INTRODUCTION
The abdominal drawing-in maneuver (ADIM) is widely employed as a representative core exercise that specifically targets the activation of deep trunk muscles, particularly the transversus abdominis (TrA). The ADIM facilitates the isolated contraction of the TrA and has been reported to be effective in re-educating a functionally impaired TrA.1,2 In patients with low back pain, compared with healthy individuals, excessive co-contraction of the entire abdominal wall3 and delayed feedforward activation of the TrA4,5 have been observed. The ADIM has been shown to be effective in correcting such delays.6,7 Furthermore, by drawing in the abdominal wall, the ADIM reduces excessive lumbar lordosis and anterior pelvic tilt, thereby contributing to postural improvement.8 Given these effects, the ADIM has been considered beneficial in alleviating lumbosacral pain and dysfunction2 and is frequently incorporated as a fundamental element of core stability programs.
Intra-abdominal pressure (IAP) refers to the pressure generated within the abdominal cavity, which is surrounded by deep trunk muscles such as the diaphragm and the TrA. Increases in IAP contribute to spinal stability through enhanced lumbar stiffness.9–14 In the context of sports physical therapy and rehabilitation, elevated IAP is considered important as it enhances trunk stability, augments the stiffness at proximal muscle attachment sites of the extremities, and thereby contributes to force production in the limbs.15
While the ADIM is effective as an intervention for low back pain, it may be unsuitable as a breathing strategy during high-intensity exercise tasks. It has been reported that the increase in IAP during the ADIM is limited to 11.7 ± 11.0 mmHg.16 Similarly, IAP elevation during the ADIM or the analogous hollowing maneuver is restricted to 9.9 ± 4.5 mmHg.17 In contrast, abdominal bracing induces an IAP increase of 116.4 ± 15.0 mmHg,17 the Valsalva maneuver in a seated position promotes an IAP increase of 156.2 ± 43.5 mmHg,18 and during a representative high-intensity resistance exercise such as the squat, IAP has been reported to exceed 200 mmHg.19 Moreover, beyond differences in the magnitude of IAP elevation, the use of the ADIM during high-intensity exercise tasks has been shown to impair pelvic, lumbar, and thoracic stability as well as lumbar stiffness compared with conditions without the ADIM.20 Collectively, these findings suggest that the ADIM may be unsuitable for enhancing trunk stability in high-intensity exercise tasks.20
However, previous research examining high-intensity exercise tasks20 has primarily focused on sagittal-plane movements, such as those used in Pilates, with limited consideration of trunk rotation in the horizontal plane. Recent studies continue to explore breathing strategies and trunk stabilization under high-load conditions, emphasizing the role of respiratory mechanics in trunk function; for example, Kawabata and Shima21 demonstrated that abdominal muscle activation and IAP are modulated by the interaction between breathing patterns and postural demands during plank-based tasks. Notably, during trunk rotation torque exertion, strong associations have been reported between IAP and torque output, both in terms of temporal fluctuations (rs = 0.924) and peak values (r = 0.594).18
Trunk rotation in the horizontal plane represents a fundamental component of many functional and sport-related movements, requiring coordinated trunk stabilization and force production.22 Despite this functional relevance, experimental studies examining the interaction between breathing strategy, IAP, and mechanical output during horizontal-plane trunk rotation remain limited. Trunk rotational torque provides a mechanical outcome that reflects the capacity for force generation during rotational tasks and is influenced by trunk stability and muscular coordination,22 yet its relationship with IAP under different breathing strategies has not been sufficiently clarified.
Therefore, the purpose of the present study was to clarify the effects of the ADIM on IAP and torque during trunk rotation. This investigation is expected not only to further elucidate the relationship between IAP and trunk rotation torque, but also to provide guidance on the appropriateness of employing the ADIM in situations requiring trunk rotational torque, including such contexts as sports physical therapy, rehabilitation, and sports performance, thereby offering practical insights for both competitive athletes and recreational sports participants engaging in rotational movements.
MATERIALS AND METHODS
Study Design
This study employed a randomized crossover design to compare multiple outcomes during trunk rotation torque exertion under two conditions. Fifteen healthy, non-athlete young adult males were recruited from a university population through verbal announcements.
Participants
Sample size was calculated using G*Power 3.1 based on a pilot study. With an effect size (d) of 0.80, α = 0.05, and power (1−β) = 0.80, the minimum required number of participants was 15. Eligible participants were men aged 18–30 years with the ability to complete all measurements and a habitual exercise routine of at least 30 minutes per day, twice per week. The exclusion criteria included: engaging in competitive-level sports, experiencing low back pain or pain during trunk rotation within the past three months, a history of severe cardiovascular disease or diabetes, difficulty with catheter-type pressure sensor insertion, and contraindications to bioelectrical impedance analysis (e.g., presence of a pacemaker or metal implants). Based on these criteria, 15 participants were recruited. Participants were instructed to refrain from strenuous exercise or unfamiliar physical activity for 24 hours prior to measurement. Written informed consent was obtained from all participants, and eligibility was confirmed through a physician-supervised interview. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Review Committee of the Graduate School of Sports Sciences, Chukyo University (August 26, 2024, Approval No.: 2024-063).
Procedures
Height was measured in a standing position using a tape measure (SK Hareru Measure 2 m, Niigata Seiki, Japan) affixed to a wall. Body mass and body fat percentage were assessed using a body composition analyzer (MC-180, Tanita, Japan). The participants were instructed to complete meals at least two hours prior and to void the bladder before measurements. Body mass index (BMI) was calculated from measured height and body mass.
IAP was measured using a sterilized catheter-type pressure sensor (MPR-500, Millar Instruments, USA). Rectal pressure, measured approximately 15 cm from the anus, was used as an index of IAP.2 The sensor was immersed in physiological saline for 30 minutes before measurement and treated to prevent drift. A rubber cover (NIKKISO-THERM, Tokyo, Japan) with a small perforation was applied to the sensor,18,23 and it was secured using surgical tape (Micropore™ Skin Tone Surgical Tape, 3M NIKKISO-THERM, Tokyo, Japan). To reduce discomfort during insertion, a topical anesthetic (2% Xylocaine Jelly, Aspen Japan, Tokyo, Japan) was applied after confirming the absence of adverse reactions using a skin patch test, in which a small amount of the anesthetic was applied to the inner aspect of the upper arm.
