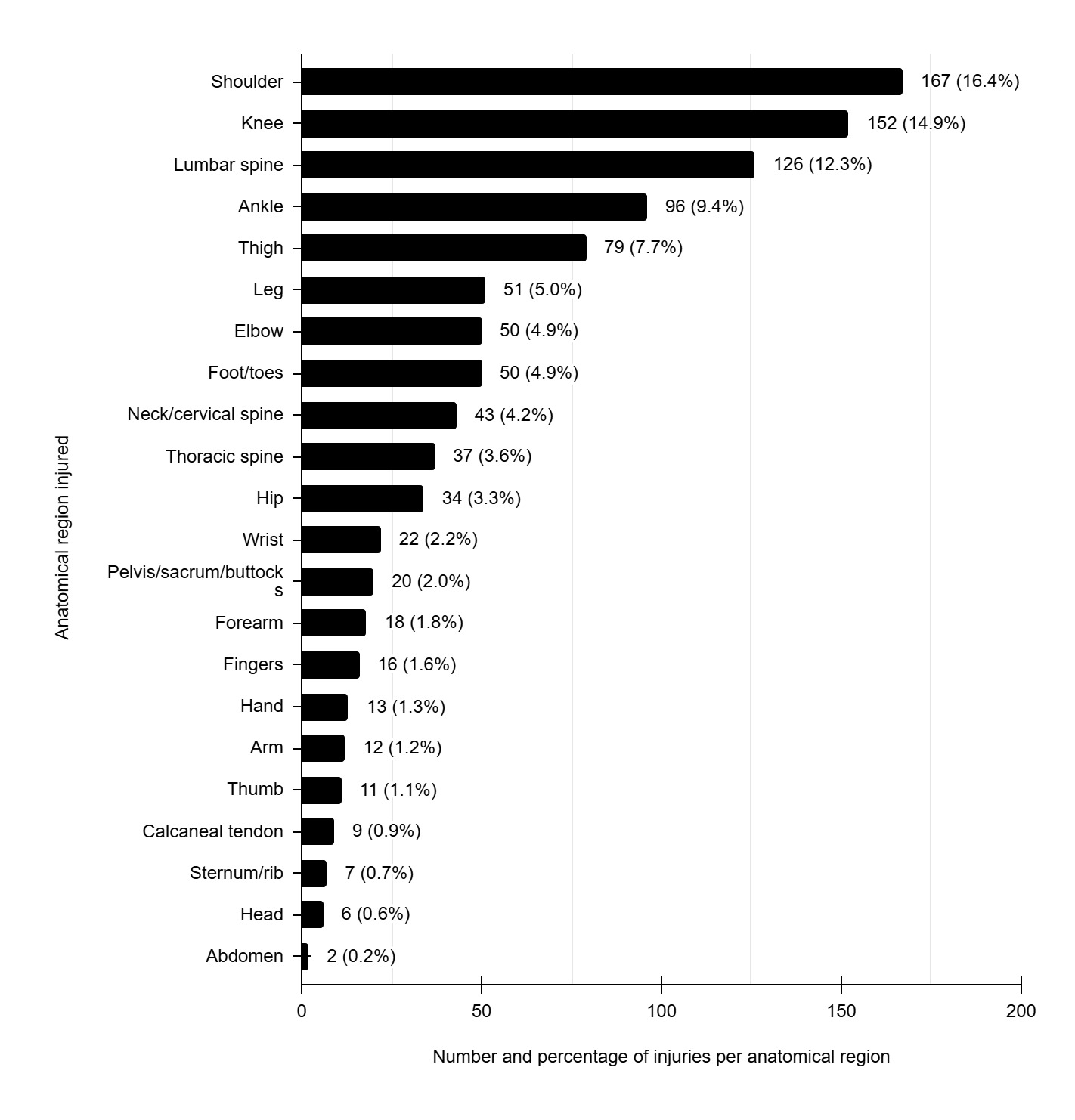
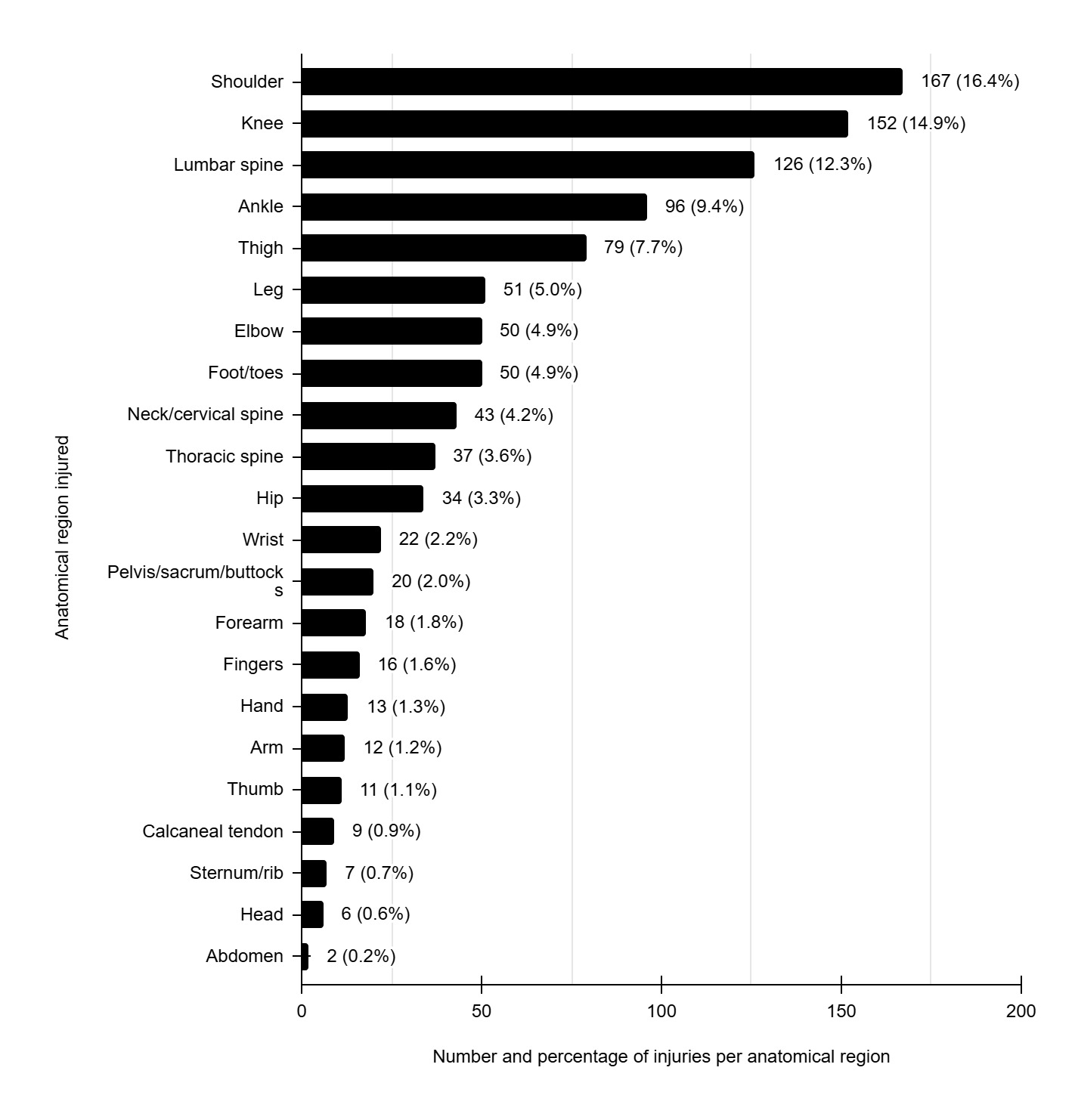
The most frequently injured anatomical areas recorded were the shoulder (n=167; 16.4%), followed by the knee (n=152; 14.9%) and the lumbar spine (n=126; 12.3%). The numbers and percentages of types of distribution of injuries by anatomical location are shown in Figure 6.
