INTRODUCTION
Younger patients undergoing total knee arthroplasty (TKA) have strong expectations to return to an active lifestyle requiring the adoption of specific programs and strategies to accomplish these goals. The inability to participate in recreational activities is often a major issue cited on patients’ final analysis and satisfaction with the surgical outcome. In this regard, many knee arthroplasty rehabilitation protocols focus on the first three months after surgery and lack robust rehabilitation protocols to restore lower extremity muscle strength, coordination, knee motion and overall function to the degree necessary to resume recreational activities.1 Limitations of knee motion and arthrofibrosis after TKA can be serious complications and the literature shows that the incidence of motion loss is from 1-20% of the cases.2 This means there can be a high number of patients affected by motion loss given that there are approximately 900,000 total joint arthroplasties performed each year.3,4
Therefore, the authors have adopted and utilized preoperative and postoperative rehabilitation programs for knee replacements fashioned after protocols for anterior cruciate ligament (ACL) and other knee ligament reconstructions. Prior research studies have identified that athletes who underwent major knee ligament surgery or had sustained complete knee dislocations sustained complications with knee stiffness, arthrofibrosis, and impaired knee and lower limb function despite undergoing postoperative knee rehabilitation.1,5–7 A number of subsequent studies have identified the importance of immediate knee range of motion (ROM) after surgery.8–11 Early identification and prompt treatment of knee motion limitations have aided in avoiding arthrofibrosis.8–11 These early studies of immediate motion and early identification of joint stiffness related to knee ligament work, laid the groundwork for applying the same principles to postoperative TKA procedures. These protocols demonstrated the importance of achieving full passive knee ROM within the first couple of weeks after surgery and that prompt treatment of early motion loss helped to preserve lower extremity function. Prompt identification of early postoperative difficulties allows for initiation of effective treatment procedures.10,11 Manual and mechanical ROM techniques should avoid high force techniques which can produce pain, damage soft tissues, and produce swelling.12–16
A safe return to an active lifestyle and recreational activities is a primary concern for younger TKA patients. Previously published work has stressed the importance of objective tests for knee muscle strength and function for assessment for readiness to return to athletics.5,6 Guidelines provided by the American Heart Association demonstrate the positive effect of physical activities on cardiovascular health, avoidance of diabetes and other medical co-morbidities including mental health and depression.7,17,18 The purpose of this investigation was to utilize objective measures on a younger population of patients following total knee arthroplasty (TKA) to allow a safe return to recreational activities and an active lifestyle. The hypothesis of this study was that a comprehensive TKA program that includes prehabilitation, early treatment of knee motion loss, enhancement of muscle strength and function testing would allow a majority of patients to return to recreational activities and an active lifestyle.
METHODS
Patients planning to undergo a unilateral TKA procedure were enrolled in this Institutional Review Board (IRB) approved, prospective study. A single surgeon performed all surgeries. Patients were divided into two groups for analysis. Patients in Group 1 completed the patient reported outcome measures (PROMs) and were followed for short-term clinical results. Patients in Group 2 completed the same PROMs but also were tested for objective parameters including quadriceps and hamstrings muscle strength, and as well, completed multiple function tests preoperatively, and at 3, 6, and 12 months postoperatively.
Inclusionary criteria were as follows: males or females 65 years of age or younger who indicated a desire to return to ADL’s, recreational and/or work activities, willing to complete the full post-operative rehabilitation process, willing to complete patient reported outcome measures (PROMs), and provide informed consent. Exclusionary criteria were as follows: male or female over the age of 65 with no desire to return to recreational and/ or work activities, patients with a history of alcohol or drug abuse within three years of the surgery, disabling or widespread osteoarthritis (OA) or other joint disease in any other joint, presence of a significant connective tissue disease, autoimmune disease, HIV positive or any other immune deficiency syndrome.
