INTRODUCTION
Approximately 200,000 anterior cruciate ligament (ACL) injuries occur annually in the United States to patients commonly in their mid-teens to early 20s. The primary treatment for these individuals is ACL reconstruction (ACLR).1–3 It is well-documented that individuals after ACLR are at increased risk to develop long term knee problems, such as early-onset osteoarthritis (OA) of the knee, with the reported prevalence ranging from 40% to 85% of patients 10-15 years after surgical intervention.4–8 Early-onset knee OA in those following ACLR is associated with significant pain, decreased quality of life (QoL), financial strain, and a significant burden on the healthcare system.9,10 The incidence of knee OA in persons following ACLR is much higher than the general population, where knee OA prevalence rates are reported from 20-24%,11,12 and typically much later in life. Thus, understanding the extent that early-onset OA of the knee is attributable to modifiable mechanisms after ACLR represents a significant clinical problem and intervention target for researchers and clinicians.
There is a growing body of knowledge linking common gait maladaptations seen in patients who have undergone an ACLR procedure and early-onset OA of the knee.13–16 Gait maladaptations, such as decreased knee range of motion (ROM), increased sagittal plane knee flexion angle at initial contact, decreased knee extension moment, and decreased vertical ground reaction force (vGRF) early in stance present following ACLR15,17 and often persist at least fivew to seven years after surgery and likely beyond.18 In the frontal plane, an increased knee adduction moment resulting in varus positioning is a common finding in this population.13,19–22This has led to emerging theories that the etiology of early onset of osteoarthritis may relate to an altered loading environment at the knee created by gait maladaptations.23–26 Because individuals after ACLR are active, even slight alterations to the loads that are experienced by the articular surfaces of the distal femur and proximal tibia and the remaining meniscus, when compounded over the course of millions of steps, may have detrimental long-term effects on knee joint health. Thus, therapeutic interventions that directly address gait maladaptations are of critical importance in the clinical setting after ACLR.
The purpose of this scoping review was to investigate the literature on therapeutic interventions after ACLR whose purpose is to normalize gait biomechanics. By identifying interventions and normalization of gait outcomes, we hope to encourage further study that leads to future implementation of effective interventions to mitigate the risk of early-onset OA of the knee, improving the long-term knee health of ACLR patients.
METHODS
Identifying the Research Question
Due to the large number of gait studies on therapeutic interventions post ACLR the search aimed to be as broad as possible using an a priori review protocol shared between co-authors (KS, SB, MI). The research question was: what therapeutic interventions are present in the literature that affect walking gait post ACLR?
Eligibility Criteria for Studies
To be included in the analysis each study must have: 1) been published between 1990 and 2023, 2) written in English, 3) conducted using human participants, 4) full text available, 5) included participants who were between the ages of 18-35 years that had undergone an ACLR procedure within five years of the relevant intervention, and 6) included outcomes measures focused on walking/gait metrics after receiving a therapeutic intervention. Exclusion criteria included, case studies, case series, wrong comparator (i.e., using gait as a training intervention but not assessing gait outcomes) and wrong setting such animal studies or human cadaver studies.
Information Sources and Search Procedures
Search terms were identified to address the purpose of the study and used to develop search strategies for six databases including PubMed, SPORTDiscus, CINAHL, Scopus, CENTRAL, Embase, (see Appendix). Main search terms centered around anterior cruciate ligament reconstruction, gait, and outcomes. Data extraction was completed in 2023 to yield a comprehensive search of existing literature related to the topic. The search (MB) and evaluation of search results were performed according to Joanna Briggs Institute (JBI) Reviewers Manual for Developing a scoping Review.27,28
Study Selection
The identified studies from the database searches were compiled into a single EndNote library and uploaded to an online systematic review program, Covidence (Melbourne, Australia). Once uploaded, duplicate studies were removed. Two independent reviewers (KS and MI) screened titles, abstracts, full texts using Covidence (Melbourne, Australia) based on inclusion and exclusion criteria. If a conflict was identified between the two initial reviewers, a third reviewer (SB) cast the final vote.
