Introduction
The radiocarpal joint is crucial to hand and wrist function. It connects the forearm to the hand and is essential for movements of the wrist. Wrist movements that allow lifting, gripping and twisting all require functional use of the radiocarpal joint.
Anatomy of the Radiocarpal Joint
The radiocarpal joint is a biaxial ellipsoid joint, meaning that it has two degrees of freedom resulting in wrist flexion and extension, and radial and ulnar deviation. The distal radius articulates with the scaphoid and lunate carpal bones. The distal portion of the radius has two concave surfaces for articulation with the scaphoid and lunate. The distal radius has an indirect articulation with the triquetrum via the triangular fibrocartilage complex (TFCC). As these bones have no actual muscle attachments, they form what is known as an intercalated segment, meaning they are dependent on the forces from muscles crossing their joints to create movement.1
The Role of MSK Ultrasound in Radiocarpal Joint
Advantages
- Non-Invasive: Musculoskeletal Ultrasound (MSKSUS) is a non-invasive imaging technique that can be used for the examination of the ligaments and bones of the distal wrist.2
-
Real-Time Imaging: Structures such as the radiocarpal joint and the scapholunate ligament of the dorsal wrist can be evaluated with MSKUS.
-
High-Resolution Visualization: Detailed images of the radiocarpal joint and the associated ligaments can be attained with MSKUS.3
- Accessibility and Cost-Effectiveness: MSKUS is portable, widely available, and less expensive than magnetic resonance imaging (MRI).
Limitations
- Operator Dependency: MSKUS requires skill and experience for accurate interpretation of findings. The ability to sonograph the distal portion of the wrist is largely influenced by the operator and the availability and technical considerations of state-of-the-art equipment.
- Depth Limitations: While increased depth may limit visualization of structures, superficial wrist structures are generally visible.
- Artifacts and Shadows: Bone and calcifications may create image artifacts, requiring adjustments in transducer positioning and frequency.
Sonographic Technique for Evaluating the Radiocarpal Joint
Equipment Setup
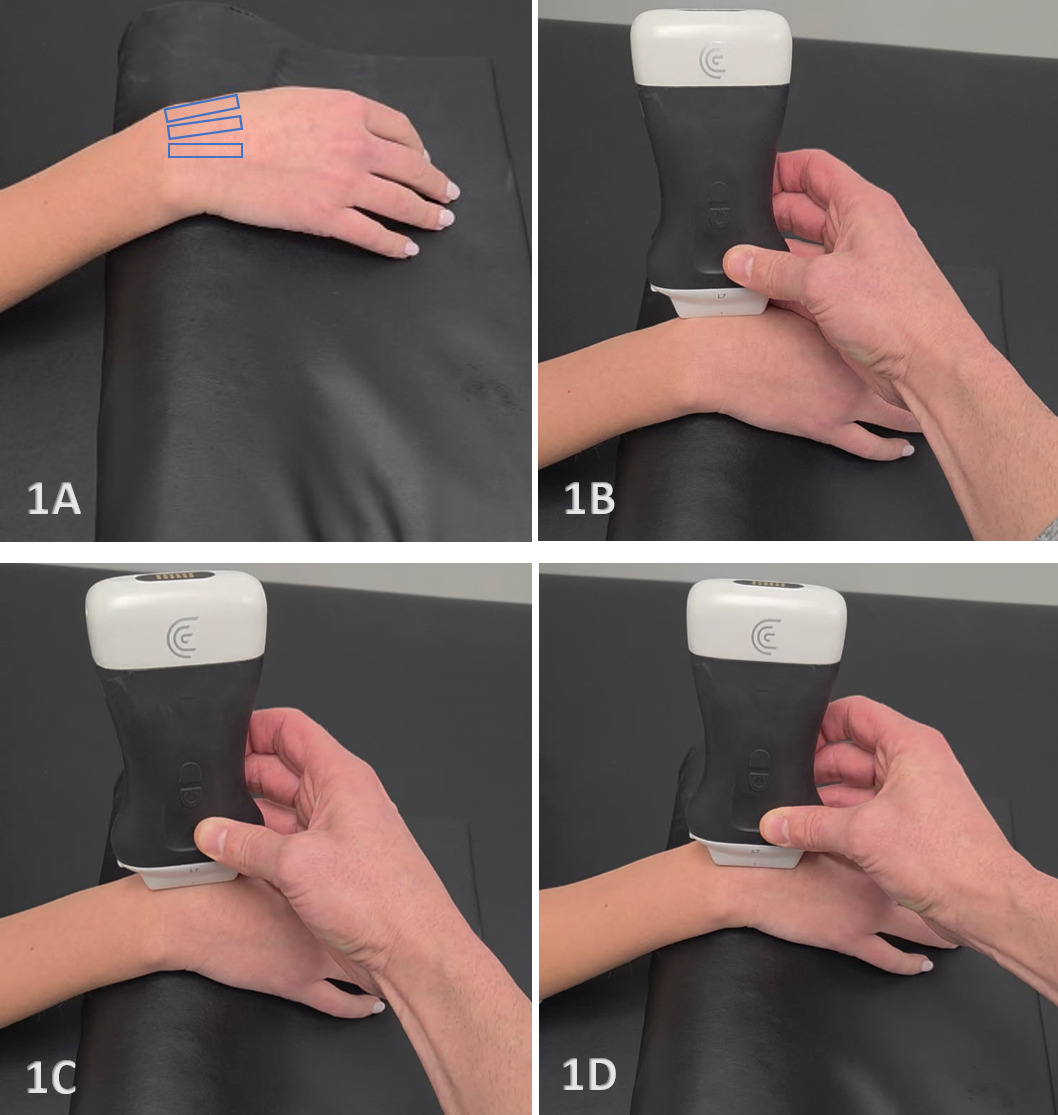
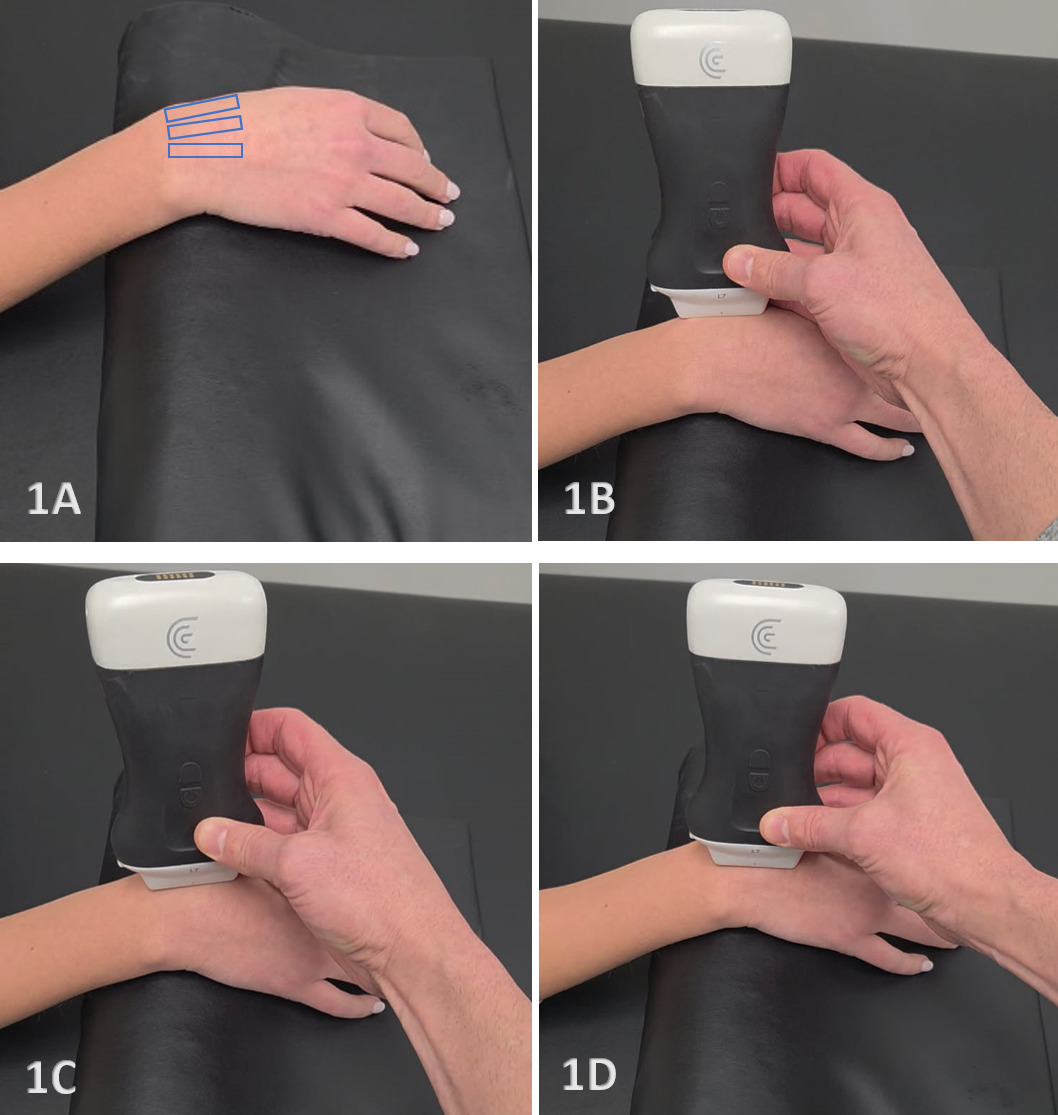
- Transducer Type: Because of the superficial nature of the wrist structures, a standard high-frequency, linear array transducer is normally used. In some instances, the L-shaped, hockey stick-type transducer may be required.