The following subjective and objective data was collected for evaluation: 1) the Cincinnati Knee Rating System (CKRS), Knee Injury and Osteoarthritis Outcome Joint Replacement Survey (KOOS JR), select questions from the VR-12 Health Survey including questions about general fitness and questions related to patient expectations before and after surgery19,20; and 2) isometric strength testing using the Biodex Isokinetic Dynamometer (Biodex Corporation, Shirley, NY) at 60 degrees of knee flexion with three repetitions each for knee extension/flexion measuring quadriceps and hamstring torque values. Additionally, the 6-minute walk, stair climbing, modified Y-Balance Test, the single leg squat, the single leg hop test, a test of core endurance, and active range of motion (ROM) for knee flexion and extension. (Appendix 1).
Appendix 1, “Return to Activity and Work Test Battery” displays all of the patient’s demographic information, date of testing, patient’s age and/or date of birth, date of surgery and surgeon. The form is divided into specific tests which includes the test name, the examiner and additional recommendations based on test scores. The description of each test and the directions for each test are also included. A summary is included at the end of the form in order to provide patient recommendations for which additional treatments or progression should be addressed.
Detailed surgical preoperative and postoperative protocols were followed for all patients. These protocols included preoperative medical evaluation, nutrition evaluation, multimodal pain management, tranexamic acid administration at surgery, systemic and local antibiotics, DVT aspirin prophylaxis for surgery except those requiring prescription anticoagulants, and overnight hospitalization for observation of medical concerns or complications.1,21,22 The operative procedure involved preoperative MRI Visionaire TM (Smith and Nephew, Andover, MA) planning for patient specific cutting blocks at surgery and the Smith and Nephew Journey II BCS (Smith and Nephew, Andover, MA) prosthesis. This prosthesis was cemented for both the tibiofemoral and patellar components. Postoperatively, all participants were seen by the operating surgeon within 48-96 hours after surgery.
Rehabilitation was initiated within 24-48 hours following surgery. The goals of the first twelve postoperative weeks of rehabilitation were to restore knee motion without limitations and to resolve pain and swelling (Appendix 2). Rehabilitation included active and passive ROM exercises, patellar mobilizations, early weight bearing and gait training, and open and closed kinetic chain exercises. Initial objective testing was completed at three months postoperative and when deficits were identified, the protocol was adjusted to include remedial exercises. Participants were re-tested at six months postoperative for all objective parameters. Results of the six-month postoperative testing dictated either a return to activity or additional rehabilitation. At twelve months postoperative, participants completed a follow-up evaluation, including analysis of all physical, recreational, and work activities.
RESULTS
Group One: Clinical Outcome Results of TKA in Younger Active Participants
Group 1 included 51 participants (54 knees) with a mean age of 58 ± 7 years and a follow up evaluation of 4.4 ± years (3.4-5.6 years). The participants completed a mean of 14 ± 6 supervised physical therapy sessions in addition to a home exercise program. The follow up data indicated no significant complication of infection, pulmonary embolism, or prosthetic loosening on radiographs. Physical examination showed no cases of knee instability or knee arthrofibrosis.
There were statistically significant improvements of the CKRS and KOOS JR scores. The CKRS patient perception rating on a 10-point scale improved from 2.0 ± 1.1 points to 8.2 ± 1.9 points (p< 0.0001). The patient reported CKRS ratings for pain and swelling before and after surgery are shown in Table 1 A and B. The KOOS JR score improved from 43 ± 18 points to 87 ± 18 points after TKA (p< 0.0001).
Patients were asked to list all physical, recreational, and work activities that they participated in after surgery. These were compared pre- and post-operatively to determine patient capabilities. Results after TKA indicated that 44 of 51 participants (86%) resumed some level of physical activity and work without limiting symptoms. The specific reporting activities were determined in a subgroup of 41 patients with 91% performing low-impact recreational activities and 9% performing higher-impact activities (patient choice and not recommended by the medical staff). Of importance, 83% of participants had the ability to take a brisk 20-minute walk five days per week (Table 2A) and 85% of participants were able to participate in 20 minutes of vigorous aerobic activity (Table 2B).
