BACKGROUND AND PURPOSE
Over 300 million people worldwide are affected by osteoarthritis (OA) with the hip and knee being the two most commonly damaged joints.1,2 Treatment includes a wide variety of pharmacologic (pain medication or injections), nonpharmacologic, and surgical (joint replacement) options.1 Of the nonpharmacologic treatments, literature suggests aerobic exercise, exercise therapy (ET), manual therapy (MT), and physical activity (PA) are effective at improving pain and physical function.3,4 Combined MT and ET approaches have shown improvements in hip ROM.5 However, conclusions regarding multimodal approaches have shown conflicting results.6,7 Physical therapy research generally agrees that there is not a specific exercise therapy prescription for hip OA; the available evidence highlights comparable safety and effectiveness among different interventions.8
The American College of Rheumatology (ACR) in a 2023 systematic review of clinical practice guidelines reaffirmed that it is unknown which type of exercise elicits the greatest benefit for individuals with hip OA.9 Rather, the ACR recommended programs be individualized and follow the frequency, intensity, type, and time (FITT) principles.9 The American Academy of Orthopedic Surgeons (AAOS) in a 2023 clinical practice guideline for the management of hip OA recommended physical therapy as a conservative treatment option for mild to moderate symptomatic hip OA to improve pain and function.10 However, several gaps in the literature were noted including: heterogeneity in types of interventions and FITT principles, failure to stratify severity of hip OA in results or subject selection, and few studies compared a comprehensive physical therapy program to a placebo group.10
The purpose of this case report was to examine the benefits of a stratified, tailored multimodal approach for an individual with moderate hip OA. This work is important because there is no consensus among medical bodies, AAOS and ACR, and Physical Therapy bodies, American Physical Therapy Association (APTA) and Royal Dutch Society for Physical Therapy (KNGF), as to which treatment prescription will have the best therapeutic effect.
CASE DESCRIPTION: HISTORY AND SYSTEMS REVIEW
The subject of this case report was a 75-year-old male and recreational runner of more than 40 years, who presented with an insidious onset of non-localized right hip pain. The subject estimated the pain onset roughly four months prior and had progressively worsened over time. Described as a dull ache, the pain ranged from 2/10 to 6/10 and was worse in the mornings but better in the evenings. Aggravating factors included bending, entering or exiting a car, long car rides, negotiating stairs, sitting, and strenuous exercise. Non-strenuous exercise, rest and massage were alleviating factors. His body mass index (BMI) was 24.0, considered within a normal range. Previous history included right sided sciatica and bilateral medial meniscus surgeries. He worked as a freelance sales consultant and maintained a part time role as a sales associate at a local running store. He lived alone but had friends and his adult daughter as a social support system. Of note, he was taking prednisone, a corticosteroid anti-inflammatory medication, once daily for a temporary period of time aimed to reduce hip pain intensity. He had three primary goals: to decrease hip pain during activities of daily living, to increase weekly long run mileage without increasing hip pain, and to complete a half-marathon scheduled four months after the initial evaluation. No prior imaging had been done on his spine or lower extremity, and he presented with no red flags such as a personal history of cancer, bowel and bladder changes, inability to walk more than four steps, or unsteady gait.