-
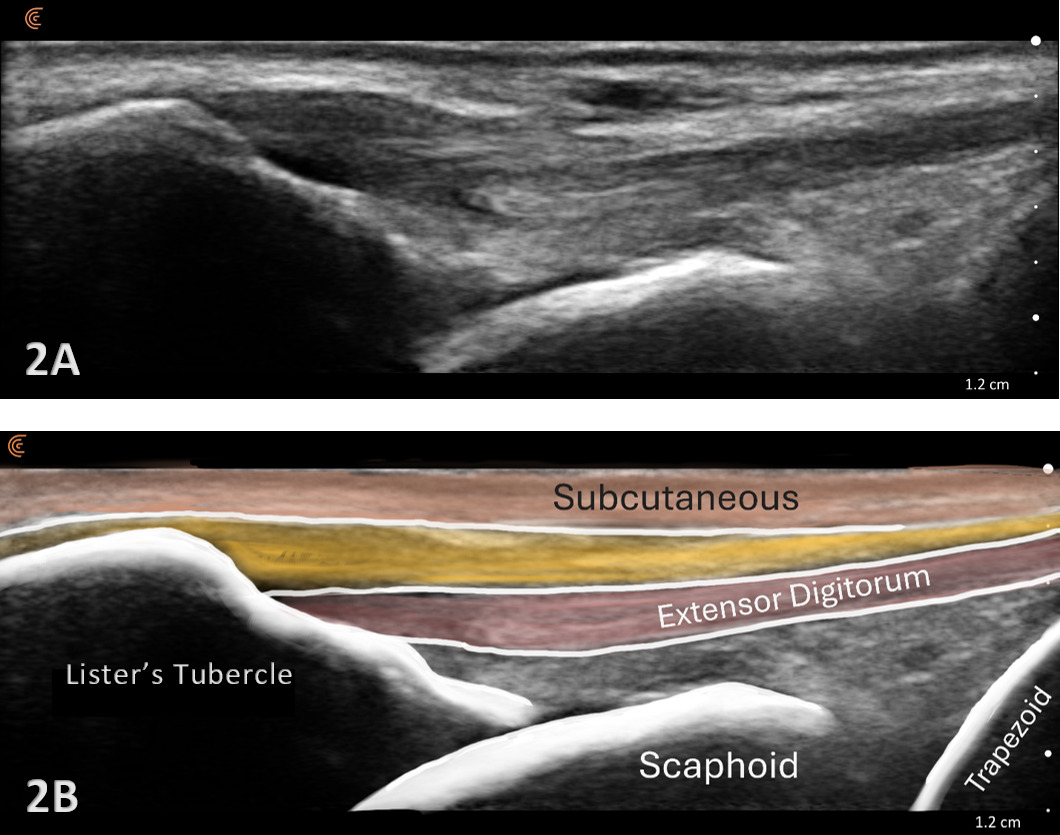
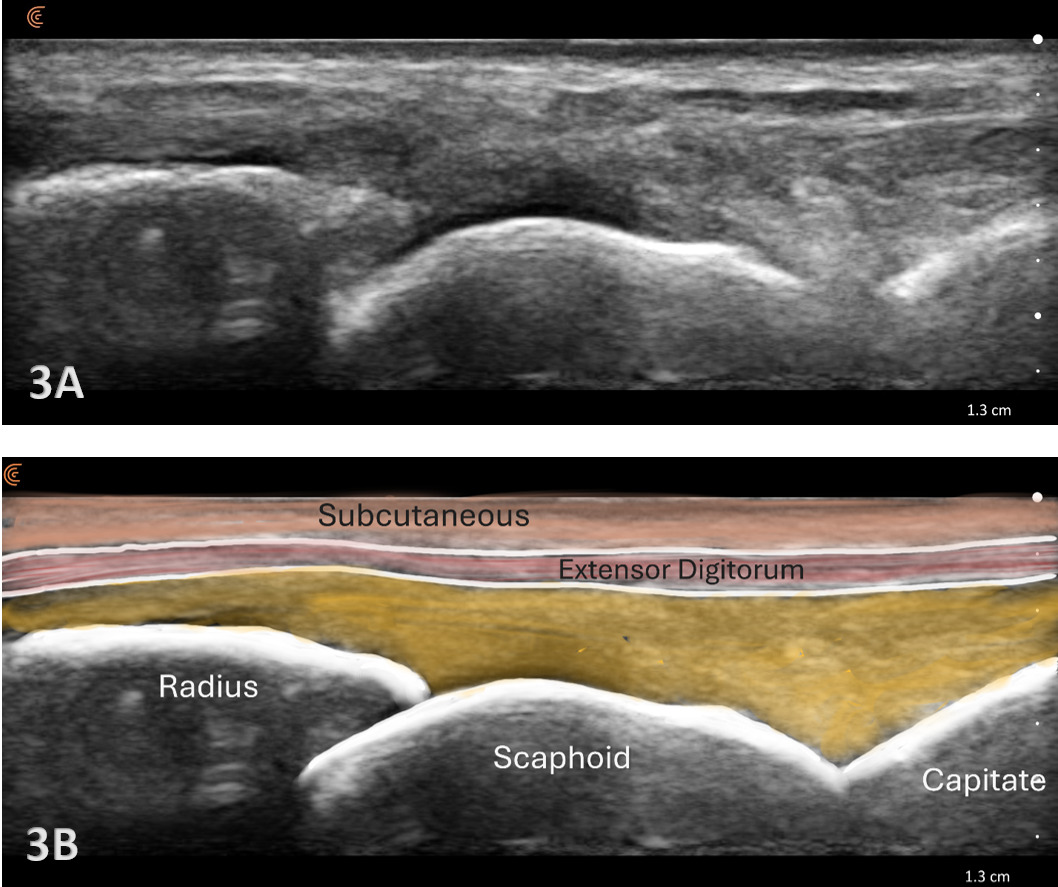
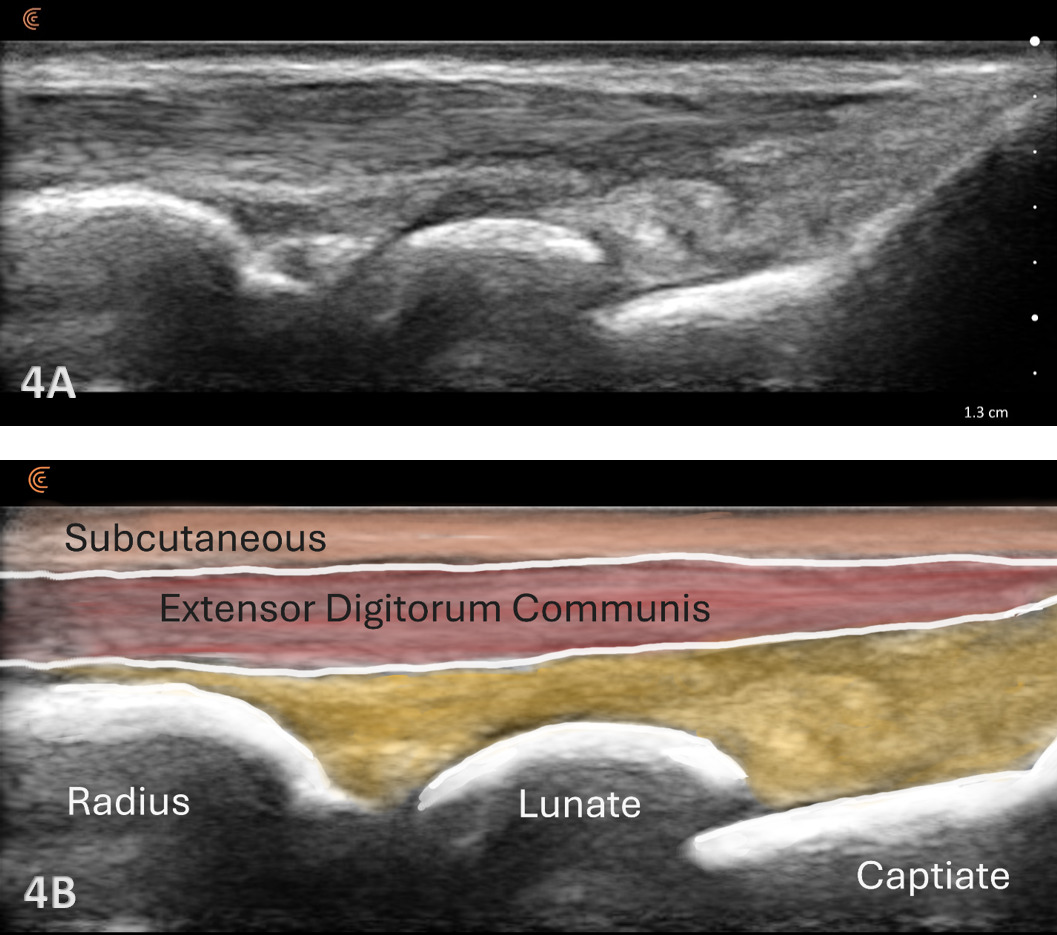
Patient Position: The patient is typically sitting with the volar forearm on the surface with the dorsal wrist facing superior. The dorsal surface is normally viewed as the structures are more superficial and easier to visualize. The transducer is placed in long axis (LAX) to view the radiocarpal joint, while, short axis (SAX) is used to view the scapholunate ligament.
