
INTRODUCTION
Softball consistently ranks as the fourth highest National Collegiate Athletic Association (NCAA) female sport by participation, comprising over 9% of all NCAA female athletes. Despite its growing popularity, there are wide-ranging gaps in current softball literature, with studies most frequently reporting solely on injury prevalence, and frequently drawing comparisons between softball and baseball athletes. With support from injury databases, researchers have gone as far to summarize the overall injury rate in fast-pitch softball to be comparable to or exceed that in baseball.1 In-game injury exposure is higher in baseball athletes by a difference of 1.48 injuries per athlete-exposure (AE); however in-practice injury exposure is higher in softball athletes by a difference of 0.82 injuries per AE.2,3 Despite these findings, modifiable and non modifiable injury risk factors, such as measures of humeral retrotorsion (HRT), throwing volume, strength, and range of motion, are less documented in softball literature when compared to the baseball literature.
Glenohumeral range of motion (ROM) is a well-established risk factor for upper extremity injury and has been well investigated in baseball athletes. High school baseball players with glenohumeral internal rotation (GIR) ROM differences greater than 25º are at an increased risk of shoulder and elbow injury than similarly aged controls.4 Increased injury risk also exists among baseball pitchers who demonstrate insufficient glenohumeral external rotation (GER) ROM on the throwing arm (<5º) when compared to the non-throwing arm.5 Comparatively, Shanley et al. discovered that softball players with a >25º side to side GIR difference did not suffer an upper extremity injury over the course of a season.4 However, to the authors knowledge, Shanley et al. is the only study to investigate the rotational motion and injury risk in softball athletes. Furthermore, the aforementioned studies did not include softball pitchers, a position that is required to throw both overhand and pitch underhand, nor did they account for HRT and its influences on glenohumeral rotational ROM.6–9
Researchers have aimed to determine the anatomical adaptations that occur amongst softball players. Similar to a baseball player, the throwing arm of a softball player exhibits more GER ROM and less GIR ROM when compared to the non-throwing arm.10 While the reduction in throwing side GIR ROM may be less in softball players compared to baseball players, obvious differences across ROM measures still exist.10–12 Osseous changes to the humerus, such as anatomic humeral retrotorsion (aHRT), is one potential explanation for these throwing related adaptations. Anatomic HRT refers to a posteromedial orientation of the humeral head axis with respect to the distal humeral epicondylar axis.13 In baseball players, there is more aHRT preserved on the throwing arm when compared to the non-throwing arm (the difference between throwing arm aHRT and the non-throwing arm aHRT, which is defined as relative HRT [rHRT]), however; limited studies have investigated these adaptations in a softball population.7,14,15 The greater angle on the throwing arm between the proximal humeral head and the distal epicondylar axis of the humerus allows for more layback during the throwing motion, while naturally diminishing the amount of internal rotation.16 Softball pitchers, however, perform both an underhand windmill motion to pitch and an overhand motion to throw. The difference in overhand throwing volume between softball position players and pitchers may lead to differences in range of motion and humeral retrotorsion seen between the positions. With this in mind, aHRT has been minimally investigated in softball pitchers.
Several studies have shown when glenohumeral ROM is accounted for within the context of rHRT, a concept referred to as HRT-corrected motion, deficits in GIR are not as common as once thought in baseball players.6–9 In fact, deficits in GER are more likely than GIR deficits in both healthy and injured baseball players.6–9 Yet, it is unknown if the same is true for softball players. Relative HRT is a crucial measurement to obtain as it helps identify motion differences and, in the presence of total rotational range of motion (TROM) deficits, determines the direction in which the deficit exists. Therefore, the purpose of this study is twofold: 1) to determine if there are differences in GER ROM, GIR ROM, TROM, aHRT, rHRT, and HRT-corrected motion between collegiate softball position players and pitchers, and 2) to determine if differences exist between GER and HRT-corrected GER and GIR and HRT-corrected GIR in collegiate softball players, regardless of position. The first hypothesis was that there would be significant differences in range of motion profiles between collegiate softball position players and pitchers. The second hypothesis was that there would be significant differences in GER and HRT-corrected GER and GIR and HRT-corrected GIR between collegiate softball players, regardless of position.
