INTRODUCTION
Population aging increases the prevalence of sarcodynapenia–a decline in strength, muscle mass, and function–which raises the risk of falls, dependence, and mortality, posing a major public health challenge.1 Resistance training is one of the most effective strategies to preserve function, improve quality of life, and prevent disability in older adults, including using high-intensity protocols.2 In this context, elastic bands have emerged as an accessible and effective alternative, especially in settings lacking conventional equipment.3,4 Their versatility, low cost, and adjustable resistance support adherence and autonomy, making them particularly suitable for older populations.5 Recent studies confirm their efficacy in enhancing functional, cardiovascular, and neuromuscular outcomes.6–8
Monitoring intensity is critical for adjusting workload and reducing injury risk in older adults, particularly those with low effort tolerance.9 The OMNI-RES elastic band (OMNI-RES EB) scale is a validated and practical tool for estimating intensity during elastic band training, enabling safe load adjustments without specialized equipment or maximal tests.10 The application of the OMNI-RES EB scale was validated by Colado et al.10,11 in both young and older adults as an indicator of whether the resistance used was appropriate for the intended objectives, based on the target number of repetitions, grip width, and the color (resistance) of the elastic band. However, this monitoring only allowed for resistance adjustments after completing the set, which may have resulted in the set being performed with a load that was inadequate for the intended objectives. Consequently, adjustments in grip width or band color were required in the following set to meet the prescribed criteria. Assessing perceived exertion from the first repetition (RPE-1) may help anticipate internal load and improve exercise prescription. Although preliminarily studied in young adults,12–14 the validity of RPE-1 in older populations remains underexplored and lacks support.
Studying electromyographic (EMG) activity during sets to failure provides insight into neuromuscular fatigue, motor unit recruitment, and physiological adaptation.15 Most research compares EMG pre-post sets or between exercises,16 but few have analyzed activation across relative set intervals (e.g., 50, 75%). This is particularly relevant in older adults, given age-related declines in motor unit number, recovery capacity, and fatigue resistance.17 No studies have assessed how EMG evolves to failure across different initial RPE values (e.g., RPE 2-8 out of 10) in this population,18 a gap likely due to safety concerns limiting failure-based protocols. Understanding peak neuromuscular activation patterns may help contextualize acute fatigue in older adults. Practically, this supports combining RPE-1 at the start of the set to guide load selection with RPE near the end of the set to determine safe termination, ensuring an adequate acute neuromuscular stimulus without relying on external loads.
In summary, although the application of the OMNI-RES EB scale is validated from a post-effort perspective, its use after the first repetition in older adults remains unexamined. Specifically, no studies have concurrently validated the OMNI-RES EB scale from the first repetition across varying intensities, assessed its reliability as a predictive tool, examined whether strength level affects RPE-1 and repetition capacity, or analyzed EMG patterns throughout a set based on initial effort levels. Thus, the purpose of this study was to validate RPE-1 during moderate-velocity elastic resistance training in physically active older adults with prior experience using elastic-band exercise, by analyzing its predictive validity, reliability, and neuromuscular and cardiovascular responses across effort levels. Specifically, the aims include to: (i) examine how four initial RPE-1 levels (2, 4, 6 ,8) affected EMG activity, repetitions, and cardiovascular responses; (ii) assess the reliability of RPE-1; (iii) analyze whether strength level influenced the RPE-1-volume relationship; and (iv) describe activation patterns across sets to failure at different initial intensities. It was hypothesized that (i) RPE-1 would reliably monitor training intensity across sessions; (ii) higher RPE-1 values would be associated with fewer repetitions and with greater muscle activation and cardiovascular responses, indicating validity; and (iii) end-set physiological responses would be similar across initial RPE levels, indicating convergence of the physiological stimulus at volitional failure.
METHODS
Study Design
This quasi-experimental study followed a concurrent-validity framework.11–13 Although several physiological and mechanical variables were analyzed, the RPE-1 served as the primary construct of interest, as it represents the perceptual metric under validation. The neuromuscular, cardiovascular, and repetition-based measures were therefore included as concurrent criteria against which to interpret and contextualize (validate) the RPE-1 responses, rather than as independent primary outcomes.