-
Dynamic Assessment: Dynamic views of the wrist can be performed by having the patient flex or extend while visualizing the dorsal tissues and bones.4
Normal Sonographic Appearance
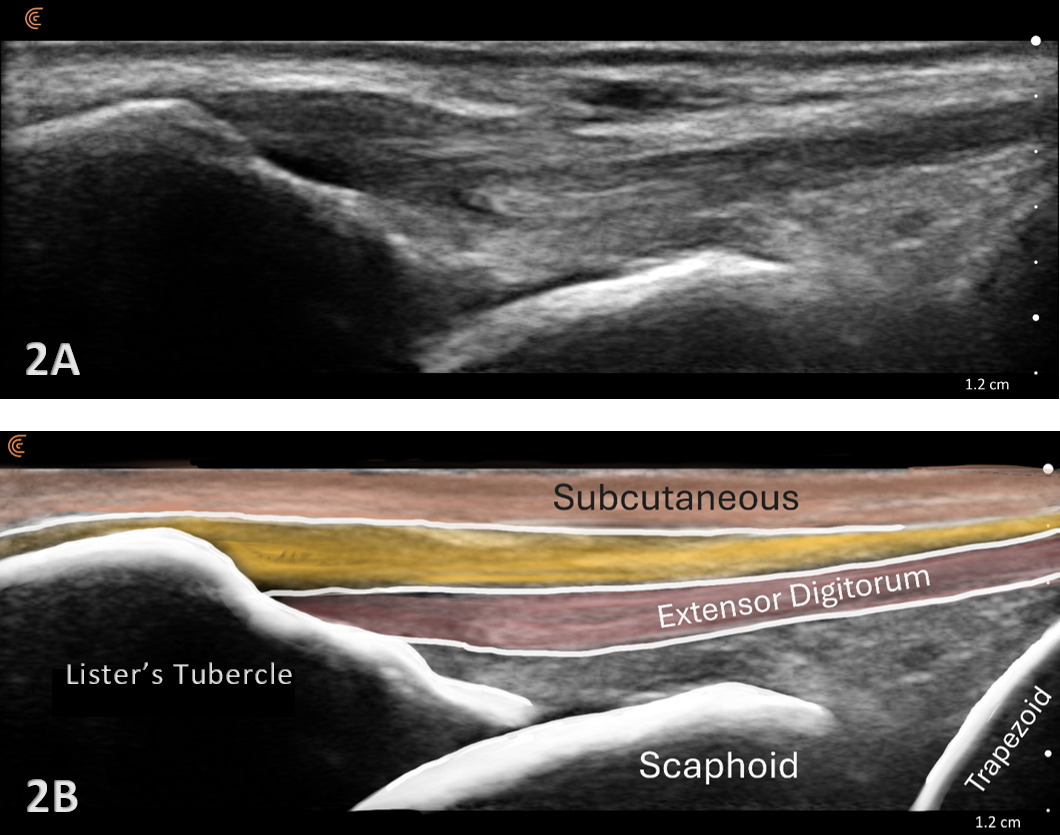
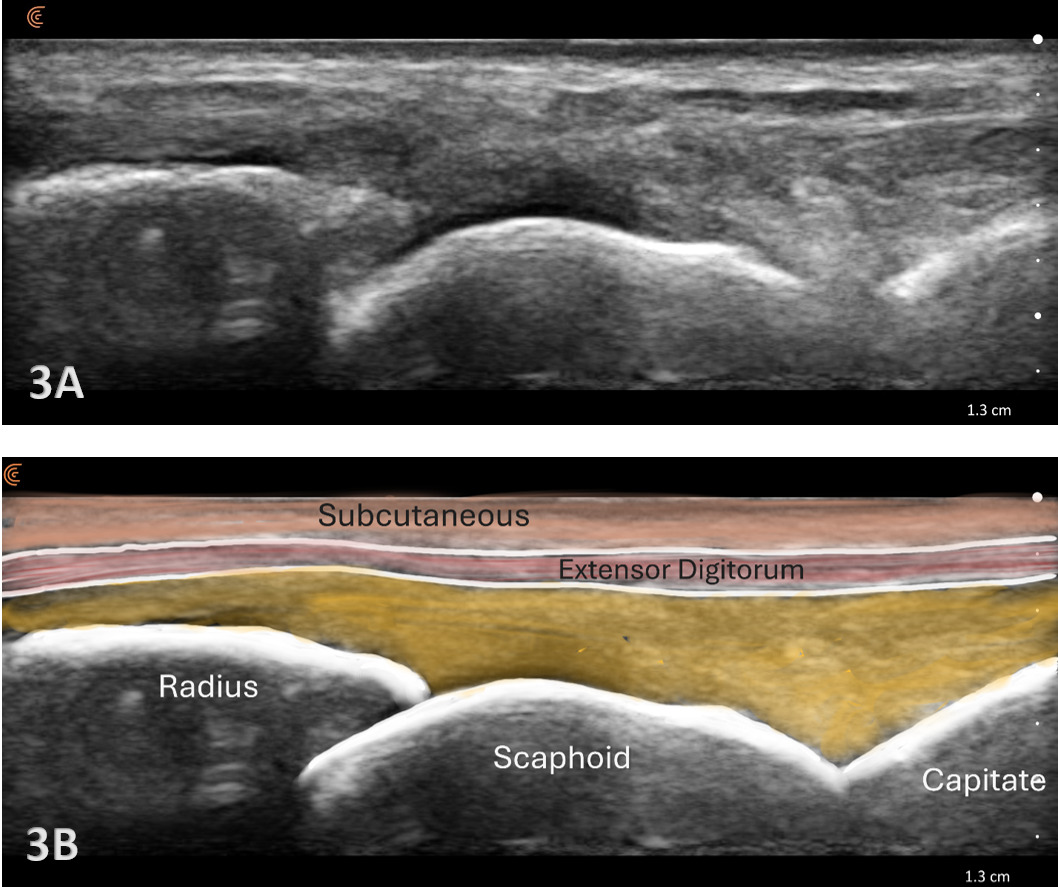
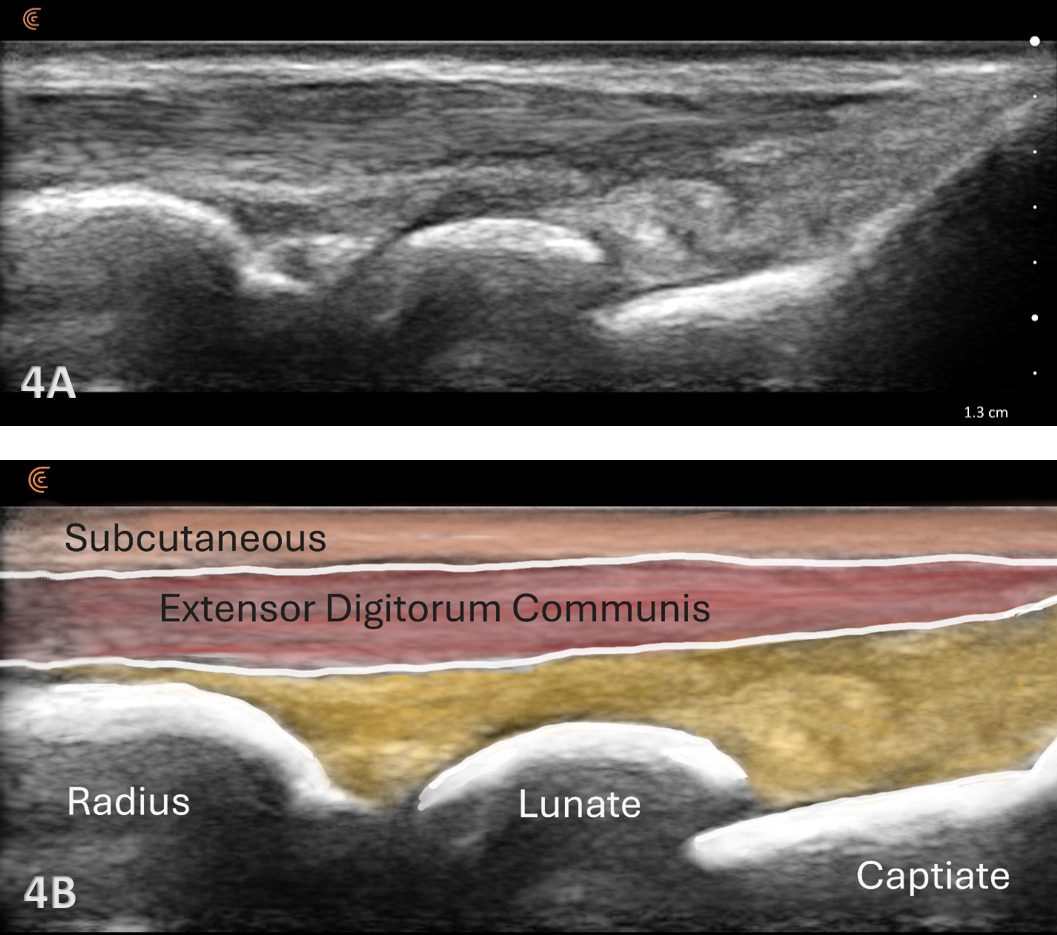
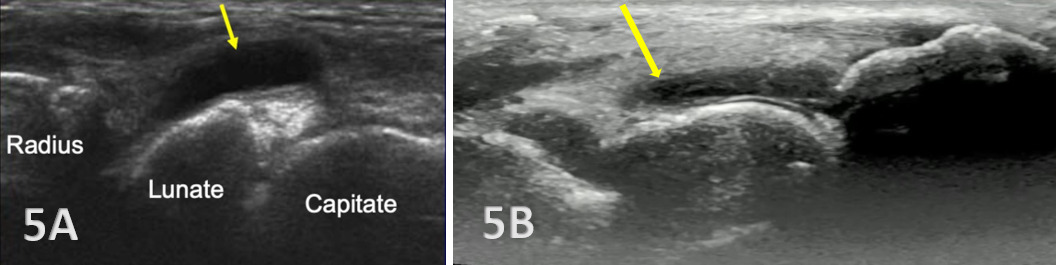
Typically, the radiocarpal joint is viewed in both the LAX and SAX. Typically, there is no joint effusion; therefore, the joint recess is collapsed or barely visible on ultrasound. The capsule should be thin and not distended. The dorsal ligaments are normally continuous and should exhibit a normal fibrillar pattern, indicating they are intact and healthy. The synovium is typically visualized as a very thin echogenic line, with no synovial hypertrophy. The articular surfaces of the radius and the carpal bones should include uniform anechoic or hypoechoic cartilage layers and demonstrate smooth, continuous hyperechoic cortical lines with no physical breaks or breaches.