METHODS
Study Design
This study is a retrospective analysis of prospectively collected data approved by The University of Texas Health Science Center at Houston Institutional Review Board (IRB approval #: HSC-MH-22-0537) in which all college participants signed an informed consent form.17 Player data were collected at different timepoints throughout the season with 15 players collected in 2023 (two during a spring preseason measurement in January of 2023, 11 during a midseason measurement in March of 2023, and two during a fall preseason measurement in August and September of 2023) and 48 players in 2024 (18 during a spring preseason measurement in January of 2024, 11 during a midseason measurement in March and May of 2024, nine during a fall preseason measurement in August of 2024, and 10 during a fall postseason measurement in October of 2024). The most recent data for each player was used for statistical analysis. All data were collected within the softball athletic training facility at the affiliated NCAA Universities. Data were collected using REDCap (Research Electronic Data Capture) electronic data capture tools hosted by UTHealth’s School of Biomedical Informatics. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external source.18,19
Study Participants
Softball players from two NCAA Division I softball programs participated in the testing sessions. Participant demographics were collected via self-report (age, height, weight, and throwing arm). Each participant self-reported primary playing position as either pitcher or position player. Participants were included in this study if they met the following criteria: (1) between the ages of 18 and 24 years old, (2) no history of elbow or shoulder surgery in the previous year that restricted athletic participation in all team activities at the time of testing, and (3) no current shoulder or elbow injury that limited or restricted participation in all team activities at the time of testing. Players were excluded from the study if they were unable to participate in all team activities due to an active, ongoing injury, or had an injury to the non-throwing side shoulder or elbow. Individual injury and participation status were verified with the team’s Athletic Trainer.
Procedures
Objective measures of shoulder rotational ROM and aHRT were collected during the years mentioned above. Measures of GIR, GER, and aHRT were obtained by examiners with combined experience evaluating overhead throwing athletes of greater than 20 years. The examiners were not blinded to the throwing arm in this study. Before data collection, the intrarater and interrater reliability for each of the three measurements were established. The intraclass correlation coefficients (ICCs) with 95% confidence intervals (CIs) and standard errors of measurement (SEMs) were calculated for this study and are presented in Table 1.
Objective Rotational Motion
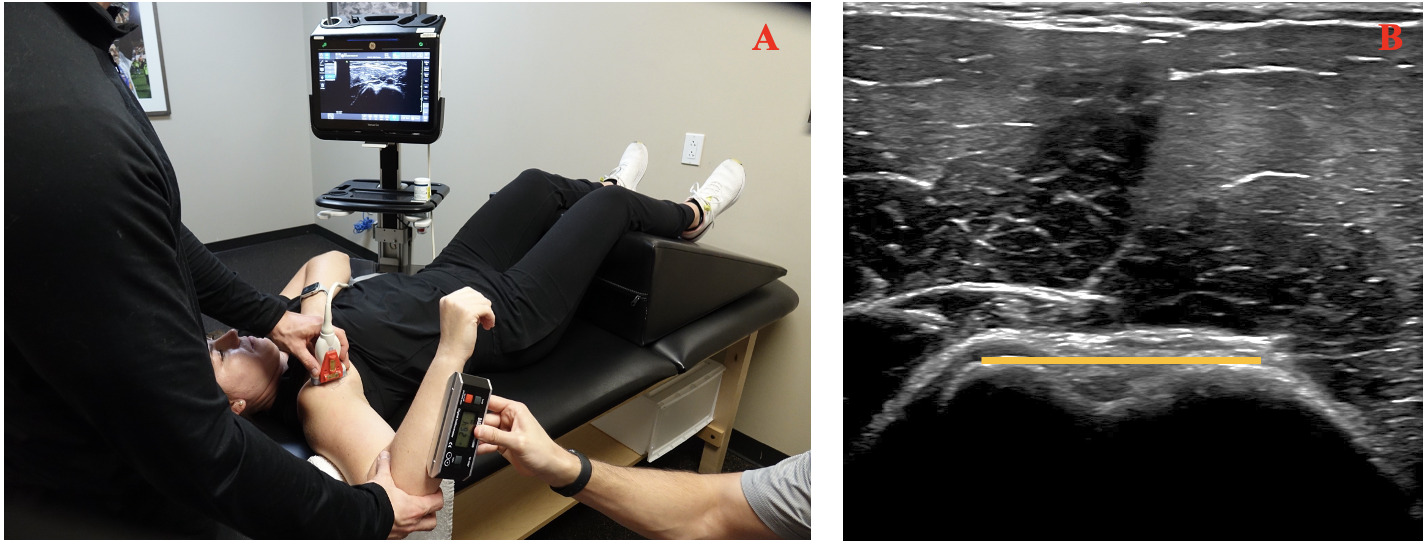