The study included one familiarization and two test sessions. Participants learned to use the OMNI-RES EB scale and to relate the tension generated by their chosen grip width to the corresponding RPE value during the standing military press. Based on these participant-selected values, the researchers had a starting point to provide one resistance level or another during the experimental sessions. Heart rate (HR), systolic/diastolic blood pressure (SBP/DBP), EMG activity [% root mean square (RMS) of anterior deltoid and long head of the triceps brachii], and total repetitions were recorded across four RPE levels (2, 4, 6, 8/10). The study was approved by the Human Research Ethics Committee of the University of Valencia (code: H1464018006594 and 1861154) and adhered to the Declaration of Helsinki. Informed consent was obtained from all participants.
Subjects
Twelve participants were voluntarily recruited through convenience sampling. Inclusion criteria were: (i) age ≥60 years, healthy, physically active; (ii) ≥3 months of experience with elastic band resistance training, and regular use of perceived exertion scales, specifically for reporting effort at the last repetition of a set; (iii) participants had no musculoskeletal, cardiovascular, or neurological disorders and were excluded if taking performance-enhancing drugs or experiencing musculoskeletal pain. All were instructed to avoid strenuous activity and performance-affecting substances (e.g., caffeine) within 24 hours before testing.
Procedures
During familiarization, anthropometric data were collected, procedures explained, and participants practiced sets to failure at different RPE levels using the OMNI-RES EB scale, associating grip width and band tension with perceived intensity. Participants wore light clothing and removed their shoes for measurements. Height was measured with a stadiometer (Seca T214, Hamburg, Germany; precision: 0.01 cm), and body weight and fat percentage were assessed via bioelectrical impedance (Tanita BF-350, Tokyo, Japan; precision: 0.01 kg), following standard positioning protocols. To minimize potential bias, participants were tested under controlled conditions (morning assessments, fasting state, voided bladder, and avoidance of exercise or caffeine 24 h prior to testing). The Profile of Mood States questionnaire (POMS)19 was also administered to assess baseline mood.
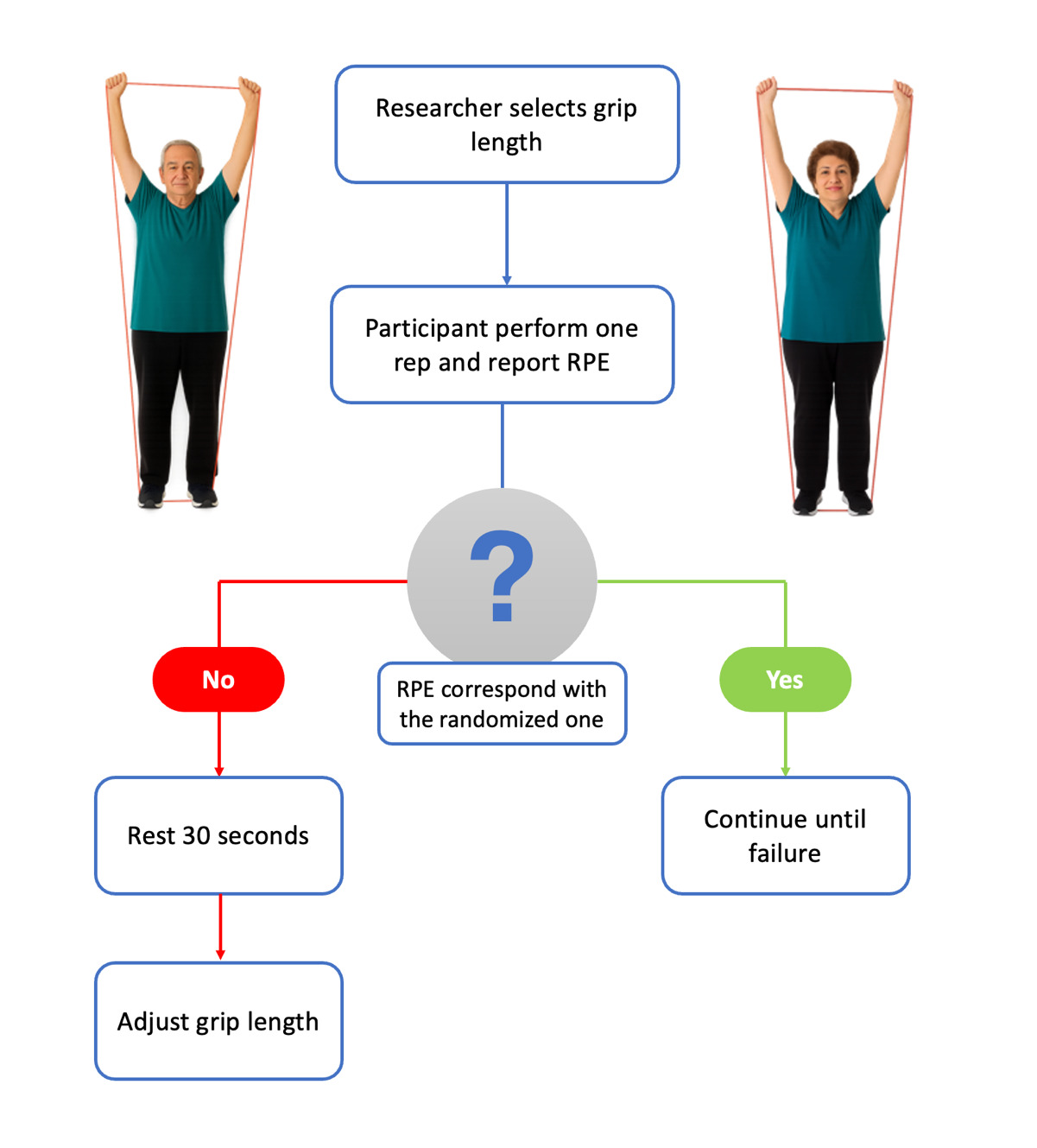
The general warm-up included 10 repetitions of dynamic mobility exercises for the upper body, followed by lower-limb and core activation exercises. A specific warm-up set of eight thrusters with elastic bands was used to activate target musculature. The thruster consisted of a front squat immediately followed by an overhead press, performed in one continuous movement using the elastic band to engage both lower- and upper-body muscle groups. Despite prior experience with RPE scales, the OMNI-RES EB was explained in detail, and a printed pictogram remained visible throughout. Participants then completed sets to failure at varying grip widths to associate band tension with RPE. RPE levels were randomized per session (via randomizer.org) and concealed to maintain blinding. At the first repetition, participants reported their perceived RPE. If the value did not match the target, the set was paused for 30 seconds and repeated with an adjusted grip until the reported RPE matched the randomized target (Figure 1).