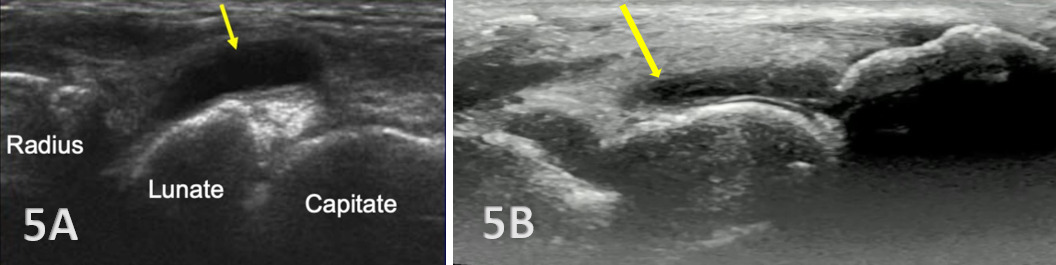
Pathologic Findings in Injured Radiocarpal Joints
-
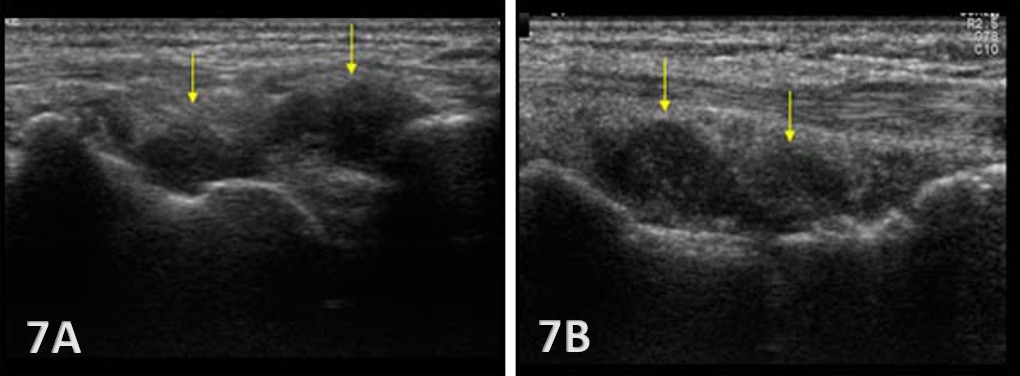
Hyperechoic irregularities of bone of the radius, scaphoid, and lunate are visible.
-
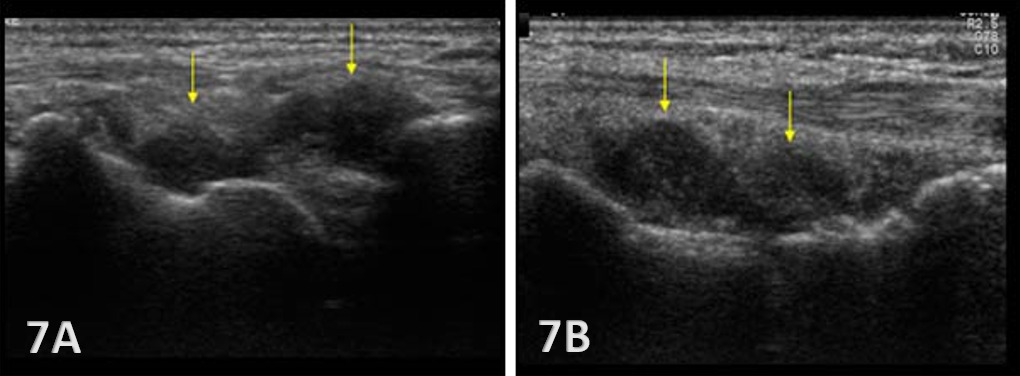
Hypoechoic bands of synovial tissue folds are present.