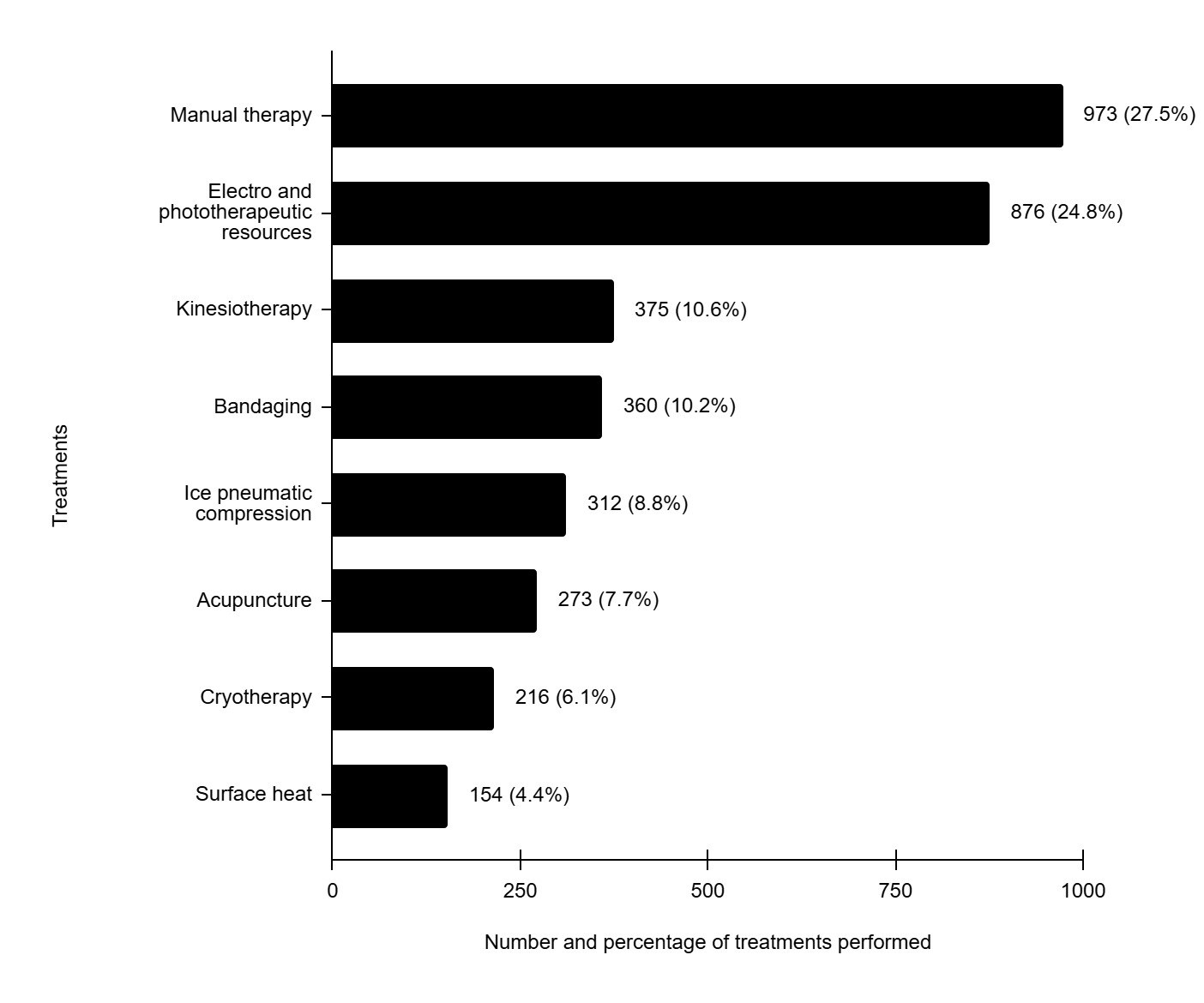
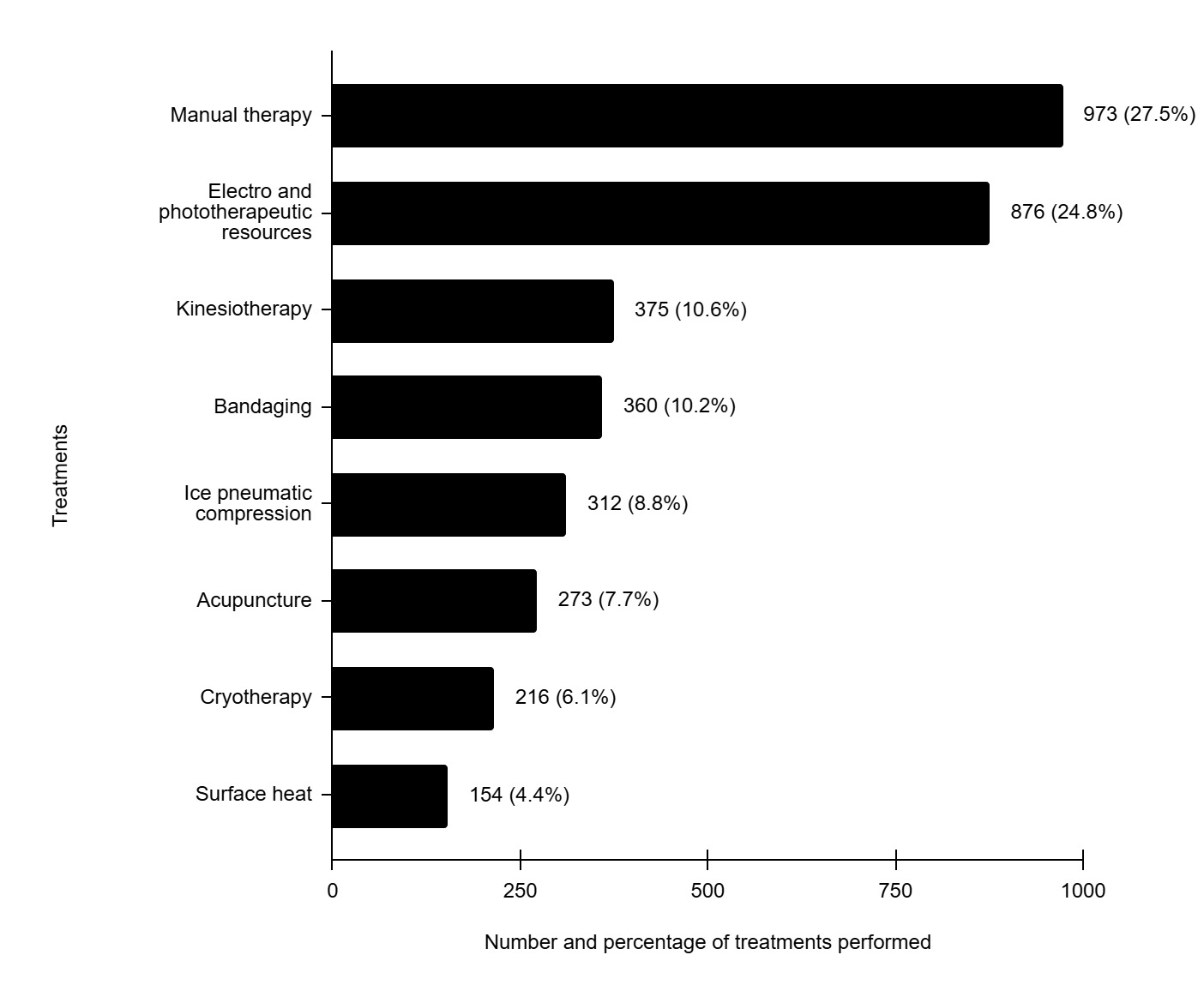
During the period of work of the physiotherapy team of the BOC, the total number of treatment sessions resulted in 3,539 physiotherapy procedures. The distribution of resources used in these procedures is specified in Figure 7. Manual therapy accounted for 27.5% (n=973) of the procedures performed, surpassing any other, followed by the use of electrophysical resources which totaled 24.8% (n=876) of the techniques applied. Other procedures used were kinesiotherapy 10.6% (n=375), bandaging 10.2% (n=360), pneumatic compression with ice 8.8% (n=312), dry needling 7.7% (n=273), cryotherapy 6.1% (n=216), and superficial heat 4.4% (n=154).
DISCUSSION
The aim of this study was to describe the athletic injuries that occurred and the corresponding sport in which they occurred during the Rio 2016 Olympic Summer Games. The physiotherapeutic procedures used to recover from these injuries were also reported.