Following familiarization, two experimental sessions were conducted to assess inter-session reliability using a standardized protocol. After warm-up, participants performed four randomized sets to volitional failure in the standing military press at RPE levels 2, 4, 6, and 8 out of 10. Each elastic band (TheraBand®; Hygenic Corporation, Akron, OH, USA) was cut from the manufacturer-supplied roll to a total length of 1.5 m, with marks drawn every 3 cm from the midpoint toward both ends to control and replicate grip width across trials. The marks were numbered to ensure symmetrical grip width and to control the grip width corresponding to a given RPE. Two band colors were used according to participants’ strength level (determined by handgrip strength) and the desired RPE: “silver” for lower resistance and “gold” for higher resistance.
Repetitions were paced at four seconds per repetition (two seconds concentric, two seconds eccentric) using a 60-bpm metronome. Total repetitions and post-set RPE were recorded. A two-minute rest was provided between sets, following prior OMNI-RES EB validation protocols.11–13
Participants’ Strength Level
Isometric handgrip strength in dominant hand was determined with a handheld dynamometer (Scacam-EH10117; South El Monte, CA, USA) as a variable of participants’ strength level. For this purpose, the arm was bent at 90°, the elbow tight against the side of the body and the wall, as well as the upper back and the glutes. The handle of the dynamometer was adjusted with the base resting on the first metacarpal, whereas the handle rested on the middle phalange of digits two to five.20 The maximum isometric effort was maintained for a maximum of five-seconds. The participants completed three attempts with three to five-minutes of rest between each one. The highest score was recorded.
Military Press Exercise
A researcher supervised all military press executions to detect deviations in technique or ROM caused by fatigue or limited body awareness. Participants were warned once; if errors persisted, the set was finalized. The exercise began at 90º elbow flexion and 75º shoulder abduction.21 Grip width was standardized via foot placement, and joint angles were verified before each set using a manual goniometer. The band was placed under both feet, and participants held one end in each hand with a pronated grip, starting each repetition from chin height. To ensure correct technique, the movement emphasized shoulder abduction (not flexion) and repetitions were only considered valid when full elbow extension was achieved. A horizontal bar was positioned at scapular height to prevent excessive trunk extension during arm elevation. For safety, bands were inspected before each set, protective eyewear was worn, and participants with abrasive shoe soles were asked to remove their shoes to avoid damaging the band. Gloves were provided if needed to improve comfort and grip.