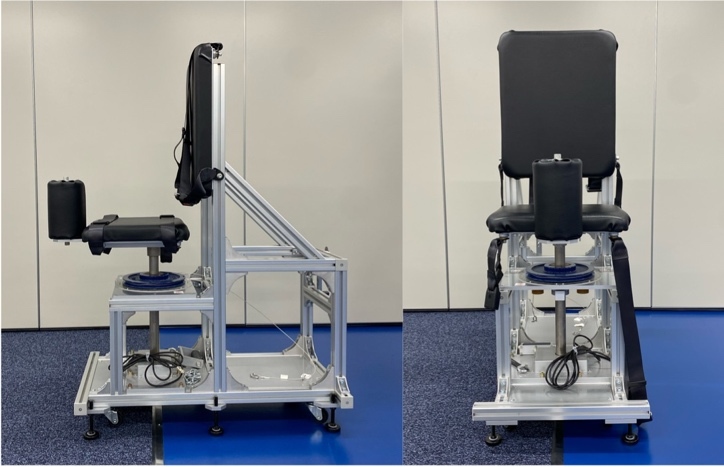
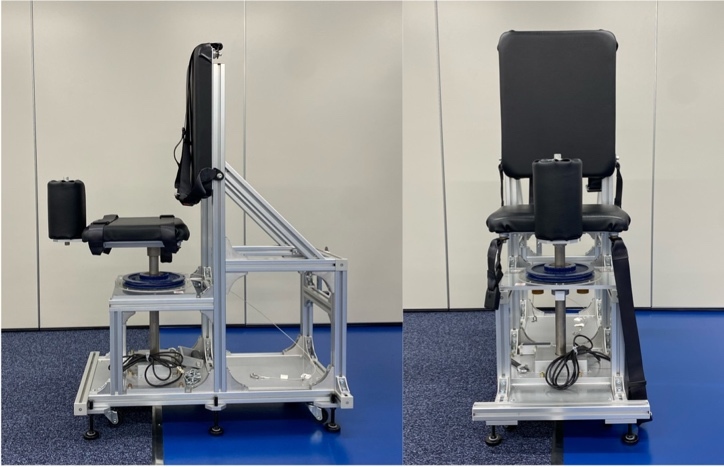
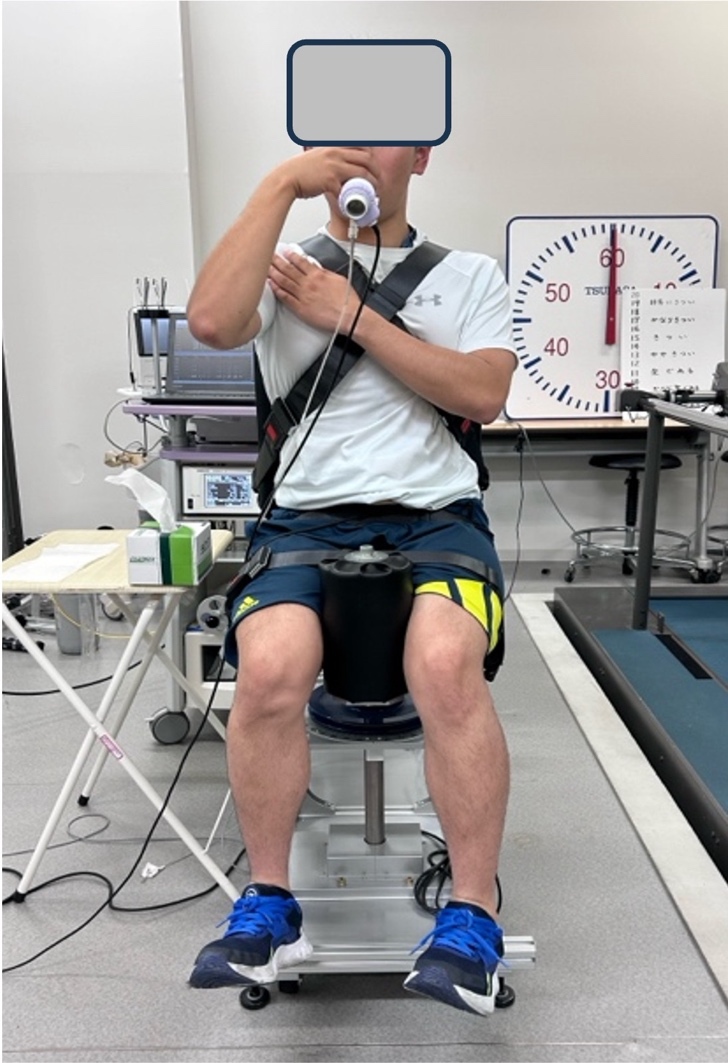
Trunk rotation torque was measured isometrically at a trunk rotation angle of 0° using a custom-manufactured trunk rotation dynamometer (SANKA Co., Niigata, Japan) (Figure 1), developed in consultation with the research group, and a strain amplifier (TSA-210, SANKA Co., Niigata, Japan).18 All trunk rotation trials were performed as maximal voluntary isometric efforts. Two maximal-effort trials were conducted for each condition, and the trial yielding the greater torque value was used for analysis. Prior to testing, participants completed a standardized warm-up and familiarization protocol. Only non-dominant side rotation was performed to minimize fatigue and learning effects due to potential left–right differences in rotational strength.18 The non-dominant side was defined based on self-reported hand dominance (i.e., the hand used for writing), and trunk rotation was performed toward the side opposite the dominant hand. Each 5-second trial, initiated by the experimenter’s cue, included a 2-second ramp-up phase and a 3-second maintenance phase. To prevent compensatory movements, belts securing the thorax, pelvis, and thighs were adjusted to each participant’s body size. The experimenter confirmed that the pelvis was in a neutral position prior to each trial using visual inspection, restricting major trunk posture changes, although small pelvic tilts could not be entirely prevented. Standardized instructions were provided to minimize compensatory motion.