It was found that 90.7% of the Brazilian delegation suffered some type of injury and were referred to the Physiotherapy Department, demonstrating the importance of this service’s availability at major sporting events. Athletes from judo, handball, gymnastics artistic and basketball were the most frequently treated by BOC’s physiotherapy services. Lopes et al.6 reported that during the 2007 Pan-American Games, 65.7% of Brazilian athletes received physiotherapy care. In contrast, a higher incidence of injuries was observed during the Rio 2016 Olympic Games, possibly due to the greater physical and technical demands of the Olympic competition. Moreover, athletes participating in the Pan-American Games may not have been as well-prepared or conditioned as Olympic athletes, which could also explain the increased need for physiotherapy care. In the Korean delegation at the Rio 2016 Olympic Games, 56.3% of the athletes received health attention,6 a considerably lower number than that of Brazilian athletes. Analyzing the data obtained by the International Olympic Committee (IOC), considering athletes treated at the Polyclinic of the Olympic Village or who were received treatment at the competition venues by the Organizing Committee during the 2016 Rio Games, a total of 8% of the athletes were injured.3 Previous works showed comparable values with 10% injured athletes in Beijing 20081 and 11% in London 2012.2
The number of injuries that occurred depended on the sport practiced by the athlete. The highest injury incidences were found in judo (14.3%), handball (6.1%) and gymnastics (6.0%). The differences in rate injuries according to the sport can be assigned in part to variations in the number of athletes participating in each sport - in this work, from 67 in athletics to only 1 in trampoline. The number of total days of official competitions by sport can also influence the number of injuries. Some sports competitions last just one day, while others last up to 15 days, influencing the number of injuries per sport. Considering the 11,274 athletes who participated in the Rio 2016, the proportion of injured athletes was highest in BMX bicycling, followed by boxing.3 Data from all physiotherapy services provided at the Olympic polyclinic showed, for this event, that the sports with the most injured athletes were handball (37%), followed by judo (22%), athletics (21%), and taekwondo (19%),14 data similar to that obtained in the current study. Comparing the injuries that occurred at Rio 2016, London 2012 and Beijing 2008, it was observed that some sports such as football, taekwondo and handball had many injured athletes, while other modalities such as fencing and swimming had few injuries.2,3 Most of the injuries suffered by Korean athletes during the Rio 2016 occurred in boxing (6.0%).6 There seems to be a tendency for more severe injuries in contact sports. However, it is difficult to compare different studies, since the results vary according to the group studied, the number of athletes and the sports analyzed in each case.
The most frequent injury among athletes was tendinopathy (20.3%) followed by sprains (19.4%), suggesting that overuse is responsible for the majority of sports injuries. Among all athletes participating in the Rio 2016, the most common types of injuries were sprain/ligament rupture (18.5%), contusion/hematoma/bruise (16.2%), strain/muscle rupture/tear (15.3%), and tendinosis/tendinopathy (10.2%).3 At the 2007 Pan-American Games, tendinopathy was identified as the second most frequent injury among Brazilian athletes (22.4%), followed by muscle strains (12.2%).9 At Beijing 2008, the most frequent diagnoses were ankle sprain (7.3%) and thigh strain (6.8%).1 In general, the type of injuries most commonly attended by physiotherapy services in different sporting events are comparable and most involce muscle, tendon, and ligament.
The most frequently injured anatomical regions were the shoulder, followed by the knee, lumbar spine and ankle. When the anatomical regions were grouped by lower extremities (LE) or upper extremities (UE), it was found that LE were responsible for 42.8% of the treatments, while the UE accounted for 30.3% of the treatment. These results are consistent with those observed by Soligard et al.8 who, when analyzing the injuries of all athletes participating in Rio 2016, showed that LE injuries were responsible for 39.2% of the care in physiotherapy services. In the Rio Olympic Games LE injuries in German athletes accounted for 56.5% of all injuries and the UE injuries for 14% of the total.8 Similarly, Korean athletes suffered 51.9% LE injuries and 24% UE injuries during the Rio Olympic Games.6 In Beijing 2008, the LEs were also the most affected region (54.2%).1
Therefore, it appears that most injuries consistently occur in the LE.