-
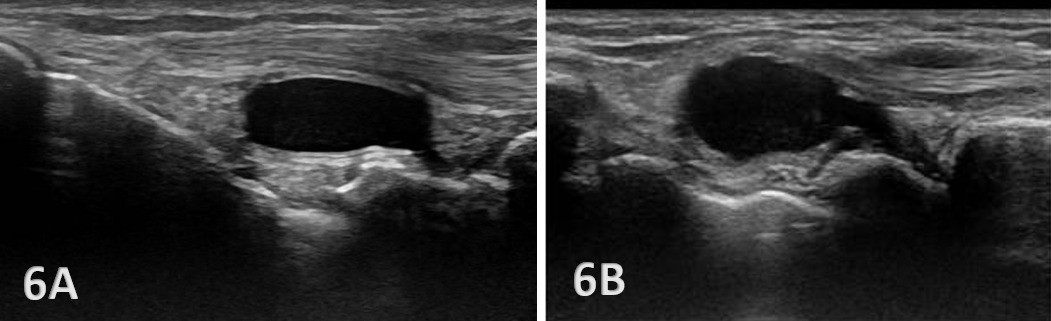
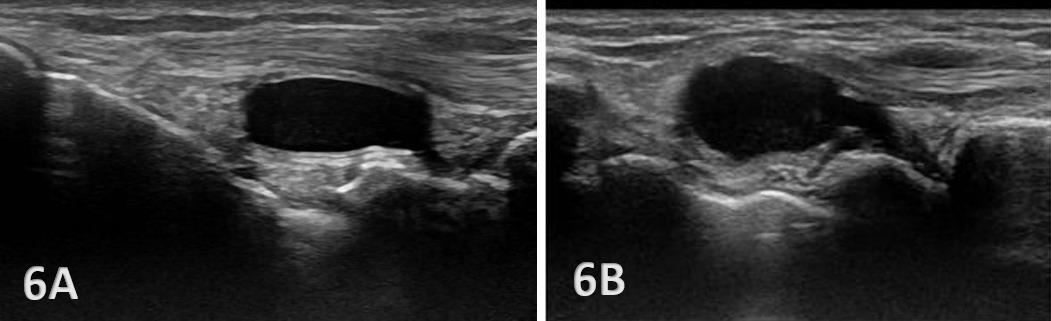
Anechoic or hypoechoic joint effusion and/or synovitis (synovial hypertrophy) and cysts within the joint.
Joint effusion is somewhat compressible and mobile when transducer pressure is applied to the area. This is different from synovitis, which appears as hypoechoic or isoechoic, non-compressible tissue within the joint recess. Synovitis may be associated with conditions such as rheumatoid arthritis, psoriatic arthritis, or other inflammatory arthropathies. Lastly, a ganglion cyst may appear as a well-defined, round or lobulated cystic structure with anechoic or hypoechoic internal contents. The cyst will usually have a small, smooth wall and exhibit posterior acoustic enhancement. These cysts will typically be minimally or non-compressible and painful.
Clinical Implications for Rehabilitation Providers
MSKUS provides real-time feedback for rehabilitation professionals, facilitating early diagnosis of injury and intervention. Key applications include:
-
Early Detection of Injury / Accurate Injury Grading: MSKUS can detect small anechoic or hypoechoic fluid collections in the radiocarpal recess that may be invisible to the naked eye. Finding this early will help guide treatment planning. Additionally, small ligament sprains or partial tears may be seen on ultrasound as irregular loss of normal fibrillar patterns.
-
Dynamic Functional Testing: Rehabilitation professionals can use MSKUS to dynamically stress the tissues with gentle wrist motion to reveal instability or soft tissue impingement between bones or abnormal findings such as cysts.
-
Guided Interventions: Ultrasound imaging assists in dry needling and precision-guided injections, such as corticosteroids for inflammation or treatment for ganglion cysts.5
-
Patient Education: Real-time imaging serves as a visual aid to explain the nature of the injury and set realistic expectations for recovery.
LIMITATIONS AND CHALLENGES
Despite its advantages, MSKUS cannot entirely replace MRI for complex cases. Additionally, the expertise required for optimal imaging techniques limits its immediate adoption across all rehabilitation settings.
Conclusion
MSKUS is a valuable, dynamic, and cost-effective imaging modality for evaluating the radiocarpal joint. It provides high-resolution, real-time visualization of bones, cartilage, and soft tissues in both acute and chronic settings. Ultrasound allows visualization of dynamic wrist movement. Incorporating MSKUS into the physical therapists’ clinical practice for distal wrist examination enhances diagnostic accuracy, supports timely management decisions, and ultimately improves patient outcomes in cases of suspected radiocarpal injury.