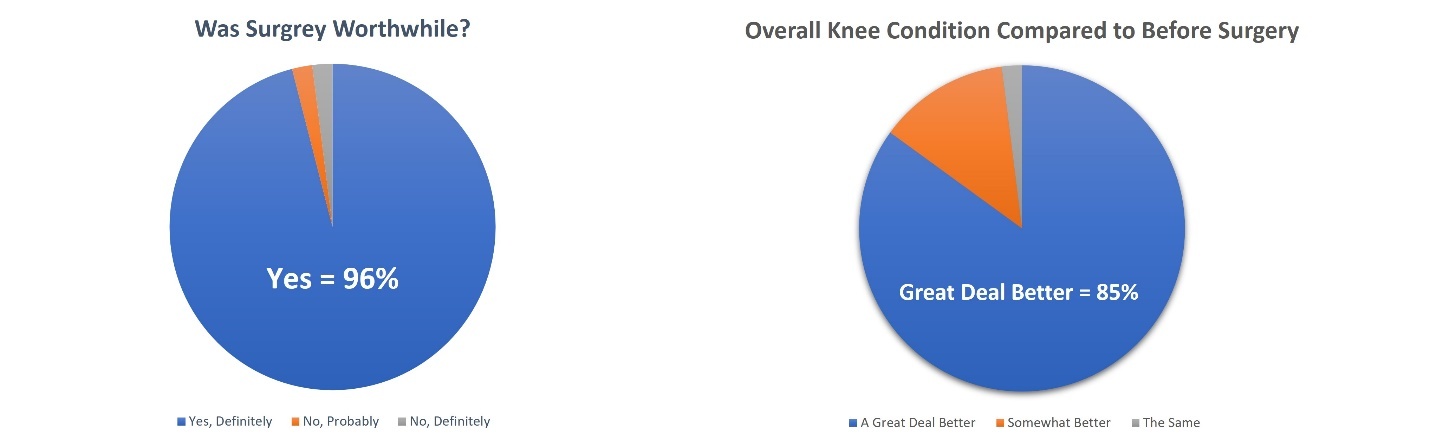
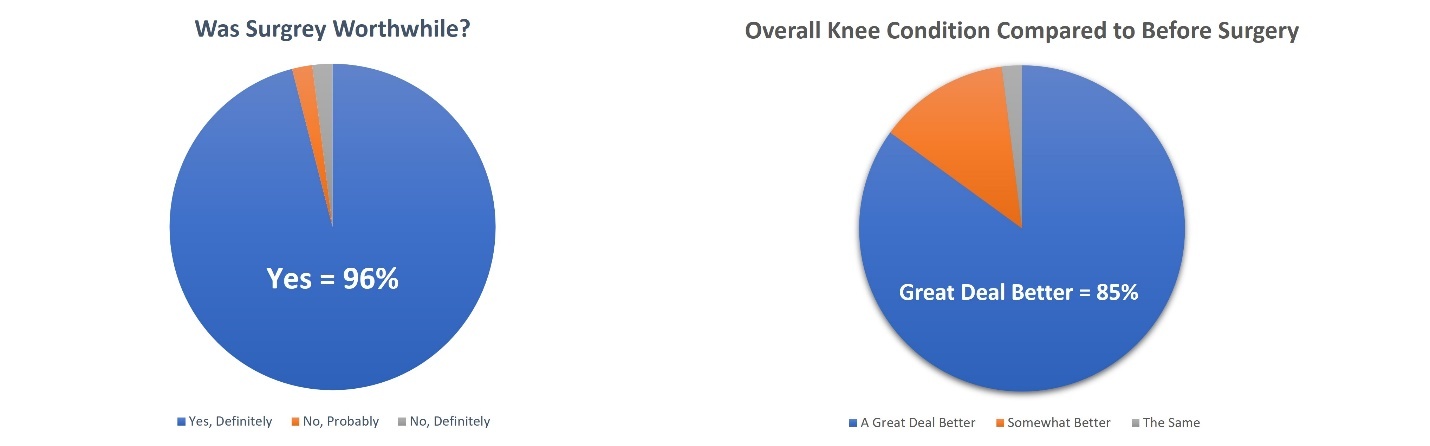
The overall patient expectation regarding the value of TKA surgery and subsequent improvement in knee condition following the procedure can be found in Figure 1.