Charting the Data
Upon compilation of the list of included articles, the evaluation of the interventions and findings to evaluate pertinent dichotomies began. It was found that many used similar intervention lengths; single session, less than 12 weeks, and greater than 12 weeks. This offered a feasible means of compiling the data in chart form for a succinct report of findings.
Critical Appraisal
In this scoping review, the aim was to report on the breadth of the available published evidence regarding therapeutic interventions that affect gait after ACLR. As critical appraisals are not required by scoping reviews, an in-depth critical appraisal was not performed.29 This approach has been accepted and supported by the database of scoping reviews on health-related topics,27,30 especially in those reviews where scarce findings do not facilitate systematic review or meta-analysis.27,28
Synthesis of the Results
The final stage of the scoping review process as described by Arksey and O’Malley29 is a thematic analysis to enable the investigation of the included studies in depth to produce a thorough summary. In this thematic analysis, interventions fell into three categories: durations consisting of a single session, less than 12 weeks, or greater than 12 weeks. There was a wide array of therapeutic interventions utilized and subsequent gait evaluation metrics. This added to the complexity of the topic and highlights the critical need for further therapeutic interventions to address gait maladaptations post ACLR that are well studied and readily available in clinical settings.
RESULTS
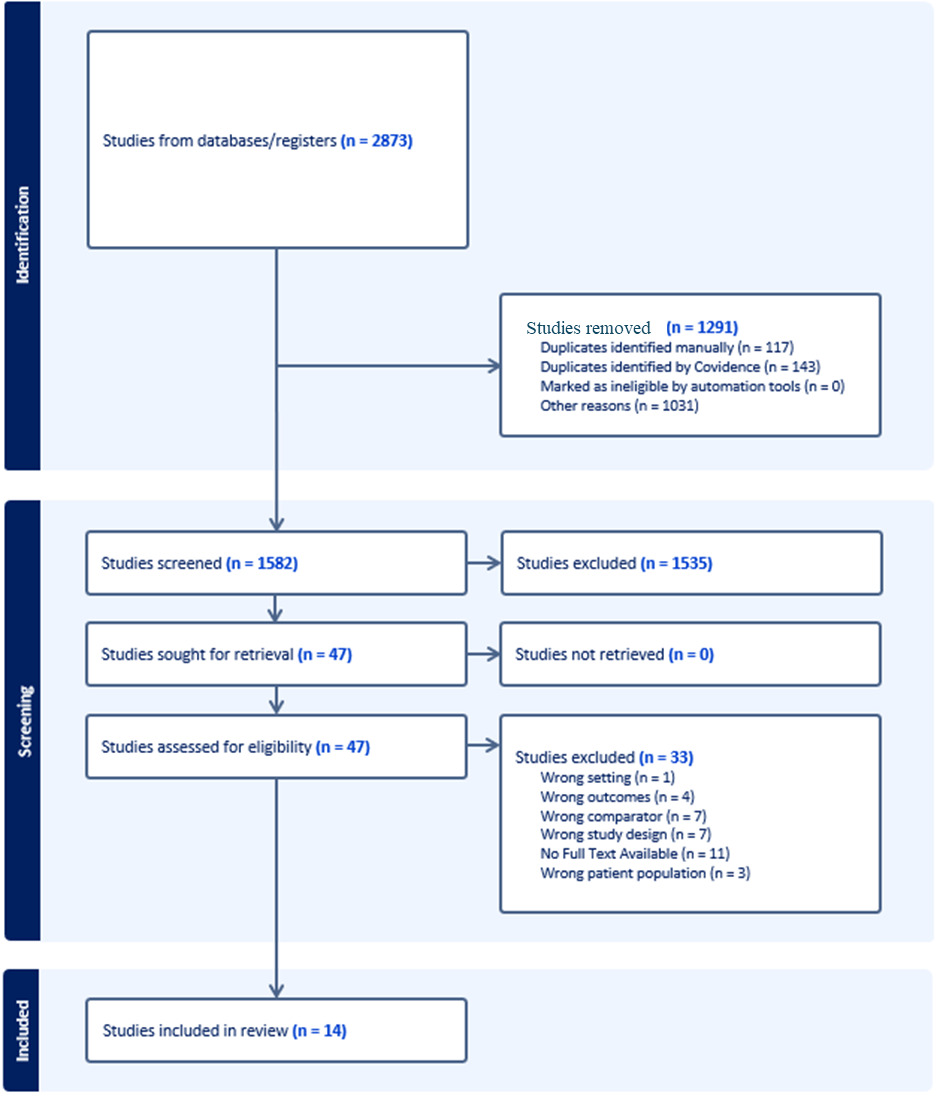
Utilizing common search terms and subsequent MeSH terms found in the Appendix, a total of 2873 articles were assessed for suitability for inclusion in this scoping review (Figure 1).

