

INTRODUCTION
Approximately seven million people in the United States seek treatment for sports related injuries each year, with the majority of these injuries occurring in the lower extremity, most commonly the knee.1 These injuries carry significant healthcare, societal, and economic repercussions. For instance, 20% of children in the United States with sports related injuries miss one or more days of school,1 and pediatric patients undergoing knee ligament surgery are at risk of decreased academic performance.2 In addition, over 25% of US adults with a sports injury will miss one or more days of work.1 The implications are even more sobering when focusing on specific injuries, namely anterior cruciate ligament (ACL) tears. ACL tears are increasing in incidence, with between 130,000-175,000 ACL reconstructions (ACL-R) performed annually.3 In fact, the U.S. spends $1-2 billion annually on anterior cruciate (ACL) management alone,4 though conservative treatment of ACL injuries and management of long-term sequelae from the initial injury may increase the economic cost above these estimates.
While there have been numerous advances in surgical technique, graft choices, and rehabilitation protocols, the results after ACL reconstruction are still less than ideal. For example, only 63% of NFL players return to their NFL careers after ACL reconstruction,5 with similar return to play (RTP) rates among high school and college football players. After ACL reconstruction, athletes are at an increased risk for reinjury of both the injured and contralateral side, especially if they return to sports too quickly.6 Wiggins et al. reported that 23% of young athletes returning to high risk sports after ACL reconstruction experienced a second ACL tear, most often during the early return to play period. Allen et al. demonstrated a 34% rate of second ACL injury among young females returning to competitive soccer after ACL reconstruction.7
In the long term, athletes are at an increased risk of developing premature osteoarthritis (OA) following ACL injury, even if they receive timely reconstruction surgery. Although the causes of ACL injury are multifactorial, it is imperative that clinicians seek to identify modifiable risk factors that may help to reduce the devastating short and long term consequences resultant of ACL tears.8 Perhaps one of the easiest modifiable risk factors to address is improving the athletes’ muscle control and strength to avoid potentially injurious positions.9
Interestingly, an increasing volume of literature has demonstrated a link between core (hip and trunk) muscle function and lower extremity injury risk such as ACL tears.10–13 Larwa et al. demonstrated that poor core stability, landing on the heels, decreased strength of the hip abductors , and increased knee valgus may contribute to injury risk in young athletes.14 Moreover, a 2007 study of collegiate athletes found that those suffering knee, ligament, and ACL injuries specifically had greater trunk displacement than their uninjured cohorts during an unanticipated trunk stabilization task.15 Recent evidence from Glattke et al. in 2022 confirms these findings.16 Additional research has connected core function with cycling mechanics, running injuries, patellofemoral pain, ankle injuries, jumping mechanics,17 step-down performance,18 and even hamstring injuries.19 In light of this evidence, it is not surprising that hip, core, and trunk strengthening has been advocated for in injury prevention and rehabilitation, as well as for improvement of athletic performance. The purpose of this current concepts review is to synthesize current evidence on hip- and core-focused assessment and rehabilitation strategies that may mitigate ACL injury risk.