Vital capacity (VC) and inspiratory volume during the Valsalva maneuver were measured using a respiratory gas analyzer (AE-310s, Minato Medical Science, Tokyo, Japan). To prevent nasal breathing errors, a nasal plug was used; if ill-fitting, the participants closed their nostrils manually. VC was measured following guidelines for pulmonary function testing24 and the maximum value of three trials was used. Measured VC was used to normalize inspiratory volume during trials, expressed as %inspiratory volume.
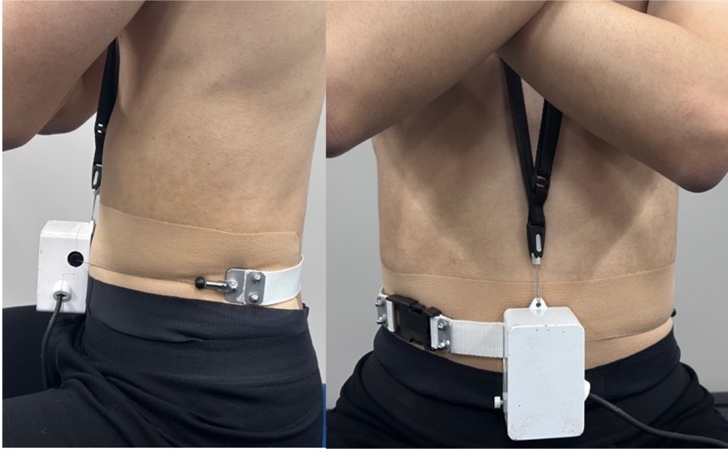
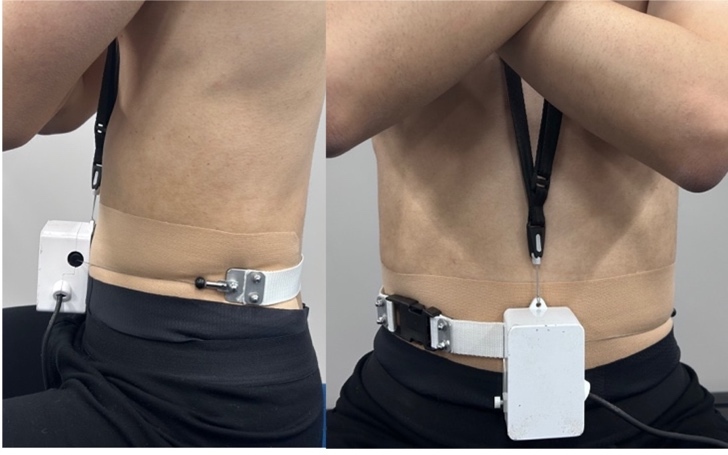
Waist circumference was measured using a thoracic range-of-motion device (SANKA Co., Niigata, Japan). A wire was positioned circumferentially around the trunk between the lower costal margin and the iliac crest (Figure 2). To minimize potential indentation of the abdominal surface, kinesiology tape was applied at the wire contact area prior to measurement. The wire tension allowed detection of relative abdominal expansion and contraction during task execution. A baseline waist value was obtained as the mean of three consecutive measurements within 1 mm at end-expiration in a resting state. Normalized values were expressed as %waist and were recorded at the moment of peak torque in each condition.
IAP, torque, %inspiratory volume, and %waist were measured during trunk rotation torque exertion under the following two randomized conditions:
Spontaneous rotation (SR): no specific instructions regarding the abdomen.
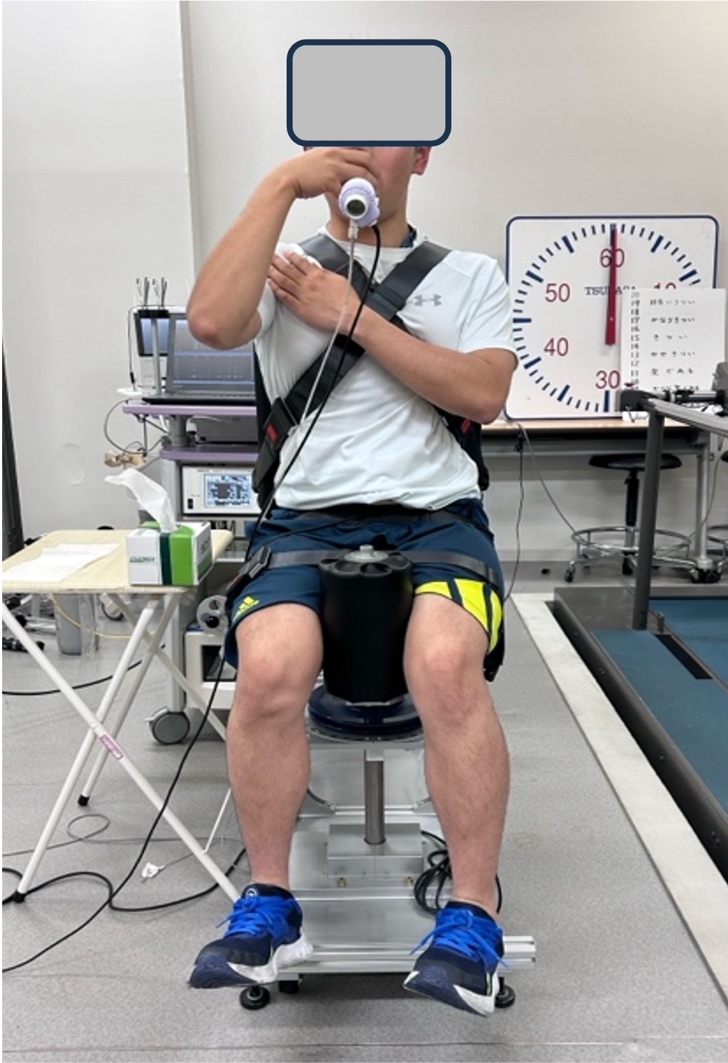
ADIM rotation (DIR): participants were instructed to exhale and maximally draw the lower abdomen inward, following a standardized verbal cue: “draw the lower abdomen inward as much as possible and pull the navel toward the spine.”25 To ensure consistent reproduction of the draw-in maneuver during force exertion, a reduction in waist circumference to below 98% of the individual baseline value was adopted as an operational criterion. This threshold was determined based on preliminary testing to balance feasibility, safety, and reproducibility of the task during maximal effort trials. The criterion was not intended to define the ADIM itself, but rather to confirm execution of the maneuver. The actual magnitude of waist circumference reduction achieved during the DIR condition was quantified and is reported as %waist. Participants were not provided with specific instructions regarding breathing strategy during force exertion. Once the waist circumference criterion was met, the experimenter provided the start cue, and participants exerted maximal voluntary isometric trunk rotation while maintaining the abdominal configuration (Figure 3). Inspiratory volume was measured at the moment of peak torque.