A total of 14 studies including 404 total participants (Table 1) met the eligibility requirements, with the earliest publication being from 2004 and the most recent from 2021.
Of the 14 publications, thee included a single laboratory visit31–34 while 11 were prospective intervention studies35–44 (Tables 1 and 2). Of these analyzed studies, six included targeted strengthening in addition to a normal ACLR rehabilitation protocol, two included partial body-weight gait training via a specialized treadmill, three included assistive devices used during gait or real time feedback via assistive devices, two included vibration therapy, and one included a harmonic oscillator intervention (Table 2). Among the prospective studies, the length of the interventions ranged from four weeks to six months, and the frequency of the interventions ranged from one training session per week to five days a week (Table 1). Follow-up periods were generally short for all studies (<six months), however there were three studies that provided two-year follow-up data.35,36,38 Four of the 11 prospective intervention studies resulted in a positive change in knee range of motion and/or knee joint kinetics.37,39,42,44 Of interest, only one of the four studies used walking as the training modality,39 while the other studies focused on neuromuscular training,40 knee extensor eccentric training37 or core stabilization45 (Table 2). We observed a variety of outcome measures utilized in these studies (Table 2). They ranged from “low tech” clinical tests (TUG, 10-m walk) to more high-tech instrumented tests (3D motion capture, EMG).
DISCUSSION
The purpose of this review was to perform a scoping review to investigate various therapeutic interventions after ACLR to specifically normalize gait biomechanics. Fourteen studies that satisfied the inclusion and exclusion criteria were included. Those investigations used a range of interventions. The mechanics of walking, given its central role in performing activities of daily living, likely plays a key role in an individual’s long term knee health and the reported altered loading cycles that occur each step for those with ACLR have been hypothesized to contribute to EOA.46,47 While this provides a motivation to identify modifiable risk factors to reduce risk of EOA, there are a limited number of evidence-based therapeutic interventions that specifically address known gait maladaptations after ACLR.
Alterations in gait can change the loading environment, with potential ramifications on the articular surface of femur and tibia, as well as the meniscus. This has led to a hypothesis that gait maladaptations alter the loading of knee cartilage after ACLR creating conditions for both overloading13,48–51 and/or underloading19,46,47,49 of the cartilage within the knee. Andriacchi et al. described the onset of OA occurring as a combination of two proposed theories. One theory proposes that individuals who adopt a high functional loading response on the knee joint develop rapid progression of OA. A second theory suggests that individuals who adapt to a low functional loading develop a slower progression of OA due to under loading.48 Another crucial component to this theory is that cartilage thickness is attributed to both joint loading and the number of loading cycles.13,52 This can be interpreted as a potential finite balance between sufficient loading cycles to encourage cartilage hypertrophy and too much loading and/or alterations in how the cartilage is loaded resulting in premature breakdown.49 This emphasizes the importance of normalizing gait as efficiently as possible as walking is the dominant cyclic activity of daily living.5,13,19,20,49
While multiple studies were identified that were able to demonstrate normalization of key features of gait at varying levels of evidence, they used a variety of interventions on a very limited number of subjects making it difficult to generalize their applicability in the clinical setting on a large scale. This identifies a need for a scalable intervention to mitigate gait maladaptations after ACLR that is feasible to apply in the clinical setting. While clinicians have shown a recognition that gait interventions after ACLR are important53 the findings of this scoping review suggest that relatively few studies exist attempting to normalize and/or assess gait after ACLR. Reducing gait maladaptations such as decreased knee range of motion (ROM), decreased knee flexion angle at initial contact in the sagittal plane and a decreased knee extension moment, and increased vertical ground reaction force (vGRF) during loading21,52,54–58 after ACLR are modifiable factors that may affect the onset of early-onset knee OA in individuals with ACLR.