THE CORE AND ITS RELATIONSHIP TO ACL INURY MECHANISM
The term “core” can be defined as the lumbo-pelvic, trunk, and hip muscles which exert their forces on the spine, ribs, pelvis, and proximal femur.20 While the exact muscles classified as “core” musculature vary among publications, the core is generally considered to encompass 29 muscle pairs including the paraspinal, abdominal, gluteal, and hip girdle muscles.20 These core muscles work synergistically to stabilize the trunk and spine. Their forces result not only in active motion but also offer stabilization against external forces.11 The abdominal and spinal musculature work together to prevent against unwanted trunk flexion, extension, lateral bending, and rotation. The hip muscles and abdominals help to maintain proper pelvic alignment. Additionally, the hip muscles enable optimal firing of the hamstrings and quadriceps muscles.11 The trunk and pelvic stabilization provided by the sequencing of muscle firing patterns around the hip and core is especially crucial to athletes, as it facilitates smooth dynamic movements of the extremities.13 A systematic review by Crossley et al. demonstrated that adolescent sports teams that implemented multi-component core strengthening programs reduced lower extremity injuries including hamstring and knee injuries with notable reductions in knee ligament injuries.21
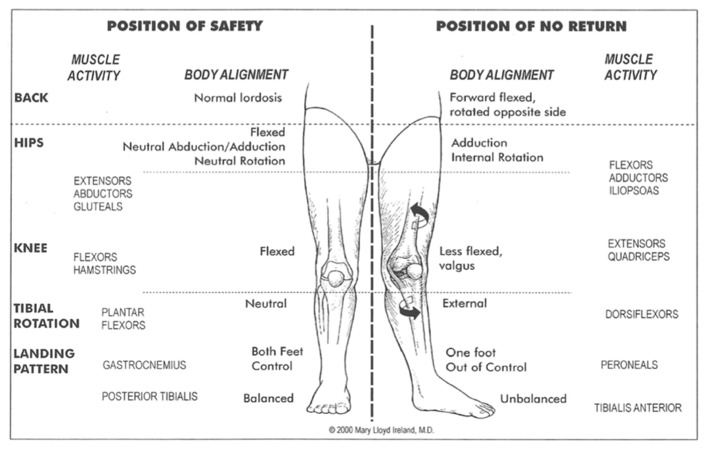
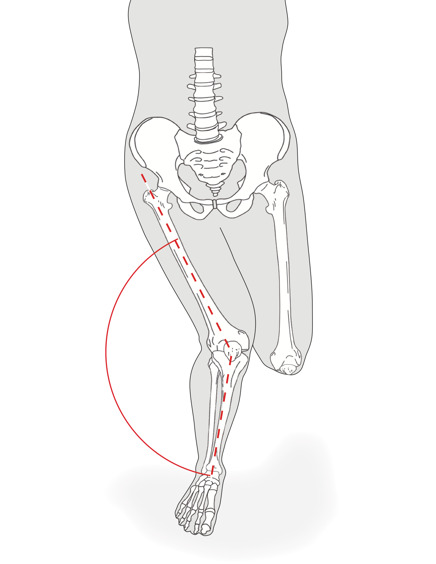
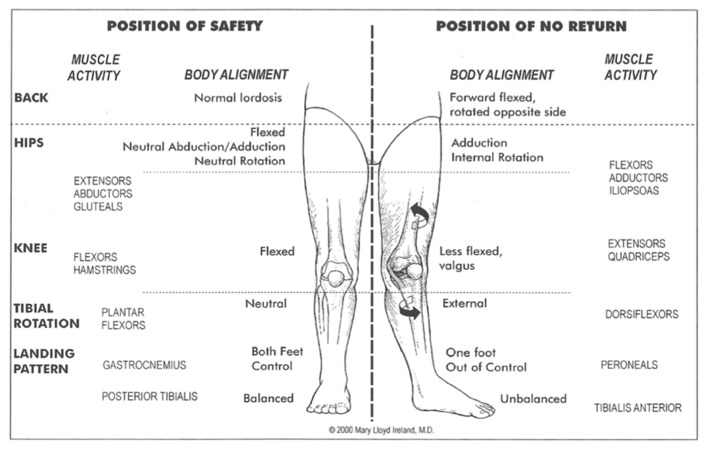
Over 70% of ACL injuries are noncontact,22 meaning that the athlete’s body position during injury is a critical, potentially modifiable, risk factor. In fact, hip, femur, and knee position during ACL injury has been relatively well studied,12,13,23 and Reiman et al. aptly described the core as the “proximal link to a distal problem.”24 Boden et al. refined this injury mechanism framework using 3D video analysis.25 As early as 1999, Ireland et al. defined the “position of no return”26 (Figure 1) which described a position of hip adduction, hip internal rotation, and slight knee flexion associated with ACL injury risk.
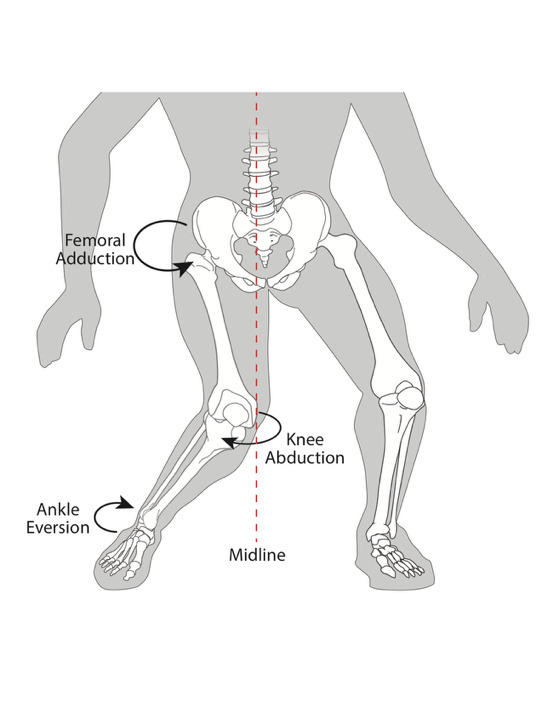
In 2005 Hewett et al. further validated this concept with what they described as “dynamic valgus” of the knee to explain the increased hip adduction and knee valgus often seen with noncontact ACL injuries (Figure 2).27
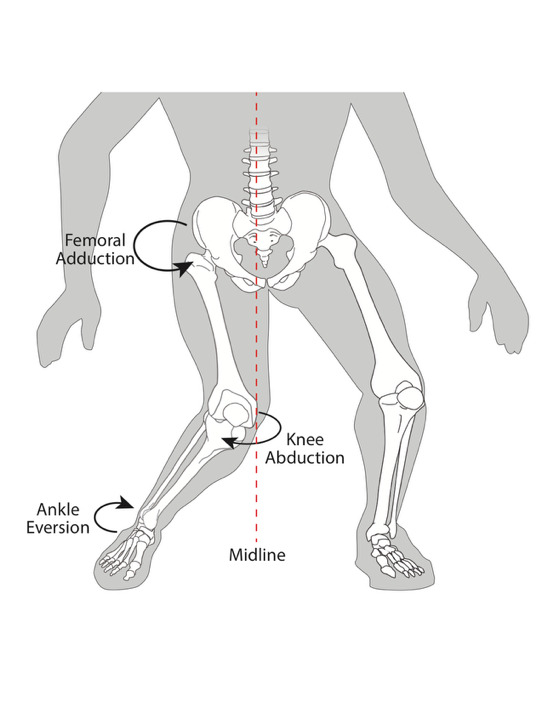
Subsequent video analyses have confirmed that the majority of noncontact ACL injuries occur during a landing or cutting task with the knee in a valgus position.22 Additional biomechanical and cadaveric studies have confirmed increased strain on the ACL when knee position is consistent with an adducted and internally rotated hip28 and a valgus knee.29 Studies have further demonstrated that knee abduction moments coupled with tibial internal rotation increase ACL strain even further.23 Clinically, these noncontact ACL injuries manifest in a dynamic position with the hip adducted and internally rotated, the knee at a low flexion angle and in valgus, and the tibia internally rotated.22
