INTRODUCTION
Rapid change of direction (COD) is key in multidirectional sports, such as football, basketball, and rugby.1 However, rapid COD is often associated with lower extremity injuries.2 During the weight acceptance phase of COD, greater knee abduction and internal rotation moments significantly increase strain on the anterior cruciate ligament (ACL).3 Specific high-risk movement patterns, including lateral trunk lean, excessive knee valgus, extended knee posture, wide foot placement, and elevated ground reaction forces (GRFs), have been shown to elevate the ACL injury risk during COD tasks.4 Insufficient trunk control has been linked to increased lateral trunk motion, greater knee valgus, and heightened ACL loading during high-speed maneuvers.5 Lateral trunk motion shifts the center of mass (COM) outside the base of support, thereby lengthening the moment arm of the GRF vector relative to the knee joint center. A laterally directed GRF vector relative to the knee joint center amplifies the coronal plane moment arm, thus exacerbating valgus and rotational loads on the knee joint.6
Asymmetries in lower-limb functional performance have been widely proposed as a potential risk factor for sport-related injuries. However, a systematic review concluded that the evidence remains inconclusive, largely due to methodological heterogeneity across studies.7 Despite the fact that many injury prevention programs have concentrated on changing technique to reduce these high-risk mechanics through technique modification and strength training, evidence regarding their effectiveness in addressing interlimb biomechanical asymmetries remains inconclusive.8 Limb dominance, typically defined as the preferred leg for kicking or initiating tasks, may influence neuromuscular control strategies and alter trunk behavior during cutting. The evidence is still inconclusive, according to a systematic review, because biomechanical asymmetries between the dominant limb (DL) and non-dominant limb (NDL) differ among sports and study populations.2 Emerging data suggest that traditional definitions of dominance, such as preferred kicking leg, may not fully represent the limb most at risk of ACL injury, especially in male athletes.9
Previous biomechanical studies on COD task have been focused on lower-limb kinematics and kinetics.10,11 However, investigation of trunk kinematics and trunk muscle activation is still needed to achieve a better understanding of integrated trunk-lower limb mechanics, especially regarding variation with limb dominance and cutting angle. Trunk motion is essential for COD performance, since lateral trunk lean and inadequate trunk stability are associated with greater knee valgus and higher ACL stress during directional changes.5 Proper trunk positioning is crucial for maintaining whole-body balance and minimizing knee joint stress, as poor trunk control can lead to excessive lateral trunk motion, increased knee valgus, and greater ACL loading during high-demand movements.12,13Although its significance, only a limited number of research have investigated trunk kinematics or neuromuscular control during cutting tasks, and none have simultaneously assessed trunk muscle activation across various cutting orientations and across DL and NDL. This gap emphasizes the necessity for a more comprehensive assessment of trunk and lower-limb mechanics during COD.
Moreover, the biomechanics of COD are strongly influenced by the direction and angle of the cut, as sharper cutting angles increase braking demands, lateral propulsion forces, and joint loading.10,14 Additionally, recent reviews highlight that cutting angle substantially alters mechanical and neuromuscular demands, which is critical when assessing injury risk and return-to-sport readiness.10,15 Sharper cutting angle increased braking and lateral propulsion forces, altering the magnitude and direction of joint loading.2 Because of this dynamic complexity, a multifactorial analysis that simultaneously takes trunk control, movement angle, and limb dominance into account is necessary. From a clinical perspective, these insights are crucial for injury prevention professionals, coaches, and rehabilitation specialists. Programs that incorporate core stability and bilateral change of direction training may reduce the risk of ACL injuries and improve sport-specific performance.16 Therefore, this study aimed to investigate the influence of limb dominance and cutting angle on trunk and lower limb biomechanics and trunk muscle activation during multidirectional COD tasks in male athletes. It was hypothesized that DL and NDL would exhibit notable variations in muscle activation and biomechanics across cutting angles, which could have useful ramifications for training and injury prevention.