GER and GIR were assessed passively in each arm utilizing a digital inclinometer (Performance Health, Warrenville, IL) as previously described by Entler et al. (Figure 1).6 Participants were supine on a treatment table in a hook-lying position with their legs supported on a bolster. A rolled towel was placed under the participants humerus to maintain scapular positioning in the coronal plane for standardization of testing. Examiner one stood at the head of the participant while moving the arm into 90° of shoulder abduction and 90° of elbow flexion while stabilizing the scapula. Scapular stabilization was achieved by grasping the coracoid process anteriorly and the spine of the scapula posteriorly for both GER and GIR. Examiner one determined the ROM for GER as the first point of resistance and GIR at the first point of scapula movement. Examiner two utilized a digital inclinometer to document the measurement, aligning the inclinometer just under the shaft of the ulna. Prior to the measurement, the inclinometer was zeroed to the vertical plane. For each participant, GER was measured first, followed by GIR. Each direction was measured twice and the mean of the two values were used for final analysis. If there was a wide discrepancy in the two measurements (>3°), a third measurement was performed to ensure consistency.
_external_rotation_and_(b)_internal_rotation.png)
Anatomic Humeral Retrotorsion
Anatomic HRT was assessed utilizing an indirect ultrasonographic technique descried and validated by previous researchers (Figure 2).20 This indirect technique measures aHRT by calculating the forearm inclination angle relative to a standardized humeral position.21 Each participant was placed supine in a hook-lying position on a standard treatment table with the legs set on a bolster. Examiner one placed the participants shoulder at 90° abduction with the elbow at 90° flexion. A towel roll was placed under the participants humerus to maintain scapular positioning in the coronal plane. Ultrasound gel (Cardinal Health, Dublin, OH) was placed on a straight ML 12-15 probe connected to a Venue Go R3 (GE HealthCare, Chicago, IL) ultrasound machine. Examiner one positioned the probe over the anterior aspect of the participants glenohumeral joint.6 The probe was aligned perpendicular to the long axis of the humerus in the frontal plane, and kept level as determined by a bubble level on the face of the probe. Examiner one rotated the humerus until the deepest part of the bicipital groove was visualized and the apexes of the greater and lesser tuberosities were parallel to the horizontal plane (Figure 2). Examiner one then asked examiner two to pace the digital inclinometer just below the shaft of the ulna and record the degrees of inclination. The digital inclinometer was zeroed to the vertical plane prior to the measurements. This process was repeated twice on both arms. The mean of the two values was used for final analysis; a third measurement was performed if there was a wide discrepancy (>3°) between the first two measurements.