CLINICAL IMPRESSION 1
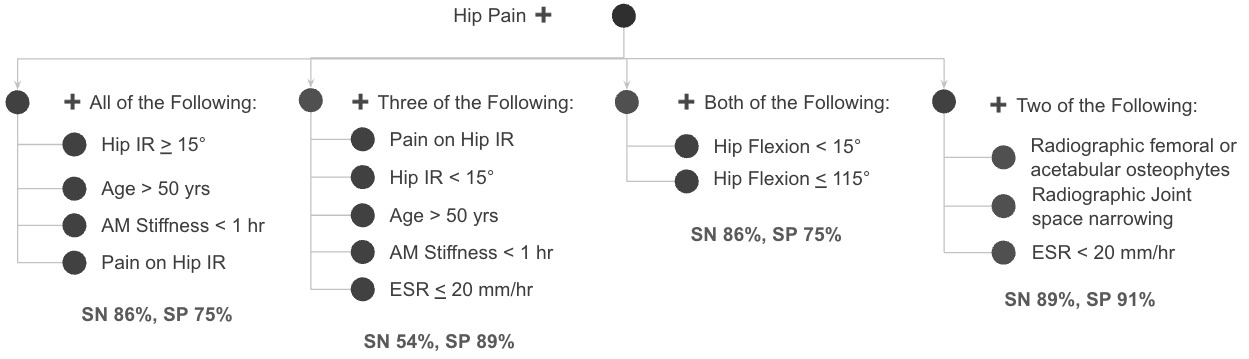
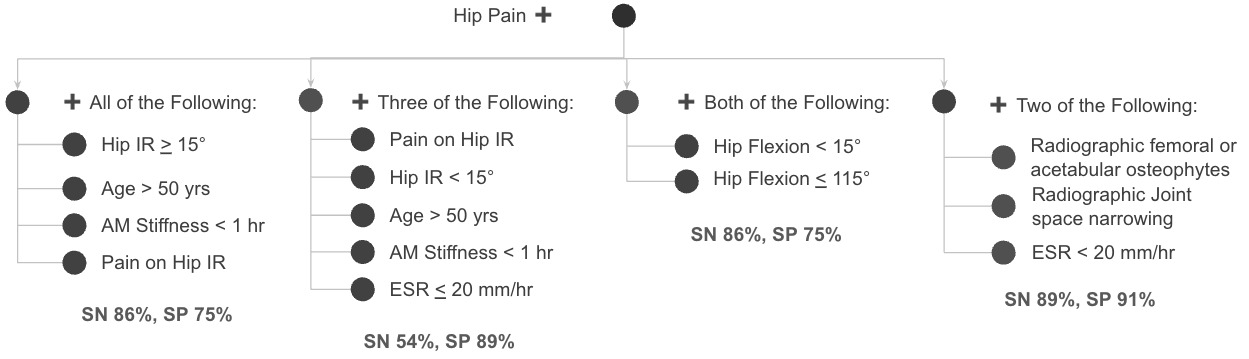
The primary problem and chief complaint were right hip pain. Subjectively, based on the ACR’s clinical classification criteria for hip osteoarthritis, the subject presented with signs and symptoms consistent with right hip osteoarthritis.11 Hip pain in combination with hip internal rotation (IR) less than 15° and hip flexion less than 115° indicates hip OA with 89.0% specificity (SP) and 54.0% sensitivity (SN).11–13 Other clinical features for the likelihood of a hip OA diagnosis included age over 50 years old, morning stiffness that improved less than one hour after waking, pain with hip IR, and the risk factor of participating in a high impact sport (long distance running).2,11–13 Figure 1 delineates the ACR criteria and a decision tree of clinical features.
Alternate diagnoses included other intra-articular hip pathologies such as femoral acetabular impingement (FAI) or labral lesion, as well as lumbar radiculopathy. FAI is diagnosed via a triad of symptoms (clicking, catching, giving way or anterior/ lateral hip pain), positive clinical signs (FADIR or FABER testing), and radiographic evidence of a hip deformity (CAM or pincer lesion).14 FAI consists of morphological variations between the acetabulum and proximal femur that result in early contact during movement.14,15 Key functions of the labrum are to increase stability and distribute weight bearing forces by deepening the hip sock and creating a suctioned seal that retains synovial fluid.16,17 A labral injury is typically precipitated by an acute mechanism of trauma or develops gradually over time by activities involving repetitive end range flexion, twisting, or pivoting.16–18 Despite the subject having positive symptoms (anterior and lateral hip pain), no inciting event, and the presence of a diurnal pattern diminished the likelihood of FAI or a labral tear.