MATERIALS AND METHODS
Study design
This study used a cross-sectional observational cohort design to examine biomechanical and muscle activity characteristics during side-step cutting tasks.
Participants
Twenty male collegiate athletes were recruited for participation in this study. Participants were recruited through announcements distributed to university soccer, futsal, and rugby teams. Athletes who interest completed a screening questionnaire and were assessed for eligibility.
Inclusion criteria were: (1) male collegiate athletes aged 18–25 years; (2) active participation in an organized university sports team with regular training (three times/week) for at least three months prior testing. Exclusion criteria included: (1) Lower limb musculoskeletal problems in the previous six months prior to the study such as joint pain and muscle pain; (2) History of serious injury or surgery of lower extremity such as fracture, meniscus injury, joint dislocation, tendon or ligament reconstruction; (3) History of low back pain in the six months before the study by receiving medication or physical therapy; (4) History of taking medication related change in muscle properties e.g. muscle relaxant or doping agent within 24 hours prior testing. Limb dominance was defined as the preferred leg to kick a ball.17
Mahidol University central review board approved the research protocol (MU-CIRB 2020/062.2704). Prior to testing, the procedure was explained in detail to all participants, and informed consent was obtained.
Side-step Cutting Test
Side-step cutting was defined as a rapid deceleration followed by a lateral change in direction executed at a specific angle.18 Participants performed side-step cuts at three predefined angles (30°, 60°, and 90°) at maximal effort. Every trial started with a self-selected approach run that was 5 meters long. Before data collection, participants completed a standardized warm-up consisting of a 5-min light jog, dynamic stretching of lower limbs. Three familiarization trials were provided for each cutting angle. The order of testing for the DL and NDL was randomized to minimize potential learning or fatigue effects. A trial was considered invalid and repeated if the participant (1) failed to contact the force plate cleanly with the target foot, (2) altered stride length to intentionally target the force plate, or (3) deviated from the prescribed cutting angle.
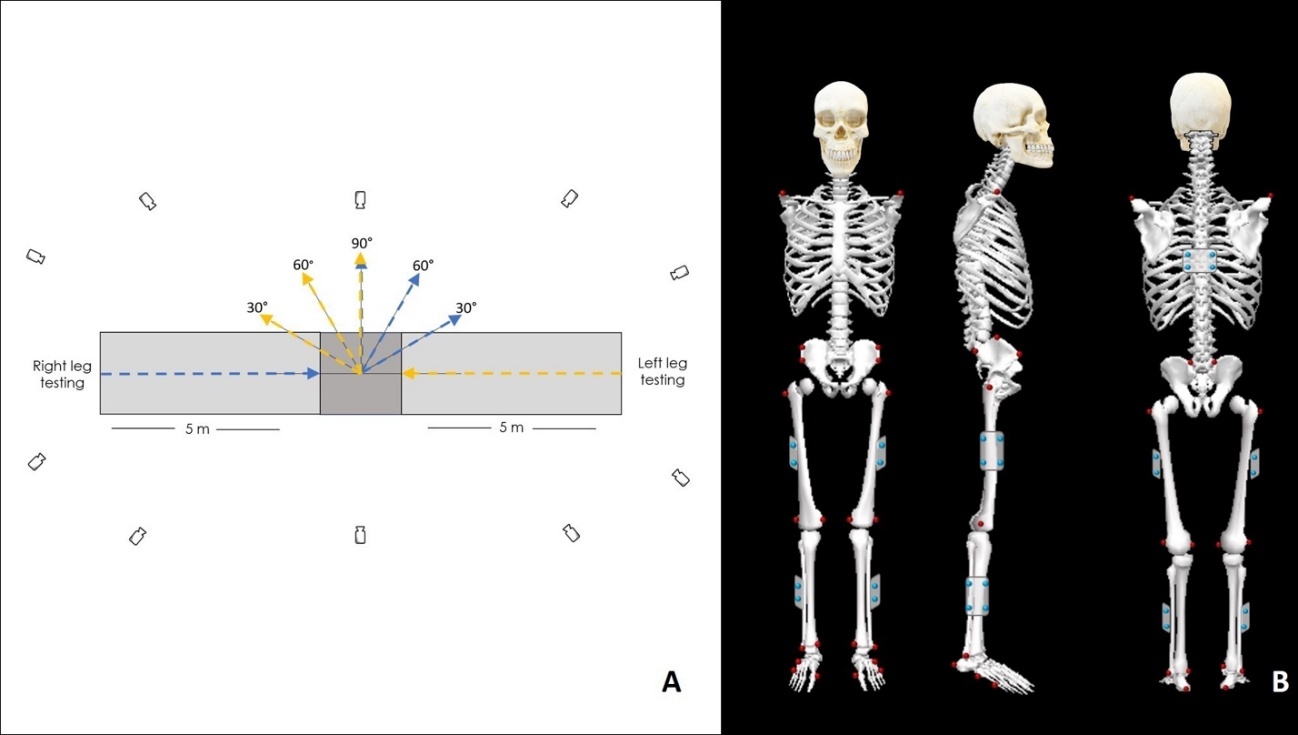
The GRFs and kinematic data were collected using an AMTI force plate (1000 Hz). Three-dimensional kinematics data were collected using 10 video cameras motion capture system (Vicon™, Oxford Metrics, UK) at 200 Hz (Figure 1A). Surface electromyography (EMG) signals were recorded at 1000 Hz using a wireless EMG system (Delsys Trigno, USA).