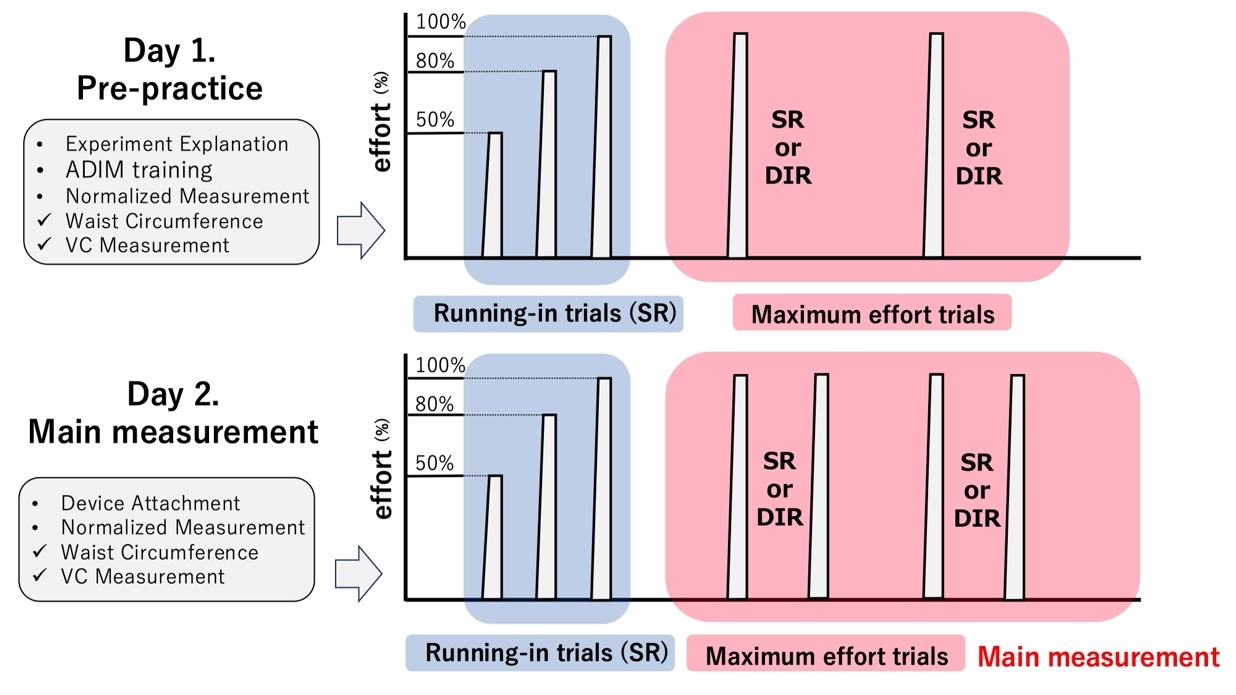
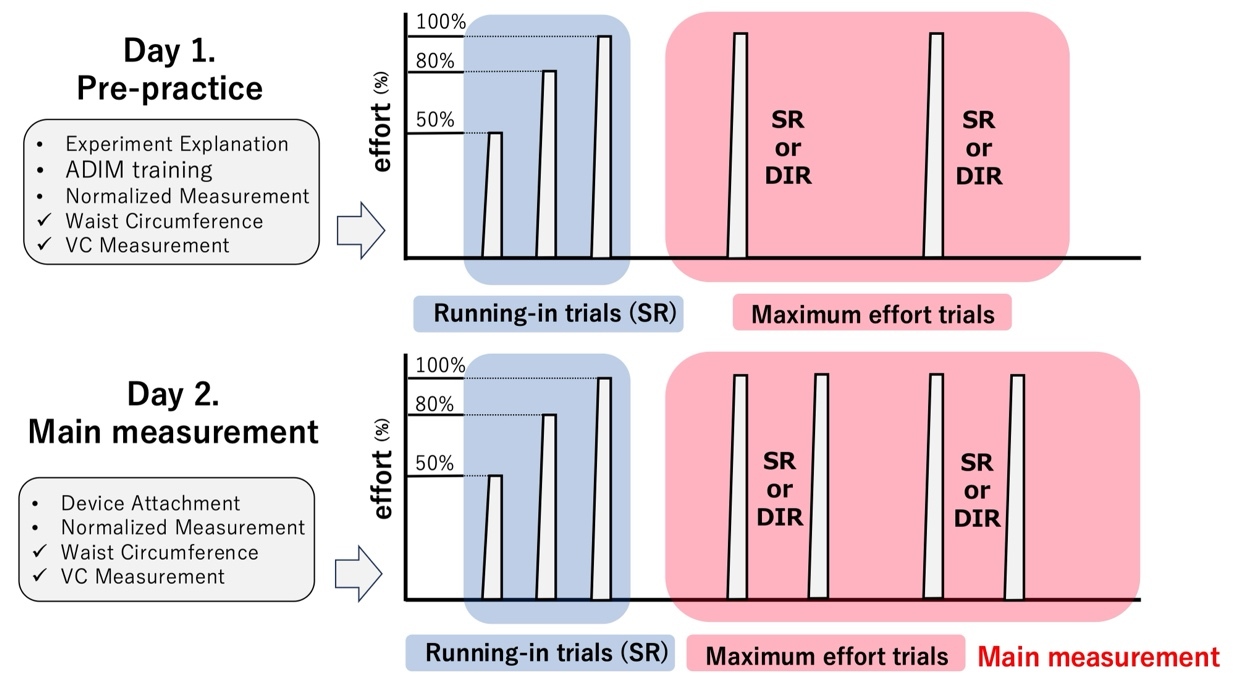
The study was conducted over two sessions: a familiarization day (Day 1) and the main measurement day (Day 2). Familiarization was undertaken to minimize learning effects during the main trials.22 On Day 1, following explanation and obtaining consent, data concerning the participants’ height, body mass, body fat, and BMI were obtained, and patch testing was conducted. DIR was practiced for approximately five minutes, followed by measurement of the baseline waist and VC for normalization. The participants then performed three submaximal practice trials at 50%, 80%, and 100% effort, with ≥1-minute rest between trials. Subsequently, each condition was performed once at maximal effort, with ≥2-minute rest intervals.