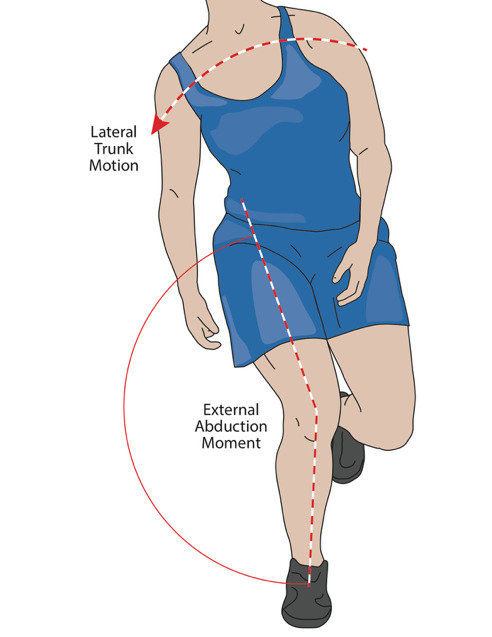
More recently the role of the trunk during noncontact ACL injury has received greater attention. For example, Zazulak et al. showed a connection between poor neuromuscular trunk control and knee ligament injury risk in 277 female athletes.15 Jamison et al. and others reported a connection between frontal plane trunk positioning30 and knee abduction moments predictive of ACL injury.27 In the study by Jamison et al., increased lateral bending away from the new direction of travel during an unanticipated run-and-cut maneuver was associated with increased knee abduction moments.30 Similarly, Frank et al. demonstrated that less trunk rotation toward the new direction of travel and increased trunk forward flexion during a side step cutting task placed the knee at an increased risk for ACL tear.28 In fact, the current best model of body position during non-contact ACL injury consists of excessive lateral trunk flexion away from the intended direction of travel, increased hip flexion, internal rotation, and adduction, and dynamic knee valgus and tibial internal rotation (Figure 3).23

PRE-INJURY AND RETURN TO PLAY SCREENING
This increased awareness of the role of trunk and hip function in the development of knee injury23 necessitates that effective injury screening and RTP tests are developed that incorporate accurate and reliable assessments of those elements. Many of the same biomechanical risk factors that are associated with primary ACL injury persist after surgery and even after RTP.31 Hence, it makes sense that effective injury screening tests could also serve as RTP tests, and vice-versa. However, despite a considerable amount of research having been dedicated to decreasing ACL injury risk and developing effective RTP protocols, there is no consensus protocol or group of screening tests. It remains unlikely that one quick test would be able to identify all individuals with hip and trunk dysfunction, and effective injury prevention and RTP screening will likely necessitate a comprehensive battery of different tests.
General Concepts
Based on the totality of evidence implicating dysfunction of the core in ACL injury mechanisms, any set of prevention or RTP screening tests should incorporate evaluation of the hip and trunk. Ideally, these tests should be inexpensive, easy to administer, quantifiable, reliable, valid, require only easily obtainable equipment, and take relatively little time to complete for each subject. In addition, these tests should identify quantifiable deficits that can be specifically targeted in prevention and/or rehabilitation programs. Furthermore, caution should be exercised when employing limb symmetry indices or other methods of comparing to the uninjured leg in the postoperative setting.31 Many studies have shown that strength and kinematic differences exist in both legs postoperatively, and similar research has shown that the uninjured limb is at nearly the same risk for an ACL tear after ACL-R as the previously injured limb.31 Moreover, owing to the singularity of the trunk segment, trunk dysfunction should affect both limbs to a similar degree, and not just the injured or “at-risk” limb.