EMG electrodes were placed bilaterally on the rectus abdominis (RA), external oblique (EO), erector spinae (ES), gluteus medius (Gmed), gluteus maximus (Gmax), rectus femoris (RF), and semitendinosus (ST) muscles in accordance with SENIAM recommendations.19
Following instrumentation, twenty-six reflective markers were attached to bony prominences on both sides including the anterior and posterior superior iliac spines, iliac crest, greater trochanter, medial and lateral femoral epicondyles, medial and lateral malleoli, distal heads of the first and fifth metatarsals, proximal head of the fifth metatarsal, and the heel. In addition, five rigid clusters (four markers each) were positioned on the lateral thighs, lateral shanks, and trunk (Figure 1B). Marker placement followed the Calibrated Anatomical Systems Technique (CAST), a standard method used to identify anatomical landmarks and track segment motion.20
_and_marker_placement_(b).jpeg)
Outcome measures and Data Acquisition
Kinematic variables for the trunk, hip, knee, and ankle were calculated at initial contact and at the instant of peak vertical ground reaction force (vGRF). Net joint moments (NJMs) at the hip, knee, and ankle were computed using inverse dynamics and normalized to body weight. All biomechanical analyses were performed using Visual3D software (C-Motion Inc., Germantown, MD, USA).
Marker trajectories and GRF data were filtered using a fourth-order, zero-lag Butterworth low-pass filter with cutoff frequencies of 6 Hz for kinematic data and 35 Hz for GRFs. Cutoff frequencies were selected using residual analysis to balance noise reduction and signal quality, as recommended in biomechanical signal processing.21 EMG signals were band-pass filtered (30–400 Hz), full-wave rectified, and averaged over the period from initial contact to peak vGRF. EMG amplitudes were normalized to the maximum activity observed during a 10-m maximal forward running task for each muscle and expressed as a percentage of this reference value.
Statistical analysis
An a priori power analysis using G*Power (version 3.1.9.6) determined that 20 participants would provide sufficient power (1-β = 0.80) to detect medium effect sizes (f = 0.25)22 for both main effects and the interaction effect of a two-way repeated measures analysis of variance (ANOVA) with an alpha level of 0.05. For each limb and cutting angles, the mean of three successful trials was used in the statistical analysis. A two-way repeated-measures ANOVA (2 × 3, limb dominance × cutting angle) was used for statistical analysis of all outcome variables. Sphericity was assessed using Mauchly’s test, and Greenhouse–Geisser corrections were applied when violations were detected. For ANOVA effects, partial eta squared (ηp²) was reported and interpreted as small (0.01), medium (0.06), and large (0.14). All statistical analyses were performed using SPSS (version 29.0; IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05.