The subject presented as a good candidate for a conservative plan of care based on his hypothesized hip OA severity. A comprehensive physical therapy program seemed to correspond well given the subject’s multifaceted clinical presentation. The chief complaint of hip pain arose from three distinct areas around the hip making the possible differential diagnoses more complicated to surmise. Moreover, the subject’s clinical signs were consistent with several competing intra-articular etiologies. Additionally, the AAOS suggests stratifying the presentation of hip OA and comparing comprehensive programs rather than single interventions. Both initial scores from the Lower Extremity Functional Scale (LEFS) and Visual Analog Scale (VAS) classified the subject as moderately impaired for function and pain respectively. From the LEFS and VAS outcome measure scores, the subject was stratified as moderately impaired hip OA severity. The subject was motivated, able, and engaged in a comprehensive program consisting of manual therapy, exercise therapy, physical activity, and aerobic exercise.
EXAMINATION
The first examination procedure performed was a postural screen of the spine and hips, performed in the standing position. Prior history of right sided sciatica and postural findings of hip bony landmark asymmetry and flattened lumbar spinal curvature prompted a more in-depth review of the lumbopelvic region. Active range of motions (AROM) of the lumbar spine and hip joint were examined next. Hip and spine AROM were conducted to identify which body regions reproduced familiar pain and to assist in a diagnosis of hip OA in accordance with criteria established by the ACR. Jin et al. reported that the lumbar and sacroiliac (SI) regions can refer symptoms to the hip.19 Thus, lumbar facet joint closing maneuvers were included and elicited both suprailiac and anterior hip pain, prompting a more in-depth evaluation of these structures.
Normal hip ROM ranges can vary by age and position tested.20 Goniometry has good validity and reliability and was used for all hip testing.21 The supine position was used for testing hip flexion, IR and ER, but extension was tested in prone. Approximate adult hip ROM has been reported to be 125° of flexion, 35° of IR, 45° of external rotation (ER), and 15° of extension.20 The subject’s right hip AROM was limited in all four tested motions, measured at 90° of flexion, 10° IR, 30° of ER, and 10° of extension. AROM of the right hip revealed that flexion elicited anterior hip pain, internal rotation reproduced anterior hip and groin pain, while external rotation provoked groin pain.
Manual Muscle Testing (MMT) of the lower extremities and passive accessory intervertebral motion (PAIVM) of the lumbar spine were performed to help rule out involvement of the lumbosacral spine. MMT reliability and validity have been regarded as inaccurate at higher grades, greater than the resistance of gravity; therefore, MMT was used only as a lower-quarter myotomal screen.22 MMT was performed in the seated position with thighs supported at the edge of the table, and the findings were unremarkable. PAIVM reliability and validity have been regarded as poor when assessing lumbar segmental hypomobility but seem to improve to good when assessing for painful lumbar segments.23 Moreover, PAIVM reliability and validity may be enhanced by combining results from other tests or measures.23 PAIVM was performed in prone, which reproduced both suprailiac pain and anterior hip pain when assessing passive joint mobility of both the central spinous process and right transverse spinous process of the L1 vertebral segment. Both PAIVM and lumbar AROM facet closing maneuvers resulted in both suprailiac pain and anterior hip pain, indicating possible lumbar facet joint pain referring to the right hip.
Lastly, special testing of the lumbar spine, SI joint, and hips was completed to further rule in a hip pathology and more completely rule-out symptoms of spinal origin. The thigh-thrust test (sensitivity 90.0%, specificity 66.0%) was used, as a positive test would indicate further diagnostics.23 The presence of bony landmark asymmetry during the postural screen prompted testing. The thigh thrust was negative bilaterally, which significantly diminished the probability of SI joint involvement. The straight leg raise (SLR) has moderate to very low reliability and high sensitivity for assessing neural tension; the cross straight leg raise (CSLR) has moderate to very low reliability and high specificity for disc herniations.24,25 SLR and CSLR were both negative bilaterally, reducing the probability of a primary diagnosis emanating from the lumbar spine. The flexion, adduction, internal rotation (FADIR) test and flexion abduction, external rotation (FABER) tests are commonly used for hip pathologies.13,14,18,20 Both FADIR (sensitivity 86.0%, specificity 33.0%) and FABER (sensitivity 78.0%, specificity 17.0%) testing were positive on the right hip indicating a more probable hip etiology.26 Table 1 further outlines the examination and findings.