_patient_and_rater_positioning_during_measurement_of_humeral_retrotorsion__(b)_field_of.png)
Data Reduction
The raw data for both objective GIR and GER as well as aHRT were reduced. Calculations (TROM, rHRT, HRT-corrected motion) utilized in this study were conducted consistent with previous research.6,8 When interpreting rHRT (defined as the difference between throwing arm aHRT and the non-throwing arm aHRT), a negative value indicates greater aHRT in the throwing arm compared to the non-throwing arm. In addition, when interpreting the HRT-corrected GER and GIR, a negative value indicates a deficit, while a positive value indicates a gain in motion on the throwing arm.
Statistical Analysis
Means and standard deviations were calculated for all continuous descriptive data, while frequencies are presented for categorical data. Descriptive data were compared statistically between position players and pitchers using independent t-tests for continuous data and chi-square for categorical data. To assess the first hypothesis, eleven independent t-tests were utilized with glenohumeral motion and HRT variables as the dependent variables and position (position vs. pitchers) as the independent variable. To assess the second hypothesis, four paired t tests were utilized. The independent variables were position players and pitchers. The dependent variables consisted of objective GIR, HRT-corrected GIR, objective GER, and HRT-corrected GER. Lastly, the authors compared softball HRT-corrected GIR and GER findings from this study to previously reported findings in collegiate and professional baseball players.
All assumptions were met as each dependent measure was assessed for normality using the Kolmogorov-Smirnov Test and visualization of Q-Q plots. Additionally, homogeneity of variance with Levene’s Test was assessed for each of the dependent variables. Due to the unequal sample sizes in the sample population and the findings from the Levene’s test of homogeneity of variance, comparisons were interpreted assuming unequal variances.22 Cohen d effect sizes were estimated for each t-test with values interpreted as small (0.2), moderate (0.5-0.6), or large (0.8-1.0).23 The initial alpha level of p < 0.05 was considered significant for all statistical analyses; however, a Bonferroni alpha correction was implemented to help avoid risk of Type 1 Errors when analyzing the dependent variables within the t-test analyses. Final two-tailed p-values were hypothesis-specific, with a final alpha of p = 0.004 for the first hypothesis and p = 0.012 for the second hypothesis (0.05/n, where n equals the number of tests performed). All data were analyzed using statistical package SPSS version 29 (IBM Corp. Armonk, NY, USA).
Post-hoc power analysis using G*Power 3.1 (G*Power, Franz Faul, Universität Kiel, Germany) was performed to determine the statistical power observed regarding the dependent t tests pertaining to the differences observed between objective ROM and HRT-corrected ROM in the position player cohort (d = 1.46) and the pitcher cohort (d = 1.38). Interpreting the alpha (0.05) with two-tails and a sample of 45 (position players) and 18 (pitchers) participants, the observed minimum power was B = 0.99. However, the power observed for the between group comparisons was insufficient; when considering the smallest (d = 0.10, corresponding with the effect size observed between groups for nonthrowing arm GER) and largest (d = 0.57, corresponding with the effect size observed between groups for throwing arm TROM) observed effect sizes, thus the observed power for the between group comparisons ranged from 0.06 to 0.52.
RESULTS
Collegiate softball player demographics (n=63) were analyzed by player position and reported in Table 2. Body weight was not recorded at the time of testing for 12 athletes in total (eight position players and four pitchers). Pitchers were significantly taller than position players (p = 0.008), however no other significant differences were present in player demographics. Glenohumeral ROM data are reported by player position in Table 3. There were no significant differences in throwing arm GER (p = 0.30), nonthrowing arm GER (p = 0.70), throwing arm GIR (p = 0.16), nonthrowing arm GIR (p = 0.88), throwing arm TROM (p = 0.84), nonthrowing arm TROM (p = 0.65), throwing arm aHRT (p = 0.05), nonthrowing arm aHRT (p = 0.77), rHRT (p = 0.08), HRT-corrected GER (p = 0.89), or HRT-corrected GIR (p = 0.67) between position players and pitchers.