RESULTS
Twenty male collegiate athletes participated in the study. Participant characteristics are summarized in Table 1. The mean age was 20.0 ± 1.3 years, with a mean body mass index of 22.6 ± 2.3 kg/m². All participants were right-leg dominant and were actively involved in soccer, futsal, or rugby at the collegiate level. All data in the current study demonstrated a normal distribution.
The results of three planes of trunk and lower extremity joint angles at IC and peak vGRF are shown in Tables 2 and 3. No significant interaction effects were seen between limb dominance and cutting angle on lower extremity joint angles at IC. The main effect of cutting angle significantly influenced (p < 0.05) the trunk, hip, knee, and ankle joints at IC. For the main effect of limb dominance, no significant difference between DL and NDL was observed except for the hip abduction angle (p = 0.033, ηp² = 0.073) and ankle external rotation angle (p = 0.039, ηp² = 0.068), with DL cutting being performed with less hip abduction and more ankle external rotation than NDL.
At peak vGRF (Table 3), there was no significant interaction between limb dominance and cutting angle for joint angles. Significant main effects were seen for cutting angles for the trunk, hip, knee, and ankle angles. Regarding limb dominance, there was a significant main effect on trunk flexion (p = 0.034, ηp² = 0.122), ipsilateral rotation (p = 0.032, ηp² = 0.128), and ankle external rotation (p = 0.036, ηp² = 0.149), with the DL showing more trunk flexion, ipsilateral rotation, and ankle external rotation than the NDL.
Table 4 shows NJMs for the hip, knee, and ankle at peak vGRF. There was no significant interaction between limb dominance and direction. Significant main effects were observed for cutting angle regarding hip, knee, and ankle NJMs, except for hip external rotator moment (p = 0.242, ηp² = 0.041) and ankle evertor moment (p = 0.838, ηp² = 0.002), while no significant effects were found for limb dominance.
For core muscle activity (Table 5), significant main effects were seen for RA on both sides (right: p = 0.028, ηp² = 0.122; left: p = 0.013, ηp² = 0.132) and EO (right: p = 0.020, ηp² = 0.320; left: p = 0.031, ηp² = 0.113), whereas no significant main or interaction effects were observed for the erector spinae ES (p > 0.05). Additionally, a significant interaction effect between limb dominance and cutting angle was observed for the left EO muscle activity (p = 0.023, ηp² = 0.240). For lower extremity muscle activity, significant main effects of direction were observed for the Gmed (p = 0.001, ηp² = 0.190) and RF (p = 0.001, ηp² = 0.183), with greater activation during 30° cutting for Gmed and 60° cutting for RF. Limb dominance significantly influenced Gmed activity (p = 0.048, ηp² = 0.110), with NDL showed more activation than DL.
DISCUSSION
The findings support the hypothesis that DL and NDL would exhibit notable variations in muscle activation and biomechanics across cutting angles. This may have useful ramifications for training and injury prevention. A main effect of limb dominance was seen for hip and ankle kinematics at IC (Table 2), trunk and ankle kinematics at peak vGRF (Table 2), and EO and Gmed muscles (Table 4). Tables 2–5 show a significant main effect of cutting angle on kinematic, kinetic, and EMG parameters.