Muscle Activation Measurement
Agonist muscle activation was assessed following Saez-Berlanga et al.21 EMG data for anterior deltoid and long head of the triceps brachii (dominant limb) were collected using a synchronized two-channel portable system (Realtime Technologies Ltd; Dublin, Ireland) with 16-bit analog-to-digital (A/D) conversion, and analyzed via the validated mDurance software22 for Android (mDurance Solutions S.L., Granada, Spain). Skin preparation followed established protocols,21 and electrodes were placed according to SENIAM guidelines and prior research.23 Bipolar pre-gelled silver chloride electrodes (Kendall™ Medi-Trace, Covidien, Barcelona, Spain) were spaced 10 mm apart, with the reference electrode on the acromion. Electrode locations were marked to ensure consistent repositioning across sessions.
Two five-second maximal voluntary isometric contractions (MVICs) were performed before the military press. MVICs followed standardized testing positions against an immovable resistance (Smith machine): for the deltoid, seated shoulder flexion at 90º without back support24; for the triceps, seated forearm extension with 90º elbow flexion.25 For consistency, EMG was normalized using the mean of the central second from the best trial.26 A practice trial ensured task comprehension, with one-minute rests and standardized verbal encouragement between trials.
EMG data were collected according to established protocols21 with a sampling frequency of 1,024 Hz. Signals were processed using a fourth-order Butterworth band-pass filter (20-450 Hz) and a 20 Hz high-pass filter to reduce motion artifacts. A test repetition ensured proper signal saturation. %RMS values were calculated for all valid repetitions, although only the first and last repetitions were included in the analysis. %RMS was also calculated for the same muscle groups across three segments of a single set (0-50%, 50-75%, and 75-100%) at distinct RPE-1 values of 2, 4, 6, and 8. EMG was interpreted strictly as an index of acute neuromuscular activation and fatigue, not as a surrogate for force production or long-term adaptation.27
Cardiovascular Variable Measurements
HR, SBP, and DBP were measured at baseline and after each set to failure using a digital wrist sphygmomanometer (Omron Electronics Iberia SAU, Valencia, Spain), placed on the left arm in a relaxed position.
Total Number of Repetitions
The number of valid repetitions was recorded by a researcher and verified using mDurance software.
Statistical Analyses
Statistical analyses were performed using SPSS (IBM SPSS v28.0.1.1(14), Armonk, NY, USA). Sample size (n=10) was estimated with G*Power software (v3.1.9.3) to detect an effect size of 0.5 with 80% power (α=0.05), r=0.5, and non-sphericity correction = 1, based on pilot data.12,13 Normality was confirmed via the Shapiro-Wilk test. A one-way repeated-measures ANOVA assessed the effect of RPE-1 (2, 4, 6, 8 out of 10) on repetitions, HR, and blood pressure. The median split technique was used for handgrip strength (i.e., baseline participants’ strength level). A two-way mixed ANOVA included strength level (low <32.41 vs. high >32.41, based on median handgrip strength) as a between-subjects factor. A three-way repeated-measures ANOVA evaluated the influence of intensity, repetition (first vs. last), and muscle (deltoid vs. triceps) on %RMS, with strength level also included in a subsequent model. A two-way repeated-measures ANOVA evaluated the influence of RPE-1, and segment of the set (0-50%, 50-75%, and 75-1005) on %RMS. Partial eta squared (ηp²) was reported as effect size (small <0.04; moderate 0.04-0.13; large >0.13).28 Pairwise differences were explored using post-hoc Minimum Significant Difference tests.
Additionally, a linear regression was conducted using RPE-1 to predict total repetitions. Reliability was calculated for %RMS, repetitions, HR, SBP, and DBP using the intraclass correlation coefficient (ICC). ICC values were interpreted as low (<0.50), moderate (0.50-0.75), good (0.75-0.90), or excellent (>0.90), based on the lower confidence interval bound.29 Results are presented as mean ± standard deviation (SD), with significance set at p≤0.05.