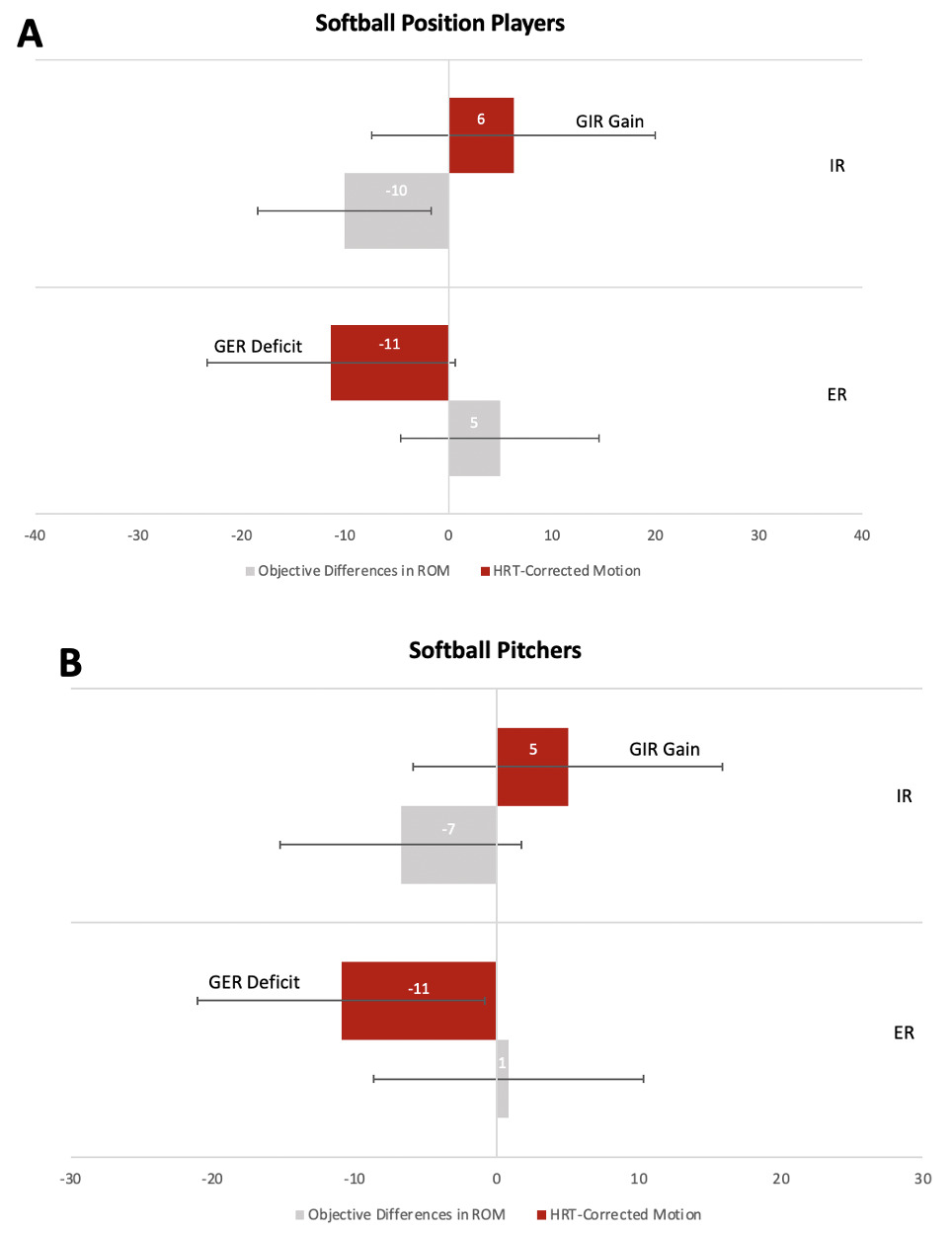
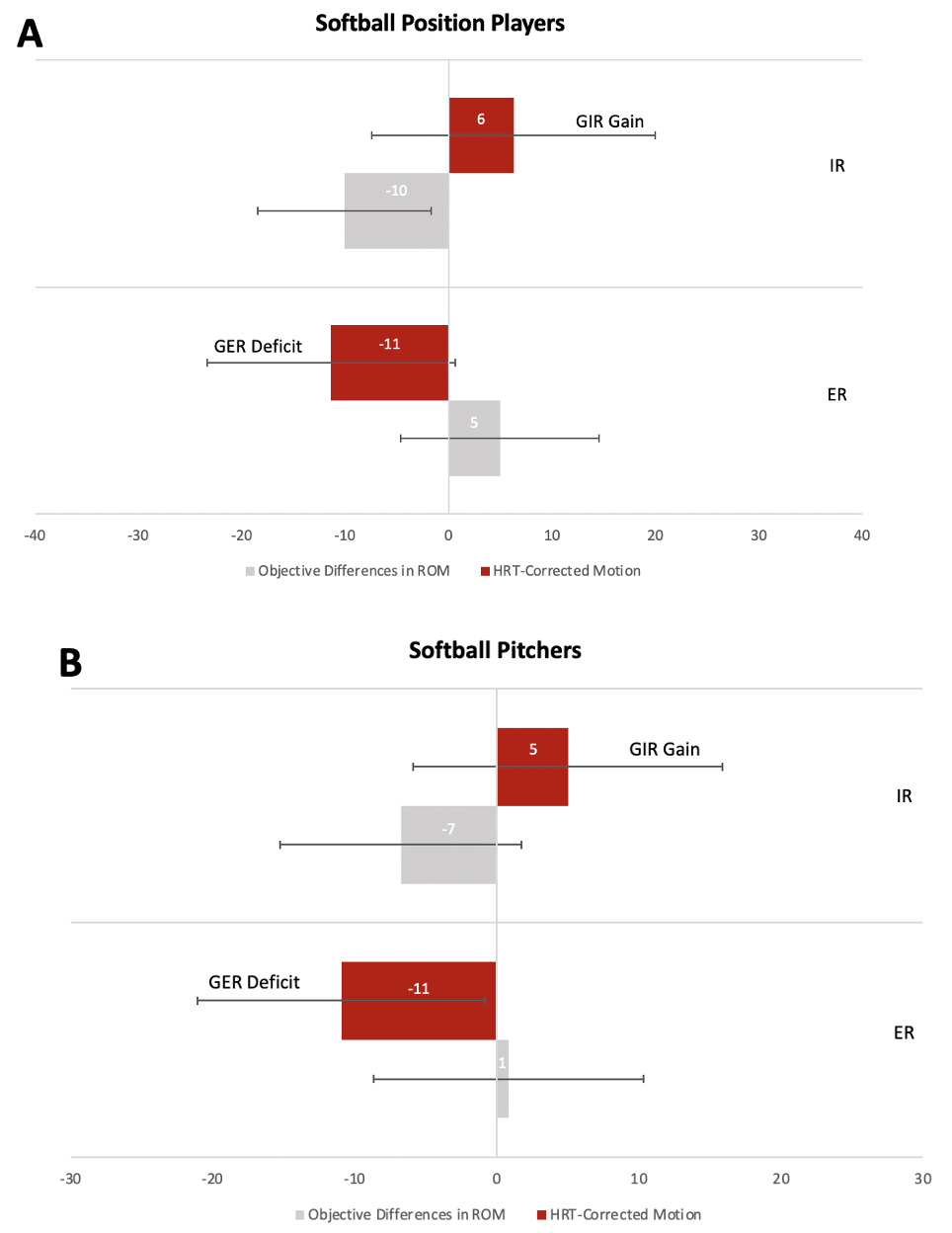
There were significant differences between measurements in objective GER and HRT-corrected GER in position players (p < 0.001) and pitchers (p < 0.001). There were also significant differences between objective GIR motion and HRT-corrected GIR in both position players (p < 0.001) and pitchers (p < 0.001) (Figure 3).