Kinematics
At IC, trunk and lower extremity joint angles varied significantly across cutting angles. The DL exhibited greater trunk flexion and ankle external rotation, whereas the NDL showed increased hip abduction. Although trunk flexion differences approached statistical significance, they did not meet the threshold. These findings support the idea that body posture at IC reflects neuromuscular control strategies critical for impact force attenuation and injury prevention.23
The current study showed that cutting at sharper angles, especially at 90°, resulted in decreased hip and knee flexion while increasing ankle plantarflexion. This pattern is consistent with those in previous studies indicating that sharper angle COD reduces sagittal plane motion and increases mechanical demands in the frontal and transverse planes.10,24 Trunk flexion was also greater at 60° compared with at 30°, indicating that athletes try to maintain momentum and COM under sharper COD.14,25 Less trunk, hip, and knee flexion increase GRFs and anterior shear forces at the knee, thereby increasing ACL loading risk.26,27
At peak vGRF, the movement patterns were similar to those at IC; however, the NDL exhibited greater trunk rotation toward the stance limb, whereas the DL rotated more toward the intended direction, along with greater trunk flexion and ankle external rotation in the DL. The NDL exhibited slightly greater hip abduction and significantly increased trunk rotation toward the stance limb compared with the DL. These kinematic differences suggest distinct neuromuscular control strategies between limbs, with the NDL adopting a more upright postural alignment and increased hip abduction. While this kinematic profile may enhance deceleration capacity, it could simultaneously modify knee loading mechanics in the frontal plane, potentially influencing injury risk profiles.28
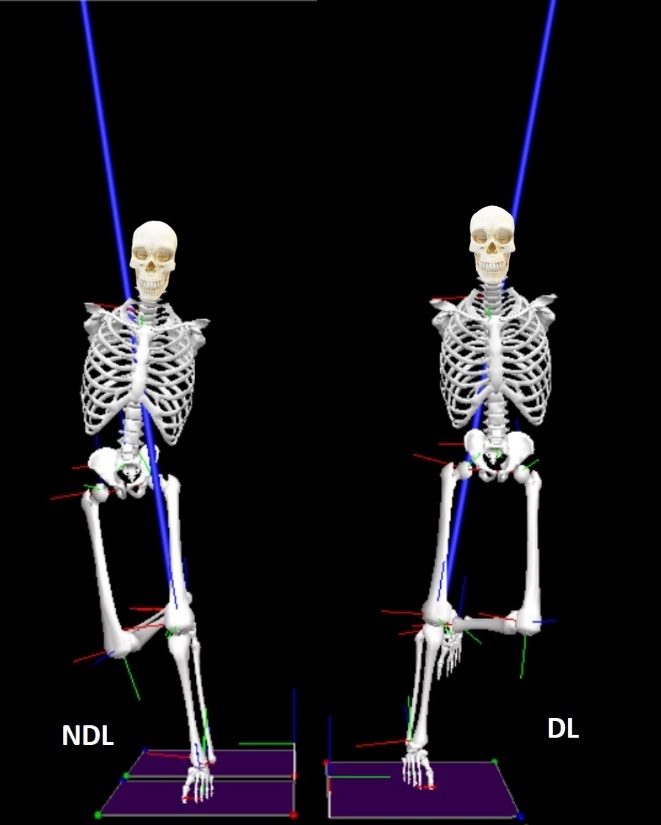
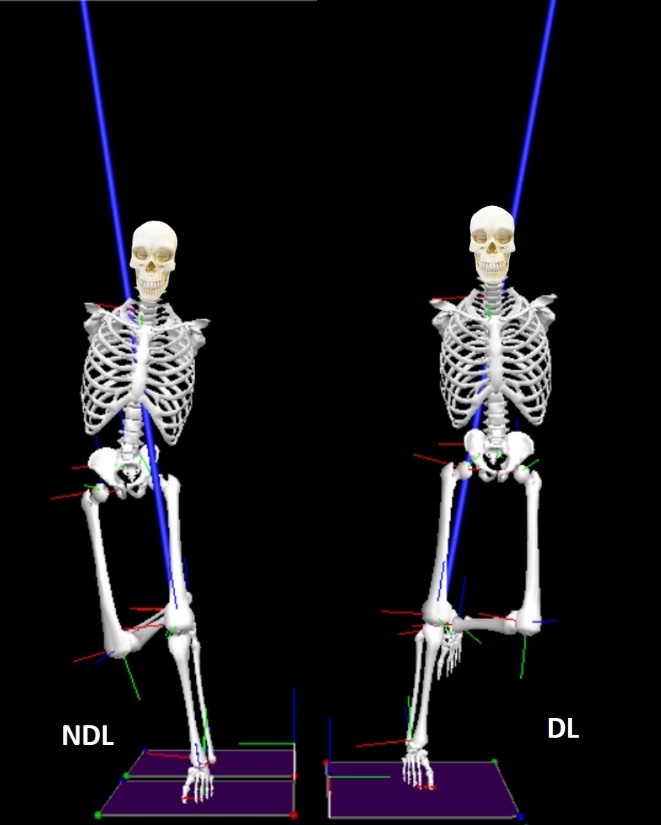
Increased trunk rotation and lateral flexion toward the stance limb during cutting may elevate external knee rotational moments and ACL loading due to altered neuromuscular control and mechanical demand on the knee joint.26,27 Figure 2 illustrates relative movement control of the trunk, pelvis, and lower limb segments during cutting tasks. The NDL appears to assume a riskier position, though compensatory flexion and rotation in the intended direction are recommended for effective vGRF absorption and speed maintenance.27 Hip and knee angles were similar between limbs, suggesting both contribute to stabilizing the joints at peak vGRF. These results indicate that while lower limb joint angles were similar on both sides, differences in trunk and hip strategies might lead to different ACL injury risk profiles.