Group Two: Results of Objective Testing of TKA in Younger, Active Participants for Return to Physical Activities
Group 2 included 50 participants (50 knees) with a mean age of 57.5 +/- 6.5 years. The participants in Group 2 completed 21 ± 8 supervised physical therapy sessions in addition to a home exercise program. Results from each test are identified and included in Table 3 (range of motion), Table 4 (strength) and Table 5 (function). The target goal of each test was scored as “pass/ fail” and whether the participant met the intended goal. Each established goal or criterion for “pass” or “fail” is included in the table. Functional testing included either distance, time, or comparison to the opposite (nonsurgical) knee except for single leg squat which had a qualitative description for the participant to match. Single leg squat was evaluated for overall impression, trunk posture, pelvis control, hip joint and knee joint.23 When the goal was met, the participant was graded as “pass”, but if it was not met, the participant was graded as “fail”. For strength testing, “pass/fail” was graded on the participant’s ability to reach the goal of 70% of the opposite (nonsurgical) lower extremity. Lastly, active ROM used target ranges (0° or hyperextension for extension and ≥130° for flexion) for the determination of “pass/fail”.
It is important to note in this study that there were no cases of knee arthrofibrosis, however seven of the 50 participants (14%) developed early postoperative stiffness despite a highly supervised rehabilitation and home directed program. One participant required an early knee arthroscopy and lysis of adhesions at two months postoperative. All participants identified with early knee ROM stiffness underwent additional interventions to address flexion and/ or extension tightness. Normal ROM was regained in all instances.
DISCUSSION
Younger TKA patients are commonly seeking a return to higher levels of functional activity and hoping to do so with minimal risks than older patients. The purpose of this study was to look at methods which would provide objective criteria to all patients to return safely to this level of activity. There is a tendency to discharge patients from physical therapy at approximately twelve weeks post-operative after TKA. While subjective reports of doing well are common at this point, the results of this study show a relatively small percentage of patients are able to pass a panel of objective testing. It is this panel of tests which provide the necessary objective results to identify whether a patient would be physically ready to resume a higher level of recreational and/or work-related tasks.
A structured program was utilized to assess all possible adverse issues. This involved initiating early weight bearing, active and passive ROM exercises, detecting any decrease in patellar mobility, and beginning both open and closed kinetic chain strengthening exercises. A longstanding benchmark is the return of knee motion from 0-90 degrees by four weeks and not waiting for six or eight weeks for this to occur. Achieving sufficient ROM is necessary for achieving full functional status. A lack of full knee extension creates functional limitation by creating changes in gait, increasing loading of the quadriceps mechanism, and creating a functional “short” limb. Restrictions in full flexion create limitations of descending stairs, taking shoes on/off, and difficulty rising/lowering to a chair. Range of motion is important to achieve early in the rehabilitation process (minimum of 0-90° by four weeks post-operative and full 0-130° by twelve weeks post-operative). Table 3 shows the progression of ROM improvement in Group 2 for three, six, and twelve months post-operative. For those not achieving those goals, specific treatment programs were put in place.