RESULTS
The baseline characteristics of the volunteers (six women and six men) are presented in Table 1. Participants were categorized according to their isometric handgrip strength into either a lower (<32.41kg) or higher (>32.41kg) strength level. Six participants were classified in the lower-strength group and six in the greater-strength group. The POMS questionnaire indicated a moderate mood state (scores 21–40, per classification norms), suggesting adequate psychological readiness for study assessments.
Criterion Variables for Concurrent Validation
Table 2 presents the %RMS achieved at RPE values of 2–8 during the first and last repetition in the anterior deltoid and long head of the triceps brachii. ANOVA results revealed that RPE value significantly influenced %RMS (F~(3.00, 16.22)~=10.48, p<0.001, ηp²=0.54). However, no statistically significant interactions were found when analyzing strength level × RPE value. Regarding repetition moment (first vs. last), a significant effect was observed on muscle activation (F~(1.00, 8.00)~=14.41, p=0.004, ηp²=0.62). The interaction between strength level and repetition moment did not show significant effects on muscle activation.
Table 3 presents the relationship between the pre-exertion intensity level of the OMNI-RES EB scale (values 2-8) and the total number of repetitions performed, both overall and stratified by participants’ strength levels. ANOVA results revealed that RPE value significantly influenced total number of repetitions (F~(3.00, 24.00)~=29.15, p<0.001, ηp²=0.74). These significant interactions also remained when adjusted for participants’ strength levels (F~(3.00, 24.00)~=2.53, p=0.050, ηp²=0.24).
Table 4 presents the relationship between the pre-exertion intensity level of the OMNI-RES EB scale (values 2-8) and the analyzed cardiovascular variables. There were no significant interactions between cardiovascular variables and the pre-exertion intensity level of the OMNI-RES EB scale including heart rate (F(3,24)=1.10, p=0.364, η²=0.11), systolic blood pressure (F(3,24)= 0.64, p=0.595, η²=0.07), diastolic blood pressure (F(3,24)= 0.53, p=0.667, η²=0.06). Similarly, no significant interactions were observed when adjusting for participants’ strength levels: heart rate (F(3,24)= 0.14, p=0.934, η²=0.02), systolic blood pressure (F(3,24)= 0.96, p=0.428, η²=0.11), diastolic blood pressure (F(3,24)= 0.89, p=0.460, η²=0.10). No significant post-hoc pairwise comparisons were found.
The internal consistency of the values obtained from all variables across different sessions showed a good to excellent reliability (%RMS ICC = 0.86, 95% CI = 0.82-0.89, p<0.001; total number of repetitions performed ICC = 0.94, 95% CI = 0.89-0.97, p<0.001; heart rate ICC = 0.85, 95% CI = 0.70-0.92, p<0.001; systolic blood pressure ICC = 0.91, 95% CI = 0.83-0.95, p<0.001; diastolic blood pressure ICC = 0.84, 95% CI = 0.70-0.92, p<0.001).
The simple linear regression analysis assessed the relationship between intensity OMNI-RES EB and the total number of repetitions performed. A significant negative Pearson correlation coefficient was obtained (r = -0.71, p<0.001), indicating an inverse association between the two variables. The regression model was statistically significant (F = 44.95, p<0.001), explaining 50% of the variance in the number of repetitions (adjusted R² = 0.501). The estimated regression equation was: Repetitions = 26.74 – 2.45 * intensity, where the negative slope suggests that for each unit increase in perceived exertion intensity, the number of repetitions decreases by 2.45 units (B = -2.45, p<0.001). The standard error of the estimate was 5.66, indicating the dispersion of observed values relative to the regression line. Residual analyses confirmed a normal distribution and the absence of collinearity issues (VIF = 1.00), supporting the model’s validity. The Durbin-Watson statistic (2.13) suggests independence of errors. Overall, these findings confirm that perceived exertion intensity is a strong predictor of the number of repetitions, demonstrating a progressive decline in repetition capacity as exercise intensity increases.