Hip Muscle Function
Hip muscle function has been most commonly evaluated via isometric strength testing using hand held dynamometry.11,18,32–34 Alternatively, some studies have utilized more complex tests such as isokinetic strength testing and rate of torque development testing using expensive testing equipment such as the Biodex system,32 and even various forms of electromyography (EMG). However, belt-stabilized hand held dynamometry has proven especially effective in analyzing muscule strength with high inter- and intra-tester reliability (Figure 4).35

In a 2016 study of over 500 male and female athletes across a variety of sports, hip abduction and external rotation strength as measured by hand held dynamometry was predictive of non-contact ACL injury risk.33 Similarly, a 2004 study reported that dynamometer-measured hip external rotation strength was predictive of lower extremity injury in a group of 140 male and female collegiate athletes.11 Numerous additional studies have linked laboratory measured hip muscle weakness with lower extremity kinematics suggestive of increased ACL injury risk.32
Trunk Muscle Function
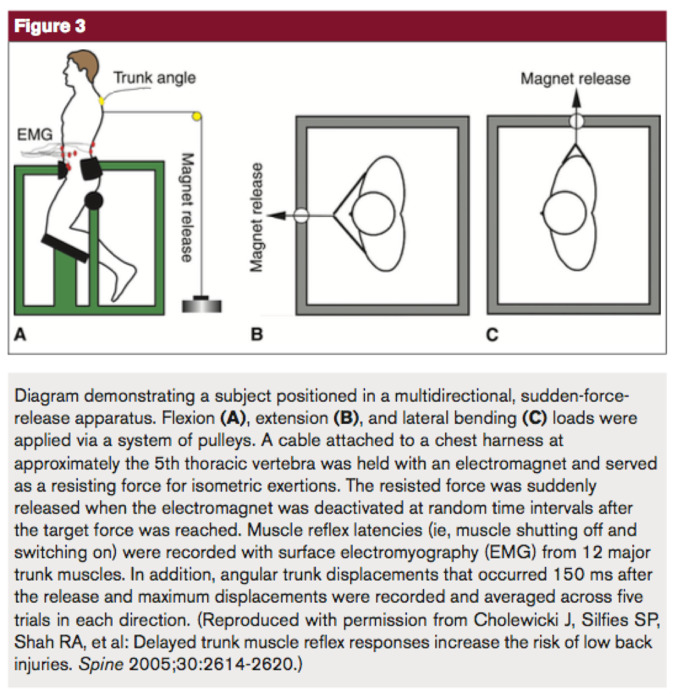
Trunk strength and stability have proven more difficult to assess. In general, efforts to measure the strength and stability of the trunk are variable across different studies and in many cases require complex testing devices. Moreover, there is no agreed upon measure of trunk muscle strength or stability. Zazulak et al. studied trunk stability using a sudden “force release” device (Figure 5).15
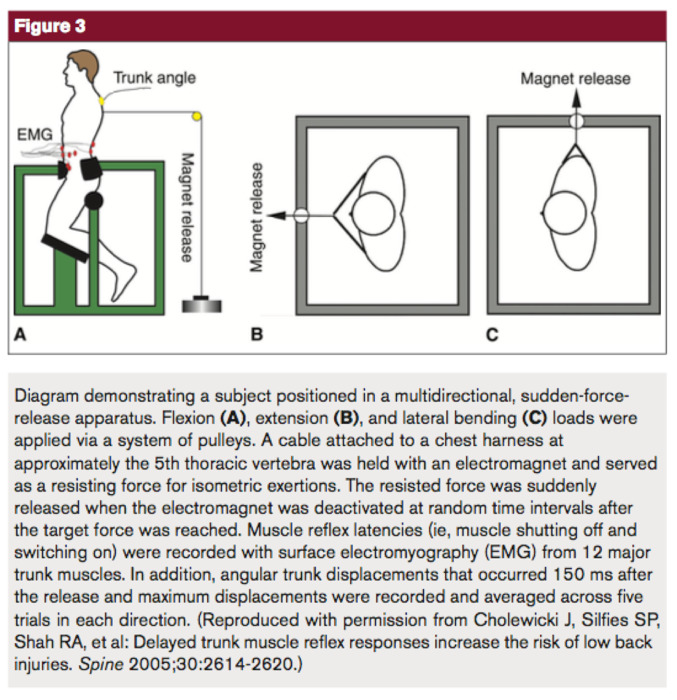
While providing useful information regarding neuromuscular trunk control and its relationship to knee injury risk, the testing apparatus does not lend itself to screening on a large scale. Many of studies assessing trunk muscle function tested measures of trunk endurance utilizing tests such as timed front and side plank tests, the modified Beiring-Sorensen test, and various maximum repetition abdominal exercises.11,13 On the other hand, Jamison et al. analyzed surface EMG activity of trunk musculature during run-to-cut maneuvers. While they found that L5 level co-contraction correlated with increased knee abduction moments, their results were otherwise mixed.37 Although not in the setting of ACL or lower extremity injury risk assessment like the previously described studies, Prieske et al. recently described an innovative method of measuring trunk strength. They utilized a frame and a harness force transducer assembly to measure isometric trunk flexion and extension strength in the standing position.38 Importantly, few of these described methods that assess trunk control are easily accessible in clinical settings, and more work is needed to identify and validate tests that are able to clinically assess trunk control.