Because knee extension is of great importance to function, many programs include specific knee mobilization programs to regain knee extension and flexion that are initiated immediately postoperatively. Arthrofibrosis may be avoided in patients by addressing limitations of knee motion early and having an effective daily knee mobility program to be completed at home. For example, managing an early limitation in knee extension often involves “hanging weight” programs not only at therapy, but also six times per day at home. The weight should produce a moderate stretch, but not a painful stretch for a compliant program to occur. The “cold” measurements of knee motion at the beginning of the clinical treatment are considered to be the available functional ROM the patient is using during their activities of daily living (ADLs). Programs for knee flexion limitations are also important. The use of mechanical overpressure therapy emphasizing low load, long duration, high frequency stretching can also be appropriate.13,16 A lack of patient compliance in their home treatment program is also a primary concern in cases of arthrofibrosis.
A potential cause for failure of early knee motion programs after TKA is inducing pain and swelling by implementing programs that are too vigorous. There is a delicate balance between exercises and mobilizations being assertive and not allowing for pain and swelling to dissipate. An added medical program to reduce postoperative soft tissue swelling and early limitation of knee motion is frequently required. In resistant cases, prescribing appropriate anti-inflammatory medication (such as a short-term course of oral steroids or dose pack) can be implemented. It is important to have a multimodal pain management program initiated during the first days after surgery, as long-term use of opioid medications is avoided.
In the authors experience, knees that fail to respond and have a persistent lack of knee flexion or extension at four to six weeks, advanced treatment may need to be included.8 Gentle knee manipulation under anesthesia (MUA) can be performed during this time frame after TKA and avoids the necessity of higher-force MUA at 8 to 12 weeks postoperative to regain range of motion. This helps to avoid forceful tearing of the surrounding soft tissues. Earlier use of knee manipulation allows the knee to be taken through a full ROM with only low forces to protect the collagen and immature scar tissues. Patellar mobility can also be restored in all directions.
If a hard stop is present at end ROM, an arthroscopic debridement and lysis of adhesions may be necessary to restore knee motion in cases where motion is not returning. One participant received an early arthroscopic lysis of adhesions at two months post-operative. Normal ROM was achieved by this patient. A case-by-case analysis should be completed and not waiting till the traditional 12 to 16 weeks postoperative before providing appropriate treatment. The goal is to prevent permanent ROM deficits.8
Another critical component of physical function after TKA is lower extremity muscle strength, specifically quadriceps and hamstring strength. While early post-operative emphasis after TKA is pain and swelling management, range of motion, and gait, it is important to achieve functional ADL strength. Results of Group 2 show that at three months post-operative, approximately 50% of patients lacked sufficient functional strength to resume physical activity. However, by 6-12 months post-operative, the majority of patients achieved functional strength (defined as ≥ 70% of the opposite lower extremity). Strength goals were achieved by providing regular objective testing and then adjusting the rehabilitation to add remedial exercises to the program. In cases where significant muscle weakness is noted, the addition of blood flow restriction training can be included in the early stages of the rehabilitation program.24 Recent publications on the use of blood flow restriction therapy show the beneficial effects of implementing this treatment early postoperative, assuming no medical contraindications.24,25 After the initial 12 weeks of therapy, assuming return to normal ADL function, added rehabilitation is necessary for the successful return to greater demands including recreational activities and cardiovascular conditioning.
Total knee arthroplasties are now being performed on younger and more athletically active patients that have major expectations to return to physical activities and an active lifestyle. In Group 1, pain had resolved in 85% and swelling in 92% of patients one year after surgery. Additionally, 83% of patients were able to take a brisk 20-minute walk five days per week and 85% indicated an ability to perform 20 minutes of vigorous aerobic activity three days per week. A panel of objective function tests were identified for screening with Group 2. These tests included ROM and strength, but also included tests for balance, stair climbing, endurance walking, and single leg squatting. Significant function deficits were evident at three months post-operative with gradual improvement occurring over the 6-to-12-month time frame. One anomaly to this panel were the scores for the single leg squat test. Even at 12 months post-operative, only one third of the patients were rated as “good” (as defined by the authors). This test likely was the most challenging as it required single leg control in multiple planes. Therefore, in determining a patient’s return to activity recommendations, the surgeon and physical therapist must rely on a confirmation of both subjective input from the patient (PROMs) and objective testing (ROM, strength, function) to determine appropriate readiness.