Additionally, a multiple linear regression analysis was conducted to predict the total number of repetitions performed based on intensity and participants’ strength levels. The model was statistically significant (F = 29.20, p<0.001), explaining 57% of the variance in the number of repetitions (R² = 0.57), indicating a strong model fit. Regarding the effect of intensity, a significant negative relationship was observed between intensity and the number of repetitions (B = -2.46, p<0.001), confirming that higher intensity leads to fewer repetitions. Concerning participants’ strength levels, a significant positive effect was found (B = 4.16, p<0.001), indicating that stronger individuals performed more repetitions compared to weaker participants. The standard error of estimation was 5.31 repetitions, suggesting a moderate prediction accuracy. Based on the results of the multiple linear regression analysis, the prediction equation for the total number of repetitions as a function of intensity and strength level is formulated as: Repetitions = 20.58 – 2.45 * (intensity) + 4.16 * (strength level). Table 5 shows the equivalences of the dependent variables with each OMNI-RES EB score.
Table 6 presents the %RMS achieved at RPE-1 values of 2–8 across the set (0-50%, 50-75%, and 75-100%) in the anterior deltoid and long head of the triceps brachii. ANOVA results revealed that RPE value (RPE-1 of 2, 4, 6, and 8) significantly influenced %RMS of anterior deltoid (F~(3.00, 33.00)~= 53.20, p<0.001, ηp²=0.83), and %RMS of triceps brachii (F~(3.00, 33)~ = 11.96, p=0.001, ηp² = 0.52). Regarding segment of the set (0-50%, 50-75%, and 75-100%), a significant effect was observed on muscle activation (%RMS of anterior deltoid, F~(2.00, 22.00)~= 29.11, p<0.001, ηp²=0.73, and %RMS of triceps brachii, F~(2.00, 22.00)~= 30.69, p<0.001, ηp²=0.74). The interaction between RPE value × segment of the set did not show significant effects for both anterior deltoid (p=0.300), and triceps brachii (p=0.596) muscle activation.
Adverse Events and Participant Feedback
No injuries or adverse events occurred during any of the study sessions. Some participants reported mild and transient muscle soreness in the deltoid and triceps regions after the testing sessions, which resolved within 24–48 hours without requiring medical attention.
DISCUSSION
The findings of the present study support the suitability of the OMNI-RES scale for monitoring elastic band resistance training in older adults, given its accuracy in assessing intensity during moderate-velocity execution based on first-repetition RPE.
Concurrent Validity and Muscle Activation: Physiological Basis of RPE
RPE-1 showed a strong linear relationship with neuromuscular activation. The EMG increase across RPE levels supports the physiological validity of the OMNI-RES EB from the first repetition. EMG responses differed between the anterior deltoid (agonist) and the triceps brachii long head (synergist), likely due to the biomechanical demands of the standing military press with elastic resistance. Anterior deltoid activation rose from 48.32% at RPE-1 2 out of 10 to 61.63% at RPE-1 8 out of 10, aligning with previous findings.30 These intermuscular differences may reflect the deltoid’s primary role in shoulder flexion and abduction,31 while the triceps assists elbow extension with lower activation32 (27.33% at RPE-1 2/10 to 41.47% at RPE-1 8/10). Triceps variability may reflect compensatory strategies in older adults prioritizing stabilization and efficiency.33 Unlike constant loads (e.g., free weights), elastic bands provide variable resistance that increases with stretch, peaking near the end of the concentric phase.14 Both muscles showed increased activation with higher RPE-1, confirming prior observations.
The current findings are consistent with results of previous studies reporting that activation increases significantly from first to last repetition across intensity, reflecting fatigue-induced recruitment, with up to 20–30% more activation at failure versus the first repetition.34 In this study, activation rose by 27.69% (RPE-1 2 out of 10) and 22.73% (RPE-1 8 out of 10). These patterns highlight RPE sensitivity for monitoring effort and intra-set fatigue.13 The link between narrower grip width, reported higher exertion, and EMG supports this method for intensity regulation in older adults.