Functional Tests
As athletic activities (and injuries) do not occur in isolation, it can be advantageous to utilize closed chain functional assessments to screen for injury risk and RTP readiness.27,39 In fact, many of these tests are commonly used, well-studied, and easily performed in a variety of environments with a high degree of reliability and consistency. It is important to understand what the individual components that make up each test are so that deficiencies can be properly identified and rehabilitated accordingly. Additionally, certain functional tests may incorporate muscle fatigability which may more closely mirror real-world conditions which influence occurrence of ACL tears.
The Single Leg Step-Down and Single Leg Squat Tests
Single leg step-down and squat tests have been well studied in the literature, and both have been shown to detect deficiencies in both hip muscle and trunk muscle strength.18,34 Multiple authors have described the utility of the single leg squat in identifying femoral adduction and knee valgus that is associated with ACL injury risk.13 The single leg squat can be a useful tool to perform in the office setting to quickly assess for hip muscle dysfunction (Figure 6).

While perhaps not as effective at demonstrating abnormal coronal plane hip and knee kinematics as the single leg squat, a timed, maximum repetition single leg step-down (SLSD) test has recently been advocated for lower extremity injury risk and RTP screening.18,34 This test consists of a subject stepping down from a raised platform 6-8 inches high in a controlled manner, for a maximum number of repetitions within a defined time period (usually 30 or 60 seconds; Figure 7).

Not only have SLSD tests been shown to identify individuals with weak hip musculature, recent investigations have also suggested that the step-down test can identify individuals with trunk muscle weakness, implying that the SLSD may be useful as a single test to gauge both hip and trunk muscle strength.18 The 60-second version of this test also likely introduces some degree of fatigue into overall test performance, which may increase its ability to simulate “real-world” conditions. In fact, patients have been shown to have SLSD asymmetries more than eight months after ACL reconstruction and even at time of RTP. Moreover, Kline et al. demonstrated that early postoperative step-down test performance was predictive of improved knee mechanics in ACL reconstruction patients at six months.34 This evidence suggests that the SLSD test may be a useful screening test to assess injury risk and readiness for RTP. In addition, the SLSD test is low-cost and relatively easy to administer without extensive set-up or special facilities. However, no prospective studies have been performed assessing stepdown performance results with injury risk.
Single Leg Hop Tests
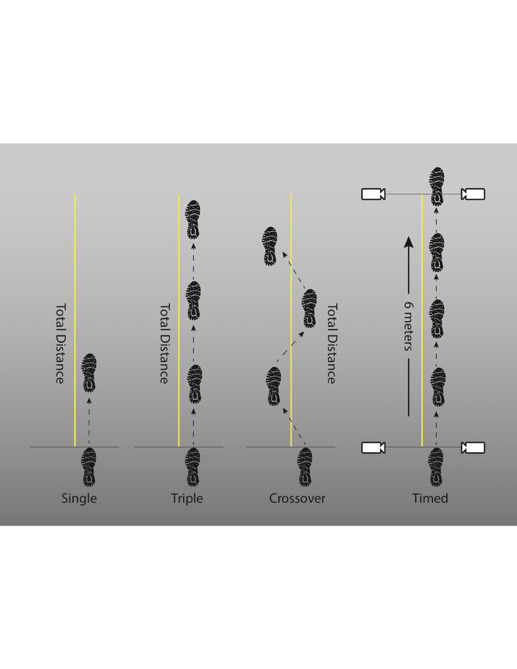
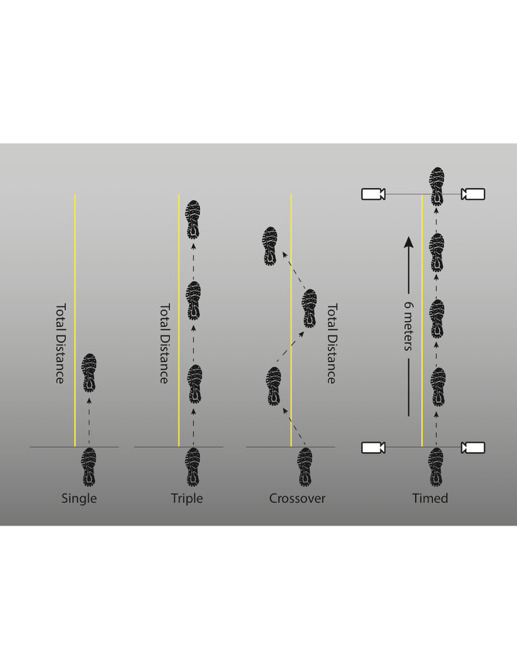
Perhaps no functional tests have been more commonly employed as ACL RTP tests than the single leg hop tests. Single leg hop tests have been demonstrated to be reliable and valid,40–42 and have been shown to predict injury risk. The most reported hop tests are the single leg hop for distance, the triple hop, the crossover hop, and the timed hop. In brief, the single leg hop for distance is a single hop in which the maximum distance covered is measured. The triple hop is similar, but consists of three hops for maximum distance, all on the same leg. The crossover hop requires three hops, but each jump must land on alternate sides of the designated line. Finally, the timed hop test measures the amount of time it takes the participant to hop six meters on a single leg, regardless the number of jumps needed (Figure 8 ).41