On Day 2, at least one day after patch testing, the catheter was inserted for IAP measurement. Measurements followed the same sequence as Day 1: normalization, practice trials, and two maximal-effort trials per condition (Figure 4).
Statistical Analyses
All data were recorded using a 16-bit analog-to-digital converter (PowerLab 16/35, ADInstruments, Sydney, Australia) and analyzed with LabChart software (v8.1.21, ADInstruments). Data were averaged at 200-ms intervals and statistically analyzed.18,26 For each condition, the trial yielding the greater torque was used as the representative value. IAP was defined as the value at the moment of peak torque. Torque was the peak recorded value, and %inspiratory volume and %waist were measured at the moment of peak torque.
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA). Normality of IAP, torque, %inspiratory volume, and %waist was assessed using the Shapiro-Wilk test. Shapiro-Wilk tests for the four outcomes indicated normality for IAP, torque, and %inspiratory volume; thus, paired t-tests were performed. %waist did not meet the assumption of normality and was analyzed using the Wilcoxon signed-rank test. Statistical significance was set at p < 0.05. Effect sizes were based on Cohen’s criteria, with d interpreted as small (0.2), medium (0.5), and large (0.8). r was interpreted as small (0.1), medium (0.3), and large (0.5).27
RESULTS
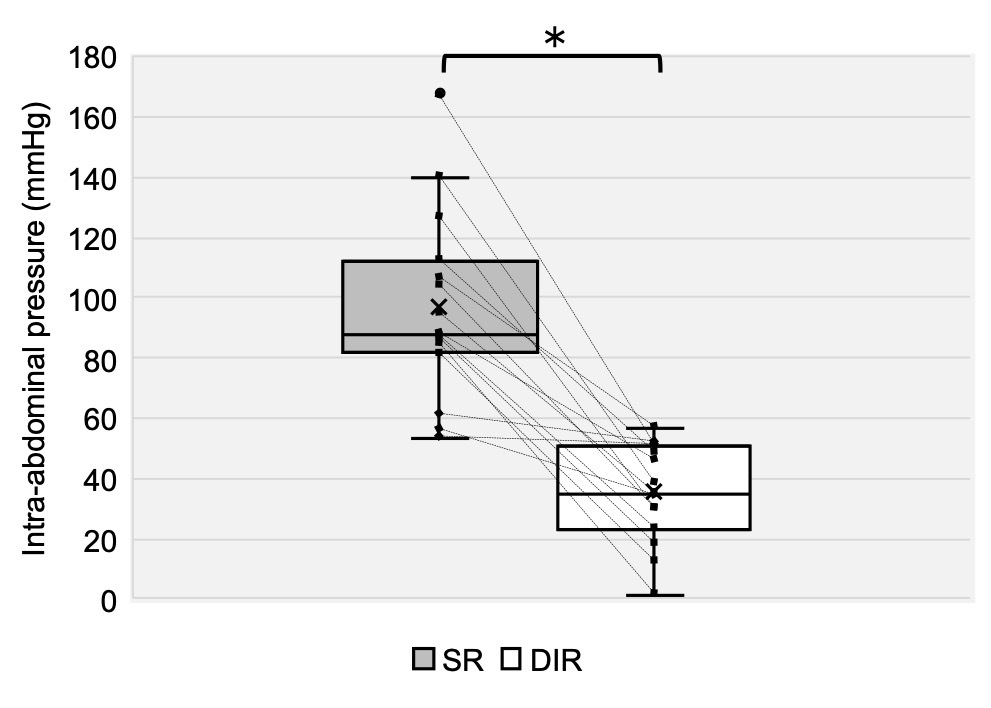
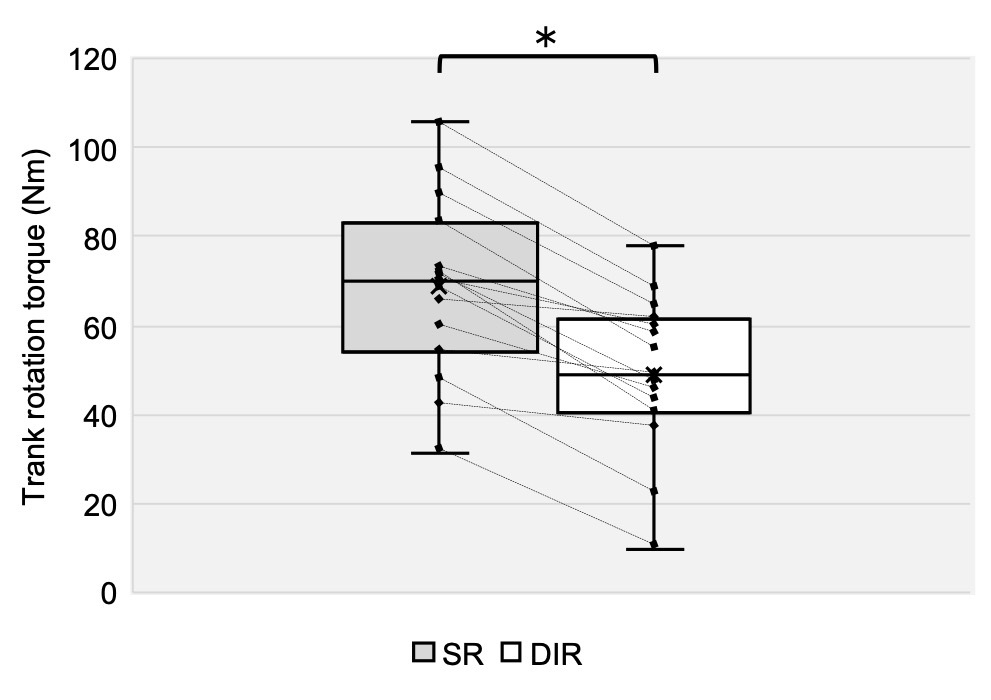
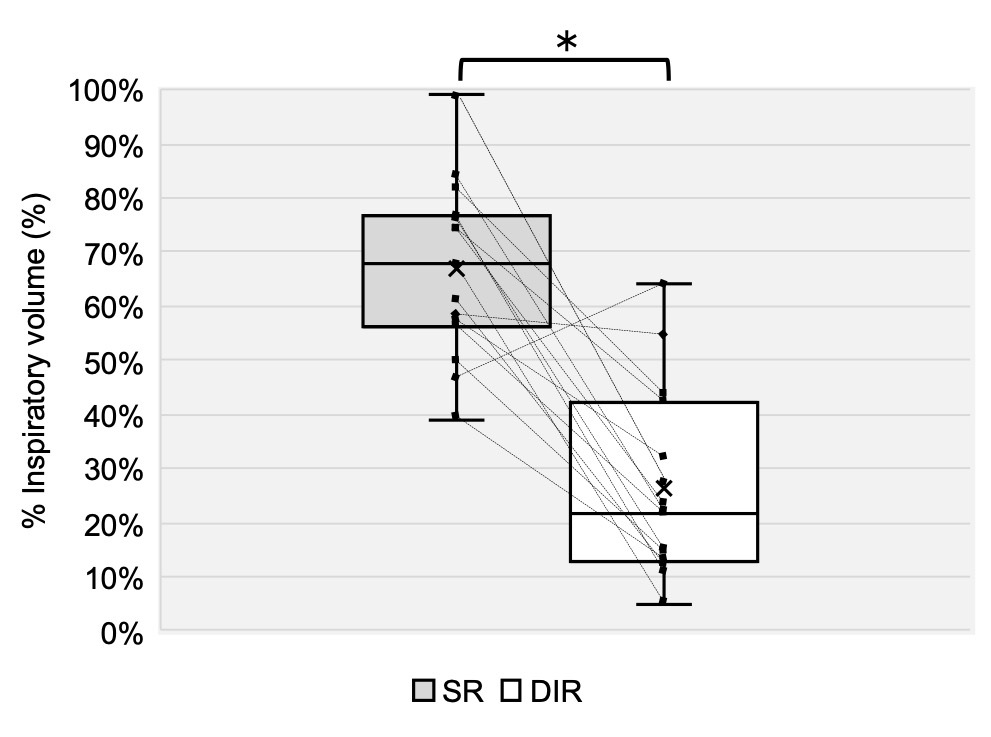
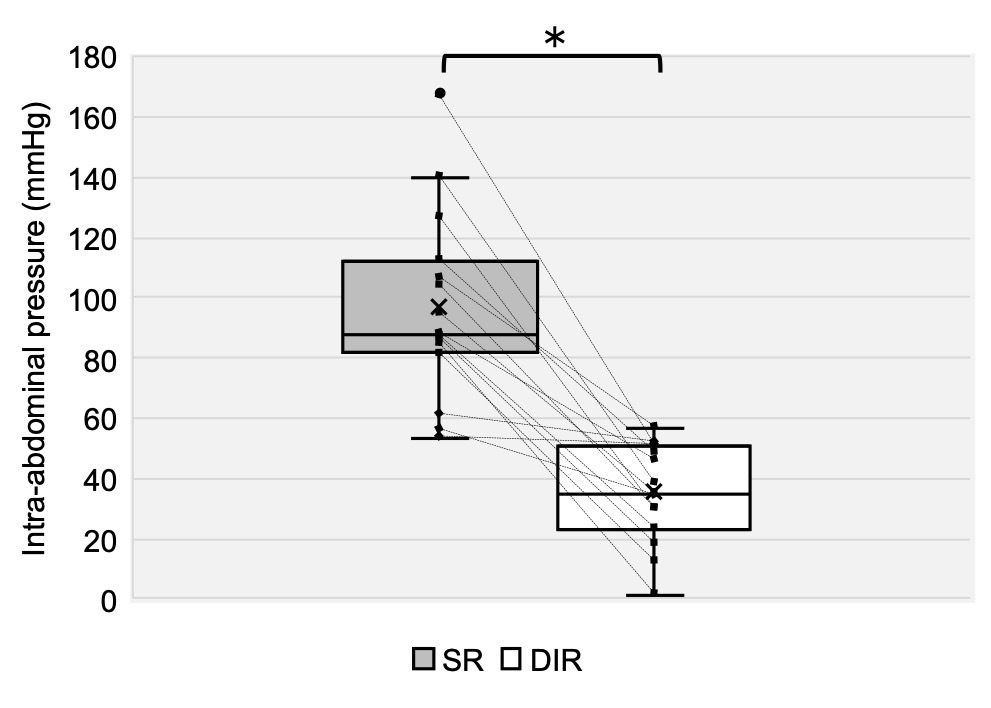
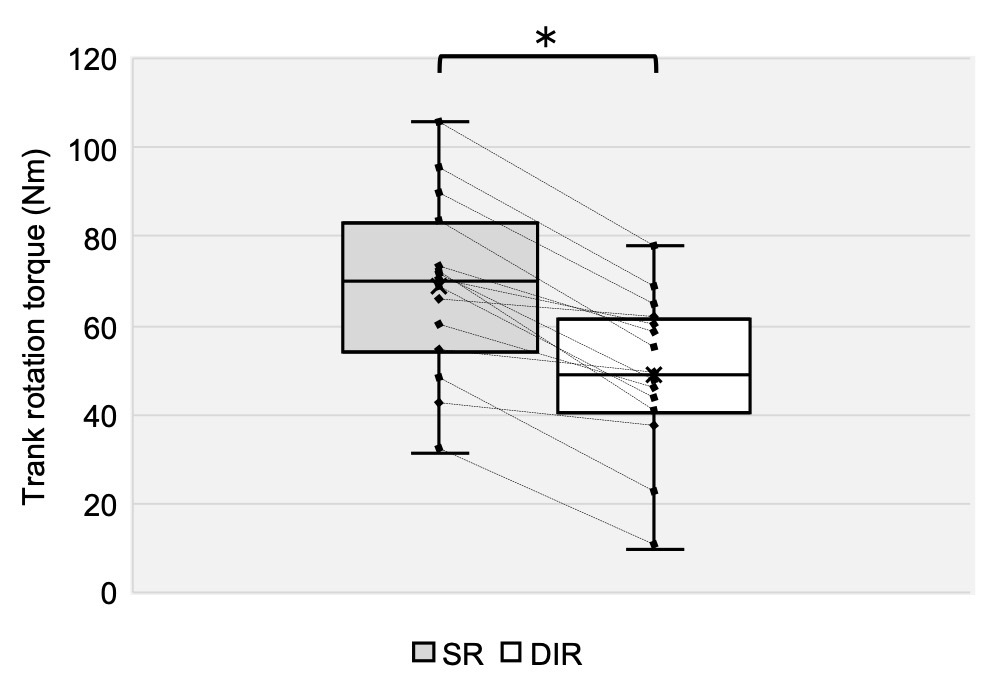
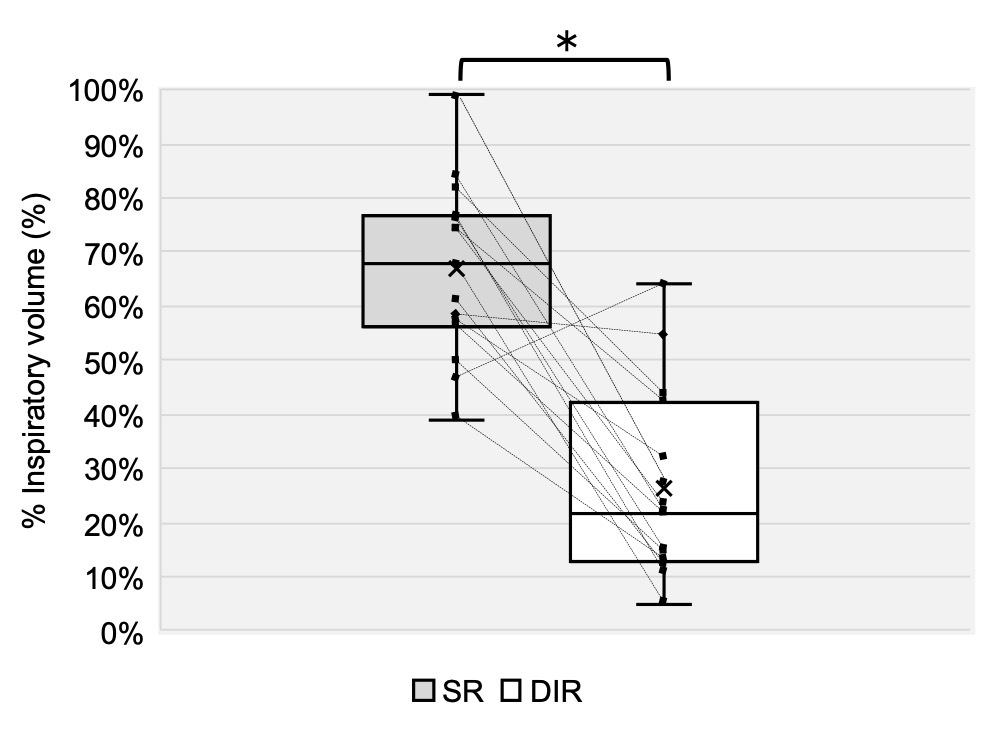
Fifteen healthy, non-athlete young adult males participated in this study (age: 22.3 ± 1.3 years; height: 170.0 ± 5.2 cm; body mass: 63.8 ± 7.9 kg; body fat percentage: 15.6 ± 4.4%). Descriptive statistics for all outcomes are summarized in Table 1. Figures 5–7 illustrate individual and group-level differences between conditions.
IAP was significantly greater in the SR condition than in the DIR condition, with a large effect size (p < 0.01, d = 2.48; Table 1, Figure 5). Torque was also significantly greater in the SR condition than in the DIR condition, with a large effect size (p < 0.01, d = 1.03; Table 1, Figure 6). Similarly, %inspiratory volume was significantly greater in the SR condition than in the DIR condition, with a large effect size (p < 0.01, d = 2.41; Table 1, Figure 7). Finally, %waist was significantly greater in the SR condition than in the DIR condition (p < 0.01, r = -0.88; Table 1).
DISCUSSION
The purpose of the present study was to clarify the effects of the ADIM on IAP and trunk rotational torque during trunk rotation. The ADIM has been widely investigated not only as an intervention for low back pain but also as a breathing strategy, including in relation to its effects on IAP and its application across different phases of motor tasks. However, the effects of performing motor tasks concurrently with the ADIM, particularly during high-load tasks involving horizontal-plane demands, remain insufficiently understood. To the authors’ knowledge, this study is the first to report outcomes obtained during a task combining trunk rotational torque exertion with the ADIM. The primary finding of the present study was that, when trunk rotation was performed under the ADIM condition, IAP, trunk rotational torque, and inspiratory volume were all significantly lower than under the SR condition.