CLINICAL IMPRESSION 2
Both the subject’s subjective and objective examination correlated with the signs and symptoms consistent with hip OA. The initial impression was complex because the subject’s chief complaint of hip pain was emanating from three different areas: suprailiac, anterior, and groin. The lumbar discs, lumbar facet joints, and lumbar stenosis can all refer to pain into the thigh.19 Lumbar spine ROM testing reproduced right hip anterior and suprailiac pain; however, the absence of radicular features, unremarkable lower quarter myotome screen and negative lumbar special testing suggested the lumbar spine could be a plausible contributory factor rather than a primary diagnosis. The subject’s age, clinical findings, and diurnal pain pattern are consistent with an 89.0% specificity and 54.0% sensitivity of hip OA as a primary diagnosis.
A plan of care was established including twice weekly sessions for a duration of six weeks with treatments consisting of manual therapy techniques, therapeutic exercise to strengthen and stabilize the lower quarter, and a prescribed home exercise program (HEP) incorporating aerobic exercise and therapeutic exercise. The LEFS and VAS outcome measures were completed at time of initial assessment and after six weeks of treatment. Hip ROM and functional outcome measures (long run mileage and total weekly mileage) were measured at the initial assessment and after three weeks of treatment. The subject continues to be appropriate for the case, as abundant evidence from the ACR, AAOS, APTA, and KNGF supports physical therapy as a first line treatment for mild to moderate cases of hip OA.10,12,13,15 The subject’s LEFS and VAS outcome measures were both measured as moderately impaired for function and pain respectively; therefore, the subject was stratified as moderately impaired for hip OA in the implementation of this multimodal approach.
INTERVENTION
The interventions were selected based on strength of evidence and then progressed primarily via frequency, intensity, and volume.13 Weight loss is strongly recommended for subjects who are overweight, 25.0 or greater, or obese, 30.0 or greater.1,2,10,27 The subject’s BMI was less than 25.0 and thus was not incorporated into this multimodal approach. Each session began with manual therapy before exercise therapy. Joint mobilizations were primarily used to increase hip AROM in flexion and IR and to a lesser extent for pain modulation. Soft tissue mobilizations were used for pain modulation and signified as a personal and contextual factor, because the subject reported prior treatment of massage therapy provided some relief for his anterior hip pain. Exercise therapy followed MT each session and consisted of core and hip stabilization exercises that were completed prior to strengthening exercises. Exercise therapy interventions were progressed following the FITT principles. The types of strength exercises were chosen by which ones could be safely and most maximally loaded while maintaining hip and spine alignment.
Joint mobilizations started with a duration of 2 sets of 30 seconds and an intensity of a grade III mobilization. Over the course of the twelve treatments, durations and intensities progressed to 2 sets of 60 seconds of grade IV mobilizations. Hip IR was the most severely limited AROM. Thus, a lateral glide manual intervention was performed throughout each of the twelve treatments. Next, hip flexion was addressed via a manual inferior glide, which progressed in time duration and intensity of graded mobilization from treatment sessions four through eight. Other manual interventions were tried with minimal benefit and can be viewed in Table 2. Due to the diminishing progress from manual interventions, exercise therapy was emphasized after treatment session eight by adding additional stabilization and strength exercises.