The most commonly involved tendons in athletes who participated in the Rio 2016 were in the shoulder,23 which is similar to those results described for London 2012.24 These data are consistent with those obtained regarding Brazilian athletes in this study. Localized elbow injuries reported during London 2012 showed a high percentage of tendinopathies involving the tendons of this region.25 This type of injury occurred mainly in combat sports athletes, such as judo, boxing and wrestling, and in weightlifting athletes. Taken together, these data are quite similar to those obtained in the present study, since tendinopathy was the most frequent injury, with judo athletes being the ones who most sought care at the physiotherapy service, and the shoulder being the most affected anatomical region.
During major sports competitions, there is usually a greater demand for medical care to focus on symptoms and handling of injuries, in order to ensure the athlete’s prompt recovery and the return to competition as quickly as possible. The types of treatment most used in the physiotherapy service were manual therapy, electrothermal/phototherapy resources and kinesiotherapy. The physiotherapists who provided care at the BOC had training, qualifications, and professional experience in manual therapy, but it is important to point out that during the 2007 Pan American Games, the most commonly used methods for treatment of Brazilian athletes were exercise (kinesiotherapy) (24.9%) and ultrasound (19.4%).9 In London 2012, the most commonly used resources were massage (23.3%), ultrasound (12.2%) and cryotherapy (10.6%).13 A recent study using data from all athletes who participated in Rio 2016 showed that the most commonly used treatments were manual therapy (40%) followed by electrotherapy (36%).14 The differences in the therapeutic resources used reflect the changes that have been made over time, seeking to use more modern and less invasive recovery techniques. It’s important to note that the physical therapists in the Brazilian delegation had different backgrounds and skills, so no specific type of manual therapy was used. Each professional used the technique they deemed most appropriate for each treatment.
Isometric exercises are indicated for the treatment of all athletes who presented tendinopathy as a pathology but are considered a long-term intervention. However, during the Olympic Games, athletes typically do not remain at the competition venue for the entire duration of the event. In practice, athletes remain at the venue according to the calendar of the sport in which they will compete, that is, they arrive at the start of the event and when their participation comes to an end, they return to their home country of origin. Thus, athletes are guided to perform isometric exercises and undergo long-term treatment to conform with best practices. However, short-term measures are utilized to minimize the athlete’s pain so that they can compete in the Olympic Games. Long-term treatment is expected to be undertaken by the athlete upon return to their home institution. Isometric exercises were counted as part if kinesiotherapy.
A methodological limitation of this study may be related to the assessment form. This form was filled out by medical professionals who, despite the training received, may have made mistakes during completion, presenting inaccuracies. In the future, studies should present an independent evaluator who records the procedures performed in order to have an impartial opinion in order to eliminate possible distortions.
Physiotherapy care is rarely the main focus of articles published on injuries in elite athletes at the Olympic Games.26 Typically, these studies focus on anatomical location, incidence, and types of injuries. The challenge for physiotherapists is therefore to determine how these data can be used to choose, among the range of available resources, which should be used in practice during these events to obtain the most effective results.
Accumulated evidence indicates that injuries vary substantially between different sports, demonstrating the need to adapt preventive measures to the context of each sport. An event such as the Olympic Games provides a unique sporting competition environment from which valuable information can be obtained about the injuries suffered by elite athletes who are at the peak of their physical and sporting development. Injury data can assist in planning health care before and during the event season. The mechanisms of injury occurrence and the risk factors associated with each Olympic modality should be analyzed in future studies for the development of effective prevention or mitigation strategies, as well as to optimize the diagnosis, treatment, and recovery of athletes during the various sporting events.
CONCLUSIONS
The results of this study indicate that 90.7% of the Brazilian athletes (n=422) who took part in the Rio 2016 Olympic Games sought care at the physiotherapy department. Judo, handball, artistic gymnastics, and basketball were the sports that most utilized physiotherapy services the most. The most commonly treated injuries were tendinopathies, sprains, contusions, and spinal injuries. The shoulder, knee, lumbar spine, and ankle were the anatomical regions most affected by injuries. The most frequent treatment procedures utilized by the physiotherapy service were manual therapy, electrophototherapeutic resources, and exercise (kinesiotherapy).