These tests were traditionally used to assess RTP readiness, and a limb symmetry index (LSI) of 85% or greater was considered the cutoff for RTP.41 In fact, Logerstedt et al. showed that a 6-month timed hop test LSI of 88% or more was predictive of successful 1-year outcomes in ACL-R patients (as measured by IKDC scores) and Reinke et al. reported that postoperative hop test performance correlated with IKDC and KOOS at the two -year follow-up.40,42 However, recent studies have shown that the uninjured leg in ACL reconstruction patients may have persistent strength and functional deficits compared to controls, and Thomee et al. and Munro et al. have advocated for a higher LSI threshold of 90-95%, or even analysis of absolute strength values relative to pre-injury levels or normative data, prior to RTP.31,41 Preoperative hop test performance has not been shown to relate to postoperative outcome.40
Few studies have examined the hip and trunk muscular contributions to hop testing.
Yonz et al. reported that isometric hip strength—including hip external rotation, abduction, and extension—demonstrated significant correlations with single-leg hop tests in patients 6–18 months following ACL reconstruction, whereas trunk strength measures were not associated with hop performance.43 Similarly, Kollock et al. demonstrated moderate to strong correlations between hip adductor and abductor strength and hop performance in healthy men, with triple-hop work showing a strong association with hip-adductor peak force (r ≈ 0.71; r² = 0.50) and rate of force development (r ≈ 0.62; r² = 0.38), as well as a moderate association with hip-abductor peak force (r ≈ 0.60; r² = 0.36).44 No studies to date have examined the contribution of trunk strength on hop test performance. As such, although hop tests have been well studied and proven valid in RTP scenarios, more research is needed to identify which strength components contribute the most to individual hop tests.
Y-Balance and Star Excursion Balance Tests
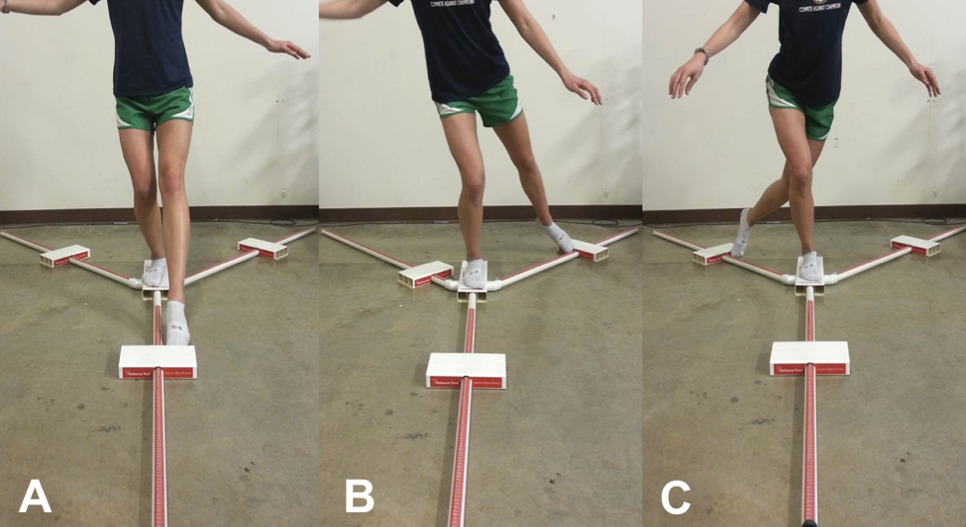
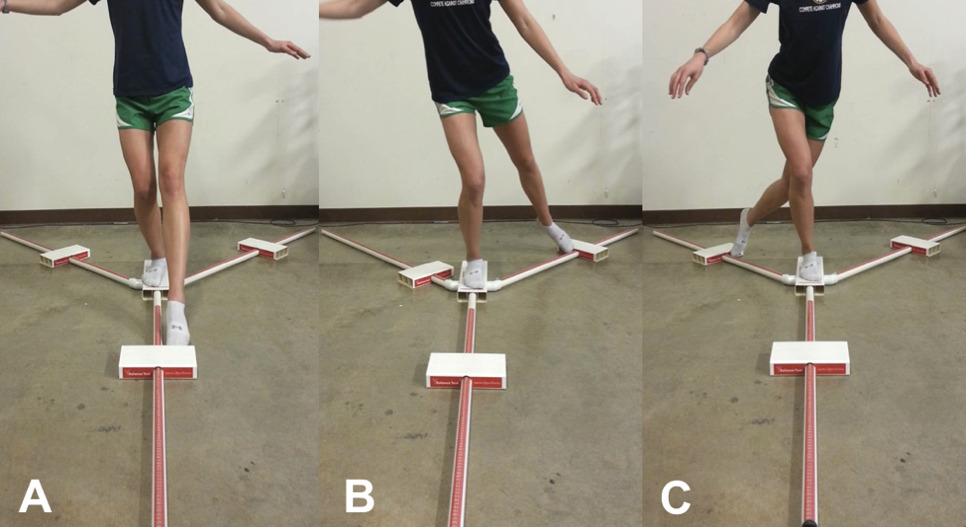
The Star Excursion Balance Test (SEBT) and Y-Balance Test (YBT) have been utilized in a variety of settings to assess neuromuscular function, postural stability, injury risk, and return-to-play readiness.39,45,46 The SEBT was first described in 1998 and measures a participants’ maximum single-limb reach distance in eight separate directions during a single leg squat on the stance leg. They YBT was derived from the SEBT in 2009 to emphasize the most commonly utilized reach directions (anterior, posteromedial, and posterolateral).45 Both tests have shown high reliability.39,45,46 While the commercially available YBT does require specialized equipment (Figure 9), similar results can be obtained with a 3-direction SEBT.45
Both tests traditionally employed the use of six practice trials and one to three measured trials, due to reported learning effects of participants. However, the high number of practice trials can be burdensome in real life testing, and several authors have concluded that as few as four practice trials are acceptable.39 Test performance is most often measured as maximum reach distance in a given direction. This distance can then be compared to the uninjured limb or normalized for limb length and compared to similar cohorts.39