Stabilization exercises were selected for the trunk and pelvis aimed to improve pelvic neuromuscular control. Trunk exercises were completed with bodyweight only whereas pelvic exercises used theraband tension. Treatment session one started with a volume of 2 sets of 10 repetitions and progressed by 5 repetitions each of treatment sessions two and three for a total volume of 2 sets of 20 repetitions per exercise. Then, the type of stabilization exercises were progressed in treatment session four at a volume of 3 sets of 10 repetitions. Again, volume was progressed by 5 repetitions during treatment sessions five and six for a total volume of 3 sets of 20 repetitions per exercise. The progression of volume from treatments one through six served as a method to increase intensity of exercise. Length of lever arm or band tension were used to progress stabilization exercises from treatment sessions seven through twelve.
Strength exercises followed a similar progression to stabilization exercises where volume progressed from 2 sets of 10 repetitions during treatment one to 3 sets of 20 repetitions by treatment number six. A balance assisted split-squat was the first maximum strength exercise chosen as the subject was able to achieve foot-knee-hip alignment with a neutral spine. A balance assisted split-squat was progressed to a loaded split-squat without upper extremity support by treatment nine. The second maximum strength exercise chosen was the back supported weighted bridge as the subject demonstrated proper lumbopelvic neuromuscular control throughout the movement. Intensity progressed treatments nine through twelve by adding five pounds of load per treatment at a consistent volume of 3 sets of 10 repetitions. Relative maximal weight ranges of 10 repetitions were targeted by increasing load and cueing the subject that the target intensity was muscle fatigue, close to but not actually muscle failure. The split-squat, hip bridge and other strength exercises were progressed from partial to full range of motion throughout the twelve treatment sessions to increase exercise intensity while maximizing hip and spine alignment. It is of note that current clinical practice guidelines do not mention effectiveness for partial versus full range of motion exercises in the context of hip OA; however, research in healthy individuals generally agrees that full range of motion exercises confer enhanced muscle adaptations compared to partial. Although, partial range of motion exercises are an efficacious alternative, especially when considering injury management, personal and contextual factors.28
OUTCOME
The subject improved in all primary outcomes including pain, most ROM’s, functional outcomes, and activity tolerance. Regarding pain, the VAS is reliable and valid outcome measure recommended for the management of hip OA.13,29 The VAS is a horizontal 100 mm, bidirectional straight line ranging from “no pain” to “worst pain imaginable” where pain is demarcated with a vertical line.29 The VAS is used for subjects to rate their current pain; the MDC is 8 mm.29 The subject’s VAS was initially 61/100 indicating moderate pain intensity and improved to 52/100 indicating a significant change in pain but still a moderate pain intensity. Hip AROM improved from flexion 90° to 110°, IR 10° to 20°, and ER 30° to 35°.
The LEFS is another reliable and valid outcome measure recommended for assessment of the individuals hip OA.13,30 The LEFS is a 20-question scale that assess functional limitations of the lower extremity.30 Degree of functional limitation is rated from 0 to 4 with a maximal score of 80, indicating no difficulty. Lower scores are associated with increased difficulty or inability to perform an activity. The minimal detectable change (MDC) and minimal clinically important difference (MCID) are both 9 points where scores greater can reasonably be attributed to a true change in outcome.30 The subject’s LEFS was initially 32/80 indicating moderate limitation and progressed to 50/80 indicating mild limitation and a significant improvement in function.
The subject reported an increased ability to enter and exit vehicles, take long car rides in excess of one hour and negotiate stairs without suprailiac, anterior hip, or groin pain. Over the six-week plan of care, the subject increased jogging frequency and time. The subject increased jogging frequency from two to three days weekly to four to five days weekly with minimal pain or functional limitations. The subject’s jogging regimen consisted of two types of aerobic workouts, a base mileage jog and a long-distance jog. The base mileage jog duration progressed from an average distance of 3.0 miles to 6.0 miles. Activity tolerance of a weekly long-distance jog improved from 4.0 miles to 8.0 miles and total weekly jogging mileage progressed from 10.0 miles to 28.0 miles.