Kinetics
At peak vGRF, NJMs showed similar patterns between the DL and NDL at the ankle, knee, and hip. However, the DL demonstrated higher magnitudes than the NDL, particularly at the hip and ankle. These differences may reflect greater neuromuscular efficiency in the DL than in the NDL, developed through habitual use in propulsion and braking.29
Although symmetrical joint moments suggest adequate bilateral training adaptations,30 the underlying movement patterns, particularly in the trunk and pelvis, remained asymmetrical. This supports the concept that athletes may use different neuromuscular strategies to produce similar kinetic outputs, which has implications for injury screening and rehabilitation.31
Cutting angle had a profound effect on kinetic patterns. Sharper angles, especially at 90°, led to a proximal shift in load absorption. The present study showed increased hip adduction and internal rotation moments accompanied by reduced ankle plantar flexion moments. This kinetic redistribution indicates a compensatory stabilization strategy, wherein the body selectively engages larger proximal musculature to handle increased mechanical loads. While biomechanically adaptive, this movement pattern may inadvertently elevate ACL loading forces, particularly when executed with restricted hip and knee flexion ranges.26
From a performance perspective, previous studies have shown that greater ankle plantar flexor moments are associated with effective push-off mechanics.32 However, the present study revealed that as cutting angles increase, the contribution of the ankle joint decreased. This reduction likely reflects a compensatory strategy prioritizing stability over propulsion under higher mechanical demands. Such a trade-off has important implications for return-to-sport protocols. Restoring efficient ankle kinetics is not only essential for regaining high-performance capabilities but also for minimizing compensatory loading at the knee and hip, which may elevate injury risk.33
Muscle Activity
The present study demonstrated that cutting angle significantly affected activation of the RA and EO muscles, but not the ES (Table 4). This pattern suggests that, during the braking phase, the trunk was primarily stabilized through flexion and rotation rather than extension. These results contrast with those of Mornieux et al., who reported no significant differences in trunk muscle activity between 30° and 60° cutting tasks.25 The difference might result from methodological variations; Mornieux et al. examined recreational athletes and evaluated trunk activity by a co-contraction ratio of both RA and EO muscles, potentially distorting directional effects.