DISCUSSION
Pitchers showed slightly reduced throwing arm aHRT values when compared to position players, however the results were not significantly different, thereby refuting the first hypothesis. The main findings of this study indicate that softball position players and pitchers demonstrated differences in GER and GIR when compared to HRT-corrected GER and GIR. This supported the secondary hypothesis that softball players, irrespective of player position, demonstrated differences in GER and HRT-corrected ER and GIR and HRT-corrected GIR. More specifically, GIR deficits are on average not present in softball players when glenohumeral ROM is interpreted within the context of rHRT; GER deficits, however, are present in this population in the context of rHRT.
There were no significant differences in range of motion measures between softball position players and pitchers. One explanation for this is that softball position players and pitchers often have overlapping throwing and training loads and commonly participate in similar strength and conditioning programs which may minimize differences seen in shoulder mobility. In addition, softball players begin throwing at a young age while often playing multiple positions. This can lead to comparable long term outcomes in shoulder motion measurements. As a result, the shared exposure to repetitive throwing demands may minimize detectable differences in shoulder motion between groups.
This is the first study to specifically examine aHRT and rHRT in collegiate softball pitchers. Hibberd et al. reported aHRT values in collegiate softball and baseball position players but did not include pitchers in that cohort.15 When assessing rHRT between softball pitchers and baseball pitchers, the rHRT is smaller in softball pitchers when compared to baseball pitchers.6 One explanation for this may be that softball pitchers use both an underhand windmill motion to pitch and overhand motion to throw, unlike their baseball counterparts who throw and pitch entirely overhand. While more data are needed within the softball literature, clinicians should still consider aHRT when interpreting GER and GIR measurements in softball players, regardless of position.
This study was the first to examine glenohumeral rotational motion in the presence of rHRT in a collegiate softball population. Previous studies indicate that the overhand throwing motion requires repetitive and excessive GER ROM causing osseous adaptations to occur at the humerus during physical development.24 As all softball players throw overhand, the nature of softball predisposes them to developing preserved aHRT values on their throwing arms. It is important to consider HRT when measuring glenohumeral rotational motion within these players to determine if ROM deficits are present and if so, which direction is most affected (GER vs GIR).
The findings of this study are consistent with previous research conducted in baseball populations that calculated HRT-corrected GER and HRT-corrected GIR.6,8 Differences were found between objective GER and HRT-corrected GER and GIR and HRT-corrected GIR in this cohort of softball players, regardless of their position. Softball players present with HRT-corrected GER deficits. This is similar to the findings of Myers et al. who found that collegiate baseball players did not demonstrate GIR deficits in the context of HRT, but instead GER deficits.7 The current findings, along with previous research, imply that GIR deficits are less frequently observed in both baseball and softball players when correcting for HRT. In fact, deficits in GER may be more common. To identify the truest injury profile of a thrower, the osseous change of HRT must be taken into account.
The current findings suggest that in the context of HRT, collegiate softball players demonstrate similar glenohumeral ROM profiles as baseball players. Table 4 presents data to examine these similarities. Although previous research has suggested that softball players do not exhibit humeral osseus adaptations comparable to those of baseball players,15 the current findings indicate that collegiate female softball players demonstrate similar throwing arm adaptations in response to joint stresses associated with the throwing motion, as described in the baseball literature.
A Clinical Example
To further demonstrate the relationship between rHRT and the clinical interpretation of glenohumeral rotational range of motion, a clinical example is presented for a 16-year-old softball pitcher. The values in Table 5 represent the bilateral rotational range of motion, TROM, bilateral aHRT, and the calculated side-to-side differences between the throwing and non-throwing arms.
Solely based on the clinical measurements taken, this athlete presented with a 10° gain of GER ROM, a 20° loss of GIR ROM, and a 20° side-to-side difference in aHRT, or rHRT. Conventional studies would suggest that this athlete has an acceptable amount of external rotation gain on the throwing limb (>5)°,46 and pathological glenohumeral internal rotation deficit (GIRD) as demonstrated by a side-to-side difference of 20° in the presence of a total arc of motion loss greater than 5° degrees (-10°).13 Clinical reasoning would lead the sports medicine team to suspect a mechanism of internal rotation loss as a potential contributor to pain and dysfunction. However, when the HRT-corrected equations are applied, a shift in the “deficient” rotational direction becomes apparent (Table 6).