RPE as a Predictor of Training Volume
Monitoring intensity in resistance training is critical for safety and efficacy in older adults.9 Traditionally based on %1RM, this approach is time-consuming, strenuous, and may be unsafe for this population.35 Moreover, novices often yield inaccurate 1RM values, compromising prescription. In contrast, RPE scales provide an effective, practical, and accessible alternative.12,13,36 Their validity in elastic resistance training for older adults is well-established, with correlations equal to or greater than those in aerobic contexts.11,37 Notably, participants in the present study were already familiar with elastic-band exercise and RPE, which reduced the inaccuracy commonly seen in novices. The use of RPE-1 has emerged as a promising strategy, allowing early load adjustment and repetition prediction, thus minimizing fatigue and injury risk.12
Recent findings confirm a significant inverse correlation between RPE-1 and total repetitions, as RPE-1 increases, repetitions decrease.11,37 This pattern aligns with previous results seen in younger, trained individuals.12,13 A narrower band grip –reflecting higher resistance– raises RPE-1 and reduces repetitions.12 This responsiveness makes RPE-1 a robust tool for load monitoring, comparable to fixed-load conditions where higher %1RM limits repetitions and raises exertion.38
The modulation of this relationship by baseline strength levels has been examined. Older adults with greater strength (>32.41 kg handgrip) tend to complete more repetitions across all RPE-1 levels. However, significant differences between strength groups are mainly evident at low intensities (e.g., RPE-1 2 out of 10), diminishing at higher levels (RPE-1 4–8 out of 10). This suggests that, while stronger individuals can tolerate greater volume, perceived effort converges as intensity increases –possibly due to greater local fatigue or a more refined mind-muscle connection that limits repetitions despite superior capacity.39
The utility of RPE-1 as a prescriptive tool in elastic band resistance training lies in its capacity to facilitate individualized load adjustment by enabling practitioners to efficiently match training volume to each participant’s capacity through the evaluation of a single repetition, thereby minimizing fatigue and expediting load selection.12 It facilitates: (i) differentiation of intensity levels during elastic resistance training; (ii) accurate prescription by linking specific RPE-1 values to target repetition ranges (e.g., RPE-1 of 6 for a 10–15 repetition); and (iii) longitudinal monitoring, as a lower RPE-1 for the same grip width reflects positive adaptation.12,14
In summary, the reliable OMNI-RES EB rating for the first repetition offers a cost-effective alternative to complex methods. It effectively monitors training intensity during elastic resistance exercises for older adults, providing coaches, therapists, and trainers with a practical tool to optimize loading and promote adherence in this population.
Reliability of the Protocol and Cardiovascular Safety
The present study confirmed high inter-session reliability, supporting RPE-1 as a reliable intensity marker in older adults who were already familiarized with elastic-band exercise and trained in the use of RPE at the last repetition. ICCs for total repetitions (0.94), EMG (0.86), HR (0.85), SBP (0.91), and DBP (0.84) ranged from “good” to “excellent”. These findings confirm protocol consistency and, in some cases, exceed previous reliability values in older adults. HR (ICC = 0.84) and repetitions (ICC = 0.94) surpassed the 0.81 and 0.79 reported by Colado et al.11 Similarly, repetition ICC also exceeded the 0.88–0.91 range reported by Colado et al.12 in younger adults. These results reinforce the utility of RPE-1 for monitoring intensity in older adults.
Cardiovascular responses (HR, SBP, DBP) did not differ across RPE-1 levels. These findings support the hypothesis that cardiovascular responses plateau during elastic resistance training when sets are performed to volitional failure, regardless of the initial intensity, load or number of repetitions. A plausible explanation is that, as observed in previous studies, reaching muscular failure elicits a relatively consistent cardiovascular response that appears to be independent of the resistance intensity or repetition count, as long as the exercise involves similar muscle mass and body regions.11,40
These results demonstrate that, in the standing military press exercise performed with elastic bands, the belief that low-resistance training automatically entails lower cardiovascular demand is inaccurate. From a physiological standpoint, acute cardiovascular response depends less on the absolute resistance used and more on the type and intensity of effort performed. Specifically, when effort approaches or reaches muscular failure, cardiovascular demands increase substantially—regardless of whether the load is low, moderate, or high. Therefore, the use of autoregulation strategies such as RPE can support safe and effective exercise dosing, tailoring intensity to the individual’s functional status and reducing the risk of unnecessary cardiovascular overload.10
Analysis of Muscle Activation Patterns throughout a Set to Failure at Different RPE-1 Levels in Older Adults