DISCUSSION
A six-week, twelve treatment session, multimodal approach was effective at reducing pain and increasing lower extremity function in the subject who was an experienced recreational runner. Multimodal approaches have been described with contrasting evidence for their efficacy.6 Perhaps, one reason for this variation in efficacy of such interventions is because the severity of hip OA was not stratified in participants. Underlying pathophysiology of pain mechanisms could be another contextual factor.
Pain is a complex and dynamic process undergoing plasticity both peripherally within local tissues and centrally via the brain and spinal cord.31 Many peripheral tissues, excluding articular cartilage, have been shown to be innervated by sensory afferent nociceptors.27,31,32 Increased peripheral nociceptor sensitivity, also known as peripheral sensitization, can stimulate nociception at lower thresholds.33 Whereas central sensitization has been identified by temporal summation both locally at the osteoarthritic joint as well as sites away from the joint, which might present as secondary hyperalgesia.15,31,33 Research suggests three distinct pain mechanisms - nociceptive, neuropathic, and nociplastic - may underlie pathophysiology of peripheral and central sensitization.3,15,27,31,33,34 Moreover, nociceptors and the nociceptive pan mechanism may be stimulated physically by mechanical stress or chemically via inflammatory mediators.3,27,32
Both peripheral and central pain mechanisms may have been present in this subject, athough they were not specifically assessed. Chronic pain (lasting more than three months), pain quality of a dull ache, pain with prolonged sitting, and pain during long car rides could have been partly attributed to central sensitization or the nociplastic pain mechanism. At least one of the three pain locations (suprailiac, anterior hip, groin) might have been hyperalgesia. Perhaps, aggravating factors such as exiting cars, negotiating stairs, and strenuous exercise could be attributed to mechanical stress or nociceptive drivers. Neuropathic pain might be present in people with higher subjective pain ratings and impaired function.33 Given the subject’s suspected moderate pain and moderate functional limitation, neuropathic pain may have contributed to a lesser extent. However, regular aerobic exercise may promote analgesia in people with neuropathic pain.34 The subject engaged in a considerable amount of aerobic exercise where both frequency and duration were likely enough to elicit adaptation.
Evidence suggests that both ET and MT modulate both peripheral and central pain mechanisms.34 Soft tissue and joint mobilization are thought to produce analgesia of central pain mechanisms by descending pain inhibition, also described as conditioned pain modulation (CPM).3,15,34 Manual hip joint mobilization was a primary intervention where the effect could have served to increase the viscoelastic properties of the joint capsule aimed at addressing a peripheral nociceptive input of mechanical or inflammatory stress; whereas, possible nociplastic mechanisms could have increased top-down central pain inhibition. Massage therapy also appeared to be effective, alluding to a potential CPM effect stimulating the nociplastic pain pathway. Further research should investigate the pathophysiology of pain mechanisms in the creation of comprehensive and individualized programs for the treatment of hip OA.
The intensity of MT joint mobilization has been examined in the context of hip OA. Research suggests that a high force in the open packed position significantly increased hip ROM in all planes of motion compared to low and medium forces.5 The open packed position of the hip is characterized by 30° of flexion, 30° of abduction, and slight ER.5 Particularly, forces up to 800 N have been shown to incur superior clinical effects compared to unknown forces.7 The results suggest a critical level of force would be necessary to change the elastic properties of the joint capsule and thus increase hip ROM.5 Grade IV hip joint mobilizations were extensively used during the subject’s treatment intervention and the open packed position was targeted. Although forces and precise mobilizing positions were not measured, hip ROM improvements provide a hypothesis for the benefits conferred from the MT intervention.