Based on the current findings, when the HRT-corrected equations are applied, this athlete actually has a 10° deficit of glenohumeral external rotation with no observed GIRD. Therefore, the rehabilitation team should select targeted treatment strategies to remedy soft tissue impairments related to external rotation ROM deficits. In this example, if only the clinical interpretation is considered (without regard to rHRT), a practitioner may inadvertently prescribe stretches to address perceived GIRD targeting the posterior shoulder soft tissues when they are not warranted. This example, combined with similar observations in healthy baseball athletes,37,43,44 and injured baseball athletes,25 and the results from the present study, together demand that attention be paid to commonly observed HRT-corrected GER deficits.
This study is not without limitations. Convenience sampling, while representative of collegiate softball teams, resulted in uneven groups of position players and pitchers. Most collegiate softball teams have a roster size of 22 players, with 3-4 pitchers per team on average. This impacted the author’s abilities to achieve equal sampling of position players and pitchers, potentially causing concern when considering the findings of comparisons between groups. While the present authors were intentional with the inclusion of the findings related to post-hoc power for clarity to the readership, the deficit of post hoc power in some comparisions does not detract from the findings. However, the results of the comparisons between pitchers and position players should be interpreted with caution as the observed power suggests the Type II Error rate was inflated due to an inadequate sample for between group comparisons, and an increased sample size could alter the interpretation of these results between pitchers and position players. Additional data collection is needed to increase the softball pitcher sample size and further investigate the differences in aHRT and HRT-corrected motion measurements between softball players that both pitch and throw overhand, and those who just throw overhand. The majority of softball players in this study were right-handed. Previous research on baseball players has indicated that left-handed baseball pitchers demonstrate smaller relative HRT values than their right-handed counterparts.25 While right-handedness is a dominant trait in the general population and within softball and baseball, findings of this study cannot be confidently applied to left-handed players until more data is available. Moreover, all participants were of college age, having reached skeletal maturity. Future researchers should aim to determine if these results are consistent in softball players across their lifespan, from youth to skeletally mature throwers. Lastly, as players were measured at multiple time points throughout the course of a season, the most recent measurement was used for data analysis. This may have influenced HRT-corrected motion measurements as previous research has shown collegiate softball position players to increase throwing arm ER and TROM and nonthrowing arm ER, IR and TROM, while collegiate softball pitchers increase throwing arm IR and TROM over the course of a season.11 Additionally, this study did not control for throwing activity performed prior to data collection, which may have influenced the ROM values obtained. To limit the effect of time of season or recent throwing activity on glenohumeral ROM measurements, future researchers could consider measurements at similar preseason timepoints. Due to the paucity of published information on softball players of any age, it is important to continue to analyze these athletes. With continued research, guidelines that minimize injury risk and maximize sports performance in softball players can be established.
CONCLUSION
Collegiate softball players, regardless of position, demonstrated differences between throwing arm GER and HRT-corrected GER and throwing arm GIR and HRT-corrected GIR. When examining an overhead athlete in any sport, it is necessary to consider the impact of osseous changes on glenohumeral rotational motion. Both softball and baseball players consistently demonstrate osseous adaptations to their humeri, likely as a result from the large biomechanical stresses placed on their bodies from throwing. Even though softball pitchers primarily utilize an underhand windmill motion to pitch, the position still engages in overhand throwing, such as in warm-ups and when fielding their position. Based on the current findings, it is imperative that aHRT be assessed in all softball players. This information can aid clinicians in identifying true motion restrictions and implementing meaningful intervention, thus attempting to reduce player injury risk and maximizing throwing performance.
Conflicts of interest
No conflicts of interest are declared by the authors.