Greater trunk flexion is thought to aid in positioning the COM over the base of support, thereby increasing downward momentum and potentially attenuating GRF at impact.27 Additionally, an interaction between cutting angle and leg dominance was observed in this study, reflecting underlying neuromuscular asymmetries, as all participants were right-leg dominant. Supporting this, Mornieux et al. also noted increased co-contraction of trunk rotators in the direction opposite to movement prior to executing a 60° COD, highlighting the anticipatory role of trunk muscles in controlling rotational momentum.25
During cutting with the DL, the contralateral (left) EO muscle exhibited greater activation than the ipsilateral (right) EO. This pattern coincided with trunk kinematic data at peak vGRF, which showed that cutting with the DL involved more trunk rotation toward the intended cutting angle; in contrast, cutting with the NDL involved more trunk rotation toward the stance limb. This suggests that athletes may attempt to stabilize the trunk in a more neutral position during the braking phase, with the EO contracting eccentrically to control trunk rotation. These findings are consistent with prior research that showed significant differences in trunk rotational power in asymmetrical sports such as golf, tennis, and ice hockey, where trunk dominance and rotational patterns are sport-specific.34 Although the current findings align with previous work showing sport-specific differences in trunk rotational strategies in asymmetrical sports such as golf, tennis, and ice hockey, the present study did not examine differences between sports. Variation in sport-specific training loads, positional demands, and movement patterns may have contributed to individual differences in trunk and lower-limb mechanics. Because the study was not powered to detect between-sport effects, this remains a potential source of variability and an important avenue for future research.
Concerning lower limb muscle activity, no significant differences were observed between limbs, except for the Gmed. The NDL demonstrated significantly higher Gmed activation than the DL. As the Gmed is critical for accelerating the COM toward the cutting angle by generating medially directed GRFs,35 this increased activity may represent a compensatory effort to stabilize the hip. Interestingly, this activation occurred despite lower hip abductor NJMs, indicating neuromuscular compensation. This pattern aligns with a previous study that identified higher Gmed activity in NDL as a strategy to maintain hip and pelvic stability when mechanical output or strength is weaker on that side.36
The findings of the current study emphasize the role of proximal neuromuscular control in injury risk reduction. Differences in trunk rotation, ankle external rotation, and gluteus medius activation showed that clinician should focus on limb-specific neuromuscular training, particularly for the NDL. This can be accomplished through exercises including hip abductor strengthening, single-leg lateral hop and stabilization, and single-leg deceleration. Furthermore, gradually familiarizing athletes to sharper cutting angles (30°, 60°, and 90°) may facilitate the adaptation to higher mechanical demands while reducing reliance on compensatory trunk strategies.
Limitations and Future Directions
The current study used a planned cutting task that may not accurately represent the unexpected movement demands typical of competitive sports environments, where most ACL injuries happen.37 To accurately replicate game-like conditions, future research should integrate reactive cutting protocols with external stimuli. Variations in approach speed may have contributed to the observed kinematic, kinetic, and neuromuscular responses. Future study should incorporate approach velocity as a covariate or independent variable to better understand its interaction with cutting angle and limb dominance. Moreover, the participants were male collegiate athletes, which restricts the generalizability of findings to female athletes, who demonstrate higher ACL injury incidence.38 Future research should investigate potential sex-specific differences in neuromuscular control strategies during cutting maneuvers.
CONCLUSION
The results of the current study provide evidence that cutting angle has a significant influence on lower limb biomechanics, and that limb dominance introduces subtle yet significant differences in trunk and ankle mechanics and muscle activation. These distinctions may increase ACL injury risk when unaddressed in training. Targeted limb-specific neuromuscular interventions are recommended to mitigate asymmetrical loading and enhance movement efficiency in athletes during high-demand multidirectional tasks.
Corresponding Author
Komsak Sinsurin
Biomechanics and Sports Research Unit, Faculty of Physical Therapy, Mahidol University
999 Phuttamonthon 4 Road, Salaya, Nakhon Pathom 73170, Thailand
Tel: +6624415450, Fax: +6624415454
E-mail: komsak.sin@mahidol.ac.th
Conflicts of Interest
The authors report no conflicts of interest.