These findings suggest that the observed reductions in IAP and trunk rotational torque under the ADIM condition should be interpreted in the context of concurrent changes in breathing-related variables, rather than as effects of IAP alone. The difference between the ADIM and SR conditions was characterized primarily by the breathing strategy adopted during trunk rotation. Under the ADIM condition, trunk rotation was performed with reduced inspiratory volume and an inwardly displaced abdominal wall, whereas the SR condition allowed a more spontaneous breathing pattern. Correspondingly, both IAP and trunk rotational torque were simultaneously lower in the ADIM condition, indicating that changes in mechanical output occurred alongside alterations in breathing-related variables. These findings provide a basis for discussing potential mechanisms linking breathing strategy and trunk rotational performance.
Previous studies have suggested that increases in IAP are influenced by multiple factors, including inspiratory volume and the activity or strength of the abdominal musculature. Hackett and Chow28 proposed that both respiratory-related factors and abdominal muscle function contribute to the regulation of IAP during exertional tasks. In particular, with respect to inspiratory volume, Kawabata et al.23 demonstrated that, during high-intensity lifting tasks, increases in IAP depend not only on increased inspiratory volume but also on the prevention of excessive expiration. These findings are consistent with the present results, in which the ADIM condition was characterized by a reduction in inspiratory volume accompanied by lower IAP. Taken together, the observed differences between breathing strategies in the present study can be interpreted within the context of previously reported interactions between breathing-related variables and IAP during high-load motor tasks.
While the present data do not allow direct assessment of muscular mechanisms, the observed differences between conditions may be explained by changes in abdominal configuration associated with breathing strategy. Under the SR condition, sufficient inspiratory volume and maintenance of abdominal circumference may have facilitated force generation by the muscles surrounding the abdominal cavity, thereby enabling greater increases in IAP. In contrast, under the ADIM condition, reduced inspiratory volume and intentional inward displacement of the abdominal wall may have limited the ability of these muscles to generate tension, resulting in smaller increases in IAP. A similar mechanism may account for the observed differences in trunk rotational torque, given that increases in IAP have been suggested to contribute to trunk rotational force generation through maintenance of the abdominal wall “hoop” structure.29 Disruption of this hoop configuration may alter muscle length–tension conditions30 within the abdominal wall and impair effective torque generation. Consistent with this interpretation, one recent study18 demonstrated positive temporal and peak correlations between IAP and trunk rotational torque during isometric trunk rotation tasks. Taken together, these findings suggest that breathing strategy may influence trunk rotational performance through concurrent changes in abdominal configuration and IAP; however, these proposed mechanisms remain speculative and should be directly examined in future studies.
Taken together with previous findings, the present results suggest that breathing strategies and respiratory exercise interventions should be selected according to task demands, intended outcomes, and the required level of trunk stability. In particular, the indications for the use of the ADIM warrant careful consideration. While the ADIM has been shown to provide benefits in certain contexts, such as reducing knee adduction moments during walking and increasing hip muscle activity,31 spinal stability and force production during higher-load tasks may be more effectively achieved using alternative strategies. Previous studies have demonstrated that abdominal bracing can enhance spinal stability and reduce unwanted trunk or pelvic motion more effectively than the ADIM,16,32,33 emphasizing the importance of coordinated activation of the trunk musculature rather than selective activation of a single muscle. Stokes et al.34 further emphasized that coordinated activation of the entire trunk musculature is necessary for adequate IAP generation, highlighting the limitations of selective muscle activation. These findings are consistent with the finding in the current study that trunk rotational torque was significantly greater under the SR condition than under the ADIM condition. Accordingly, although the ADIM has value—particularly as a motor control retraining technique for addressing movement dysfunctions35—it may not represent an optimal breathing strategy in all situations. For tasks requiring high levels of trunk stability or rotational torque, breathing strategies that allow greater IAP generation, such as bracing or the Valsalva maneuver, may be more appropriate. Therefore, breathing strategies should be selected and instructed with consideration of individual characteristics, task intensity, and specific performance goals.
Several limitations of this study should be acknowledged. First, breathing strategies during force exertion were not strictly controlled, and spontaneous straining or Valsalva-like behavior may have influenced IAP responses. Although most participants exhibited greater IAP and trunk rotational torque under the SR condition than under the ADIM condition, one participant showed a different trend in inspiratory volume. This finding suggests that individual variability may exist in inspiratory volume responses to ADIM cueing. Second, the underlying muscular mechanisms could not be directly evaluated because electromyographic activity and muscle fiber length were not measured. Abdominal circumference was used as a surrogate indicator to infer abdominal wall configuration; however, this measure may be influenced by subcutaneous adipose tissue and therefore may not fully reflect actual muscular behavior. Third, the experimental task consisted of seated isometric trunk rotation, representing a specific and constrained context that differs from dynamic or sport-specific movements. Therefore, caution is warranted when extrapolating these findings to clinical practice or athletic performance settings. Finally, this study included only healthy young adult males, which limits generalizability of the findings. Future studies should include more diverse populations with respect to age, sex, ethnicity, and training background.
CONCLUSION
This study examined the effects of performing the ADIM on IAP, trunk rotational torque, and inspiratory volume during trunk rotation. The results demonstrated that performing trunk rotation under the ADIM condition was associated with lower IAP, trunk rotational torque, and inspiratory volume than under the SR condition. These findings suggest that changes in breathing strategy, accompanied by reductions in inspiratory volume and IAP, may influence trunk rotational torque during rotational tasks. Therefore, while the ADIM should not be disregarded—particularly as a motor pattern retraining technique—it may not be optimal in all situations. In tasks requiring high levels of trunk rotational torque or stability, alternative breathing strategies that allow greater IAP generation may be more appropriate, depending on task demands and individual characteristics.
Corresponding author
Asuka Kimura
Tokodachi 101, Kaizucho, Toyota, Aichi, 〒470-0393, Japan
Email address: asuka20000317@gmail.com
Phone number: +81 80-2645-2501
Funding
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI, Grant Number 24K14546.
Conflicts of Interest
The authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
We would like to express our sincere gratitude to all participants who contributed to this study.