The present study contributes to analyzing neuromuscular behavior during resistance exercise to failure in older adults, using %RMS stratified by RPE-1 levels (2, 4, 6, and 8 out of 10). To date, this is the first study in this population to characterize motor unit recruitment progression across a set using elastic bands at moderate velocity. This is relevant given the scarce evidence on intra-set muscle activation in older adults and the modulation of these patterns by initial effort perception. Results showed a progressive increase in %RMS (50% to 100% of the set) for both the anterior deltoid and long head of the triceps brachii, with larger increases at higher RPE-1 levels. For example, deltoid activation rose from 47.89 ± 12.73 at RPE-1 2 out of 10 (0-50% of the set) to 61.27 ± 19.22 at 75-100% of the set, and from 63.07 ± 13.48 to 76.44 ± 19.68 at RPE-1 8 out of 10. These findings likely reflect progressive motor unit recruitment in response to intra-set fatigue, consistent with physiological principles of sustained submaximal effort.41
These data support the hypothesis that fatigue can induce high muscle activation even at low initial RPE, provided the exercise is performed to failure.42 This observation has practical relevance at the acute level, as it enables an adequate neuromuscular stimulus without increasing external load–a key advantage among older adults for whom high loads may be contraindicated.5 Importantly, this interpretation refers to acute internal load and neuromuscular effort, not long-term strength or hypertrophy adaptations. Additionally, the interaction between RPE-1 and set progression suggests that initial perceived exertion modulates the neuromuscular response. This relationship facilitates individualized effort regulation and volume adjustment within a session or microcycle, based on functional status and perception, rather than implying long-term training effects. RPE-1 is a non-invasive, self-regulated indicator of internal load12 that may enhance adherence and efficacy in older adults.
A practical key finding is that, although neuromuscular activation (%RMS) increased at 50%, 75%, and 100% of the set across RPE-1 levels, the absolute gain from 75% to 100% was modest–e.g., ~3.8% at RPE-1 8 out of 10 in the anterior deltoid (from 72.66 ± 17.21 to 76.44 ± 19.68)–suggesting early termination may preserve adaptative benefits. This supports American College of Sports Medicine (ACSM) guidelines recommend submaximal intensities to maintain technique and reduce injury risk, especially in novices.43 Recent evidence also favors repetitions in reserve (RIR) strategies–stopping 2–3 reps before failure (15–25% volume reduction)42–as safe and effective, particularly for older adults or those with limitations.18,44 These methods yield comparable strength and hypertrophy gains, with less fatigue and better adherence.45 Thus, the findings validate conservative RIR-based prescriptions or submaximal RPE at the end of the set (7-9 out of 10) to balance efficacy, safety, and long-term compliance.46 Taken together, these findings support the value of intra-set EMG analysis to optimize effort dosing and training design, where neuromuscular stimulus depends not only on absolute intensity but also on accumulated fatigue and initial perceived exertion.
Limitations and Future Directions
This study has some limitations that should be acknowledged. Although an a priori power analysis was conducted to estimate the minimum required sample, the limited number of participants may still reduce statistical power and increase the risk of a Type II error; therefore, the findings should be viewed as preliminary and require confirmation in larger trials. This sample consisted of healthy, physically active older adults with prior experience using elastic bands and RPE scales, which may limit the generalizability of the findings to less active or clinical populations. Additionally, only one upper-body exercise (standing military press with elastic bands) was assessed under controlled laboratory conditions; therefore, caution is needed when extrapolating these findings to other exercises, muscle groups, or training settings. Although standardized procedures were followed, factors such as electrode placement and skin impedance may introduce variability in surface EMG. Future studies should examine RPE-1 in a wider range of exercises and populations, including older adults with different functional levels or chronic conditions, as well as evaluate long-term training adaptations and its application in real-world settings.
CONCLUSION
The first-repetition RPE obtained using the OMNI-RES EB scale has proven to be a valid, and reliable indicator for monitoring intensity during moderate-velocity resistance training with elastic bands in older adults. RPE-1 accurately predicted total repetition volume and captured the intra-set progression of muscle activation, enabling precise and efficient exercise prescription. The need to combine RPE-1 and final RPE to safely and effectively regulate neuromuscular and cardiovascular stimulus during moderate-velocity training has also been shown.
Funding
This work was funded by the AICO 2024 grant (Grants for Consolidated Research Groups; CIAICO/2023/056) from the Regional Ministry of Education, Culture, Universities and Employment of the Generalitat Valenciana, Spain. Additionally, it was supported by a predoctoral grant to Angel Saez-Berlanga (CIACIF/2021/189) from the Generalitat Valenciana, funded by the European Social Fund.
Conflict of interest declaration
The authors declare no conflict of interest.