While the modifiable nature of post ACLR interventions provides promise, recent work shows that while many clinicians ascribe value to gait training during rehabilitation, only 35% of respondents reported objectively measuring gait during rehabilitation.53 Furthermore, given the findings of this review, there are very few well studied therapeutic interventions that mitigate gait maladaptations after ACLR. Given the subtle nature of gait maladaptations, the use of sensitive means of quantifying pre-post changes to gait are important.59,60 The recent advent of valid and reliable means to quantify aspects of gait using 2D based camera technology,61,62 markerless multiple camera views to reconstruct 3-dimensional video capture outside the lab,61,63 or wearable technology64–66 is providing clinicians and scientists means to perform these quantitative assessments in clinical settings.
Many of the included studies demonstrated significant variation in the type and focus of the therapeutic interventions used to address altered gait, including focus on proprioception, eccentric strengthening, core stability, biofeedback, partial body-weight training, and joint mobilizations. To add to the difficulty of applying these interventions clinically, the studies highlighted were observed to include low standardization of timing, volumes, intervention types, and gait metrics as outcome measures. For this scoping review the authors appraised investigations that were single session studies (n=3) and prospective interventions (n=11). The single session investigations tested the effectiveness of acute interventions such as local muscle and whole-body vibration,31 robotic intervention,32 biofeedback while walking34 and anterior tibiofemoral glides.33 Each of these acute interventions led to improvements in the specific kinetic or kinematic gait outcomes with one study showing that gait modifications were still present one month post-intervention.32 It is not clear to the extent that these unique interventions would result in long term or sustained effects on knee joint kinetic and kinematics due to their single visit, cross sectional design. Some of the prospective interventions assessed showed promise at normalizing gait metrics, however the long-term efficacy of these treatments is unknown. Two investigations that reported positive findings showed promising long-term results at six months post ACLR.42,45 The short-term nature of the interventions (nine of the ten interventions lasted 12 weeks or less with limited follow-up) do not allow the assessment of implications on gait along a longer time horizon, especially pertaining to long term functional gait, as the outcome metrics were also highly variable. Of note, three investigations did assess outcomes at one- and two-year post-op. These studies failed to show meaningful improvement in these outcomes related to alterations in function of the reconstructed knee.35,36,38 These authors suggested that longer interventions may be required. Further studies standardizing interventions and evaluating the gait metric outcomes are needed before adopted into clinical practice, especially as many of these interventions are not commonly being utilized in clinical practice.53
LIMITATIONS
A limitation that may be present within this study is the use of MeSH terms that may not have aligned with translations of terms from studies written in other languages. A second limitation could be the operational definition of therapeutic interventions. For this study therapeutic intervention as a physical intervention performed by a clinician on a patient with ACLR was defined. This may have omitted other prospective interventions that, while unlikely, may have a positive effect on gait metrics such as psychological interventions or durable medical equipment such as bracing interventions.
CONCLUSION
The results of this scoping review show that few studies have tested interventions to target gait normalization after ACLR. Further, the lack of standardization of the interventions in the 14 studies, as well as variability in rehabilitation duration and follow-up assessments of the interventions give rise to an important clinical problem to address. A need is present for well-vetted and widely studied therapeutic interventions that address common gait maladaptations after ACLR to address long-term knee health in individuals with ACLR.
Conflict of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.