ET in this case consisted of a combination of mobility, stability, and strength training exercises. A considerable amount of research exists for the efficacy of strength training in the treatment of hip OA.1,4,7,8,12,27,35 Specific parameters with this subject can be referenced in Table 3. An important consideration in the management of hip OA is the balance between hip joint under loading and overloading as hip joint forces interact with cartilage mechanobiology to regulate cartilage structure.1,15,27,36–40 Therefore, exercise intensity and optimal hip joint loading may be important considerations that must be balanced for effectiveness of exercise therapy interventions. Hip joint loading was increased over the course of the six-week treatment intervention across FITT principles. Rigorous intensities were targeted during the ET intervention, but it is unknown whether they were achieved. The subject did achieve muscle fatigue but never exercised to muscle failure and his prior lifting performance was undetermined. It is important to note that the subject expressed strenuous exercise as both an aggravating and alleviating factor. Further research might try to utilize hip joint loading as a contextual factor for individualizing treatment for the management of hip OA.
Knee adduction moment (KAM) and knee extensor weakness contribute to knee osteoarthritis (KOA).13,15,36 Similarly, perimuscular weakness, decreased gluteal muscle size, and increased hip adduction moment are thought to contribute to the progression of hip OA.13,35,37 ET emphasized loading the hip musculature while minimizing hip adduction. Strength exercises targeted hip musculature directly such as the weighted, back-supported hip bridge utilizing a hip-hinge movement pattern (articulating an anterior and posterior pelvic tilt) and the weighted, split-squats by biasing a near vertical shank angle. Dynamic hip stabilization exercises such as the band-resisted, running-form lunge actively pulled the hip into adduction to increase neuromuscular control, coordination, and hip abductor muscle activation. It should be noted that the duration of the physical therapy intervention spanned six weeks; therefore, strength improvements may have been incurred but may not have been long enough to elicit a true muscle hypertrophy adaptation.35 Further research might try estimating exercise intensities in excess of 60% of a one-rep maximum effort, ensure a strength training frequency of greater than or equal to twice weekly, ensure intervention durations exceeding six week protocols, or might utilize biomechanics as a filter for exercise selection. Perhaps, the biomechanical emphasis in conjunction with strength training adaptations played a role in the significant functional improvement outcomes observed.
LIMITATIONS
A number of limitations of this case report should be noted. First, no cause and effect can be determined. Next, the interventions were found to be effective for this subject, a seasoned runner of more than 40 years, but may not be generalizable to other individuals or populations. Objective measures for strength were not performed and would have offered additional detail (beyond MMT ratings) to describe strength gains that were noted. Also, neither a gait analysis nor a running analysis was performed which may have assisted in analyzing functional changes that occurred. Further research may benefit by performing one repetition maximum testing or calculations in order to more precisely measure exercise loading progression. A method of measuring aerobic exercise intensity such as heart rate or rate of perceived exertion (RPE) may also be measured to more confidently draw conclusions regarding the effects of aerobic exercise.
CONCLUSION
The results of this case report indicate that a six-week, twelve treatment session, multimodal approach was effective at reducing pain, increasing lower extremity function and jogging activity tolerance in a 75 y.o. male subject who was an experienced recreational runner. The effectiveness of the ET, MT, and aerobic interventions could be attributed to the assessment of the subject as having moderate hip OA severity, the pathophysiology of underlying pain mechanisms, the intensity of force used during mobilizations, the underlying mechanobiology of optimal hip joint loading considered during exercise progressions, or addressing neuromuscular control of the lumbopelvic/hip region to improve lower extremity biomechanics and reduce hip adduction during functional activities such as running. Further research could consider melding a pathoanatomical approach with a pain mechanistic approach while considering hip OA severity as a paramount contextual factor in the creation of comprehensive, personalized and holistic programs for the management of hip OA.
Conflicts of interest
The author reports no conflicts of interest.
Acknowledgements
University of Illinois at Chicago Department of Physical Therapy including Dr. Tanvi Bhatt, Dr. Deborah Davey and Dr. Meaghan Rubsam for direct technical help, academic advising, manuscript organization and critical intellectual review and Dr. Laura Thorp for indirect assistance and intellectual contributions.