Performance on the SEBT and YBT has been associated with ACL injury, or injury risk, in numerous studies. Plisky et al. reported that a 4cm or greater between limb anterior reach discrepancy resulted in a 2.5 times increased risk of lower extremity injury. Furthermore, in females, a reach distance of 94% or less of contralateral limb reach distance resulted in a 6.5 times greater injury risk.47 Smith et al. similarly found that a 4cm reach discrepancy between limbs was predictive of injury risk in Division I collegiate athletes.46 Few studies have examined Y-Balance performance in ACL injured patients. Herrington et al. reported lower reach distances in ACL-deficient limbs in the anterior, lateral, posteromedial, and medial directions as compared to controls. Interestingly, even the uninjured limb performed worse in the medial and lateral directions than the control group.48 Delahunt et al. described lower posteromedial and posterolateral reach differences in female ACL reconstructed patients at a mean of 2.9 years after surgery.49 Recently, Kline et al. did not find any correlation between YBT anterior reach and knee kinematics six months after ACL reconstruction.34 Clagg et al. found decreased SEBT and YBT anterior reach distances in ACLR patients at time of RTP.50
Few studies have examined muscle strength contributions to SEBT and YBT performance. Norris et al. reported that gluteus maximus was most activated in the anterior and medial directions of the SEBT.51 Lee et al. evaluated healthy women from age 45-80 and found that hip extension strength was positively associated with anterior and posterolateral reach directions, and hip extensor and abductor strength were positively correlated with posteromedial reach distance.52 McMullen et al. demonstrated lower SEBT reach distances after hip abduction fatiguing exercise,53 and Roberson et al. reported isometric hip abduction strength to be predictive of Y-balance composite score.54 Collectively, the results of these studies show that gluteal muscle strength and activation are important to good performance of the SEBT and YBT.
INJURY PREVENTION AND POSTOPERATIVE REHABILITATION
Numerous studies have been performed with the goal of preventing non-contact ACL injuries. Many of these trials have demonstrated that targeted exercise and rehabilitation, most often in the form of well-balanced neuromuscular training programs, can improve the deficiencies in muscle strength and functional test performance described above. Furthermore, some of these programs have been directly linked to decreased injury risk. For example, Khale et al. reported improved SEBT performance after a six-week core strengthening program in older adults.55 Likewise, McLeod et al. found improved SEBT performance after a six -week neuromuscular training program in female high school basketball players,56 and Sandry et al. reported improved SEBT performance after a six-week core stability program in high school track athletes.57 Lastly, Barber-Westin described improved hop test performance after a six-week neuromuscular training program in competitive tennis players.58 These studies show the potential of targeted neuromuscular training programs to improve the SEBT and potentially reduce injury risk.