Activities that are desired to return to by those having had total joint arthroplasties are primarily low impact recreational activities and include walking, climbing, bicycling on level surfaces, swimming, doubles tennis and golf.26 High impact sports that risk implant survival are not commonly advised. Low impact activities involve many different types of strenuous loading conditions on the lower limb and knee joint which require rehabilitation to return muscle strength, full motion, coordination, and endurance. Ultimate patient satisfaction is based on the patient achieving these expectations for an active lifestyle. The ability of the patient to pursue American Heart Association (AHA) guidelines for a healthy lifestyle remains an important goal.17,18,26
A systematic review evaluated studies regarding the ability of patients to perform recreational activities including sports and recreational activities after TKA and to determine if the activities were symptomatic.7 Nineteen published studies met the inclusion criteria, comprising 5179 knees with a mean age of 67.5 years and a mean 4.8 year follow up after TKA. There was a marked difference in the outcomes among studies regarding the number of patients that resumed recreational activities. Return to activities ranged from 34 to 100%. There was also a low number of patients, 0-16% that were reported to meet AHA guidelines for aerobic physical activity.7,26 This is contrasted to the results of the current study in which participants met a minimum of 75% function goals at twelve months postoperative, except for the 6-minute walk and single leg squat tests indicating that a continued focused exercise program is recommended for further development of strength and cardiovascular endurance even at a year after surgery.
Kuijer et al conducted a similar analysis of TKA studies and reached a conclusion that there is a lack of information and data providing objective criteria to identify a patient’s ability to safely participate in their desired activity.27 Therefore, to achieve AHA guidelines at a fitness level of 150 minutes per week of moderate intensity or 75 minutes of vigorous physical activity, criteria-based screening is necessary.17,18 There are multiple rehabilitation protocols to achieve this level of safety and symptom-free return to physical activities.1 The primary strategy is to base the return to physical activity on passing objective tests of ROM, muscle strength, balance, and function using published test batteries.28 An example of a test battery used in the study is shown in Appendix 1. Equally important are guidelines for the return to work following TKA.29
LIMITATIONS
The objective evaluation of the participants’ muscle strength was measured using the Biodex Dynamometer (Shirley, NY). While there are significant benefits from using this device, its cost makes it difficult to purchase for many healthcare facilities. Utilization of handheld devices would be the next best thing, with manual muscle testing (MMT) the least desirable option. The isokinetic dynamometers have standardized norms for age, sex, and body weight making these numbers ideal. While preoperative data is beneficial, the objective numbers were not used during the comparisons to determine pre to postoperative progress. Due to the protocol of testing through a full year postoperative, participant loss was encountered. Additionally, testing at 24 months postoperative would also be able to identify what participants would be able to retain, insuring continued safe participation in recreational activities.
The need for total knee arthroplasty surgery will continue to increase over time. As life expectancy continues to increase, the benefits of expanding studies to include the age group above 65 years of age and the need for objective testing will also be necessary. In addition, exploring the relationship between preoperative and postoperative outcomes would also help to determine the benefits of postoperative rehabilitation services. Additionally, expanding the preoperative programs to include education/ evaluation for nutrition, fear avoidance and existence of co-morbidities could also be studied to determine their exact role in treatment success.
CONCLUSIONS
A structured and tailored rehabilitation program for TKA patients achieved high patient satisfaction and return to recreational activities. Despite subjective improvement noted in Group 1, significant functional deficiencies noted in Group 2 indicate that careful consideration is needed regarding discharge from rehabilitation for patients who desire a return to an active lifestyle. Major objective improvements occurred at 6 to 12 months postoperative that allowed patients to achieve return to activity guidelines in this relatively younger population.
Disclosures
Institutional support from Smith and Nephew to conduct the study.
Timothy P. Heckmann, PT, ATC: ROMTech – Stock