There have also been several studies conducted assessing the effect of alterations in joint biomechanics and/or injury risk as the result of focused neuromuscular training program. For instance, Stearns and Powers demonstrated that a four-week hip-focused training program led to improved lower extremity mechanics suggestive of lower ACL injury risk in active young females.59 Zebis et al. similarly found that a 12-week neuromuscular training program led to more ACL-protective movement patterns in female soccer and handball athletes.60 These neuromuscular training programs typically consist of a combination of targeted hip and trunk strengthening, plyometric and agility drills, balance and proprioceptive exercises, and technique-focused movement retraining emphasizing proper landing and cutting mechanics.59–62 Importantly, Mandelbaum et al. demonstrated a 74% decrease in ACL injuries in female athletes who participated in a sport specific neuromuscular training program,62 and Hagglund et al. reported that higher compliance with a similar program led to less ACL injury risk in female soccer players.61
Emerging Role of Neurocognitive and Neuroplastic Factors
Although the present review focuses on musculoskeletal and biomechanical aspects of hip and trunk assessment, emerging evidence suggests that ACL injury risk and recovery are also influenced by neuroplastic and neurocognitive factors.63 Following ACL injury and reconstruction, athletes may demonstrate altered cortical activation patterns, visuomotor control, and dual-task performance, indicating that neuromuscular deficits reflect not only proximal strength and coordination but also higher-order central adaptations.64 Integrating simple neurocognitive elements such as reaction-time constraints, unanticipated cutting directions, and dual-task challenges into hip- and core-focused screening and training may better approximate the demands of sport.65 A comprehensive review of neurocognitive testing paradigms and neuroplasticity-directed interventions is beyond the scope of this review; however, future work should clarify how these approaches can be combined with the proximal assessment and training strategies described here to further refine ACL risk reduction and rehabilitation frameworks.
SEX DIFFERENCES
Females are known to have a higher relative risk for ACL tear as compared to their male counterparts, and the reasons are multifactorial.66 As Ireland described in 2002, the key factors in this discrepancy are proximal, and not distal.67 Females perform landing tasks with greater hip adduction, femoral internal rotation, and knee valgus than their male counterparts.68 Liederbach et al. found that not only did females demonstrate more knee valgus during a landing task, but also more lateral and forward trunk flexion.69 Jacobs et al. reported lower hip abductor peak torque and greater knee valgus during a landing task.70 Zazulak demonstrated that females had higher rectus femoris muscle activity and lower hip muscle (gluteus maximus) activity in a landing task as compared to males.17 Mendiguchia et al. systematically reviewed the literature and determined that females utilize different core stability mechanisms than males in landing tasks, land with less hip and knee flexion, land with a greater ground reaction force, and are at disproportionately greater risk of ACL injury during these tasks.71 Prevention and rehabilitation guidelines should account for these sex differences that contribute to high injury and reinjury rates among female athletes.
Not only do females land and cut with potentially higher risk knee mechanics, but hip and trunk strength may be more strongly related to these knee mechanics in females than in males. Burnham et al. reported that trunk strength was more related to single leg step-down performance and dynamic knee valgus in females than in males.18 Similarly, Bolga et al. reported that females generated a larger gluteus medius EMG activation during single leg squats than males, suggesting a greater reliance on gluteal function for good knee control.72 Jacobs et al. reported correlations between hip abduction strength and knee valgus during single leg landings in females, but not in males.70 Furthermore, Ferri-Caruana reported in a laboratory study with 29 female athletes that core strength and neuromuscular training improved hip and knee flexion angles during dynamic landing movements which is associated with reduced risk of ACL injury.73 These results indicate that sex differences in strength affect neuromuscular control as well, suggesting that both aspects need to be addressed in rehabilitation.
SUMMARY
Anterior cruciate ligament injury is a common occurrence in competitive and recreational athletes. An injury of this magnitude carries with it significant consequences for the long-term health of the knee, even after technically sound ACL reconstruction and rehabilitation. Therefore, any potential screening or neuromuscular training programs that may potentially result in decreased injury rates should be thoroughly investigated. Fortunately, it is well established that hip and trunk muscle strength deficits may lead to higher risk knee kinematics associated with ACL injury, and addressing these deficits may help to prevent initial or recurrent injury. This relationship may be stronger in females, although further research is needed to confirm this connection. However, the link between proximal control and ACL injury is well described, and rehabilitation and preventative efforts should focus on improving the proximal muscle groups that affect knee control.