Introduction
Anatomy of the Radiocarpal Joint
The distal radioulnar joint (DRUJ) is a uniaxial pivot joint with only one degree of freedom.1 This joint connects the distal ends of the radius and ulna and is essential for rotation of the forearm. DRUJ movements are also important for functional activities such as twisting, gripping, carrying, and weight bearing of the upper extremities. One of the important stabilizers of the DRUJ is the triangular fibrocartilage complex (TFCC). The TFCC is named for its triangular shape. The TFCC is a complex structure that provides intrinsic stability to the DRUJ. The TFCC is composed of multiple structures, including both superficial and deep portions of the dorsal and volar radioulnar ligaments, the fibrous disk and ulno-meniscus homologue, the sub-sheath of the extensor carpi ulnaris, the wrist ulnar collateral ligament, and the ulnocarpal ligaments of the volar wrist that include the ulnolunate and ulnotriqeutral ligaments. Due to its anatomical complexity, this portion of the wrist has historically been called the “black box” of the wrist.2 Clinicians’ understanding of the complex anatomy of this area has improved greatly due to anatomical, cadaveric, and biomechanical studies.3–7 The TFCC has 3 main functions: 1) stabilize the DRUJ, 2) stabilize the ulnocarpal space, and 3) act as a shock absorber to transmit ground reaction forces or loads through the ulnar side of the wrist.8,9
Injuries to the ulnar side of the wrist are generally overuse or traumatic, such as a fall on an outstretched hand (FOOSH). Patients will report pain on the ulnar side of the wrist, predominantly during twisting or during movements into radial or ulnar deviation. Patients will present with popping or clicking sensations, weakness, limited range of motion, swelling, and instability, characterized by the sensation that the wrist is “giving out” or “slipping”. These symptoms will make most wrist activities difficult, especially those with rotation, such as opening door knobs, cooking, and/or using a screwdriver.
The Role of MSK Ultrasound in TFCC Injury
Advantages
-
Non-Invasive: Point of care ultrasound is a non-invasive imaging technique that can be used for the examination of the soft tissue and ligaments DRUJ and TFCC in the distal ulnar side wrist.
-
Real-Time Imaging: MSKUS enables evaluation of structures, such as the DRUJ and TFCC, as well as associated ligaments.
-
High-Resolution Visualization: MSKUS provides detailed images of the DRUJ, TFCC, and ligaments.
-
Accessibility and Cost-Effectiveness: MSKUS is portable, widely available, and less expensive than magnetic resonance imaging (MRI).
Limitations
-
Operator Dependency: MSKUS requires skill and experience for accurate interpretation of findings. The ability to sonograph the distal ulnar side of the wrist is to a large extent influenced by the operator and the availability and technical considerations of state-of-the-art equipment.
-
Depth Limitations: Visualization is usually not a problem for the superficial wrist structures.
-
Artifacts and Shadows: Bone and calcifications may create image artifacts, requiring adjustments to transducer positioning and frequency.
Sonographic Technique for Evaluating the TFCC
Equipment Setup:
-
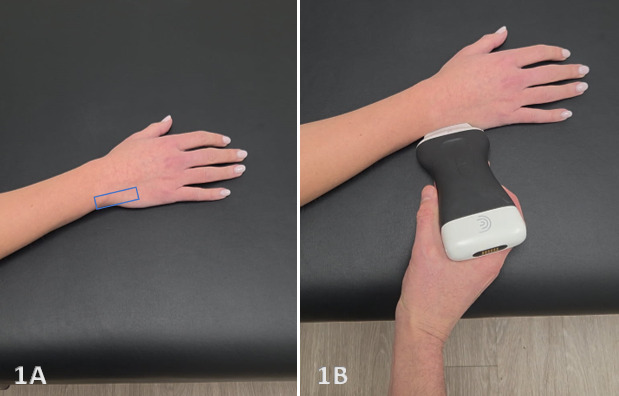
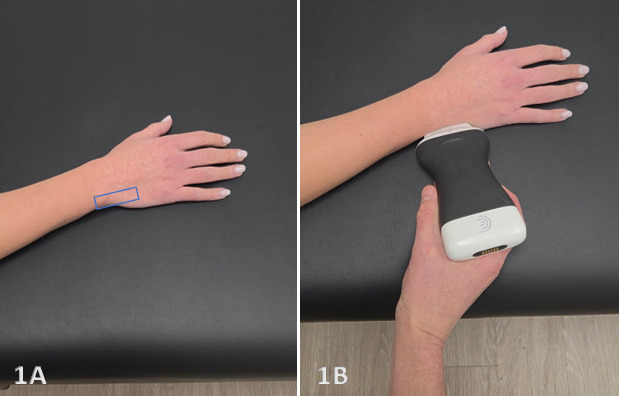
Transducer Type: Because of the superficial nature of the wrist structures, a standard high-frequency, linear array transducer is normally used. In some instances, an L-shaped, hockey-stick-type transducer may be required.
-
Patient Position: the patient typically sits with the volar forearm on the surface with the dorsal wrist facing superior. The dorsal surface is normally viewed as the structures are more superficial and easier to visualize. The transducer will be placed in the long axis (LAX) and short axis (SAX) to view the TFCC.
-
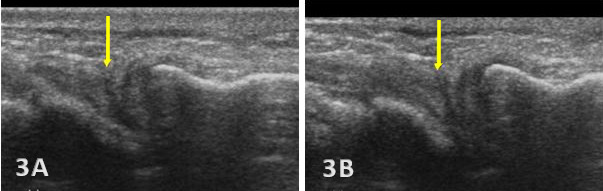
Dynamic Assessment: Dynamic views can be obtained by having the patient supinate or pronate the wrist, or flex or extend the wrist while visualizing the ulnar-sided structures.
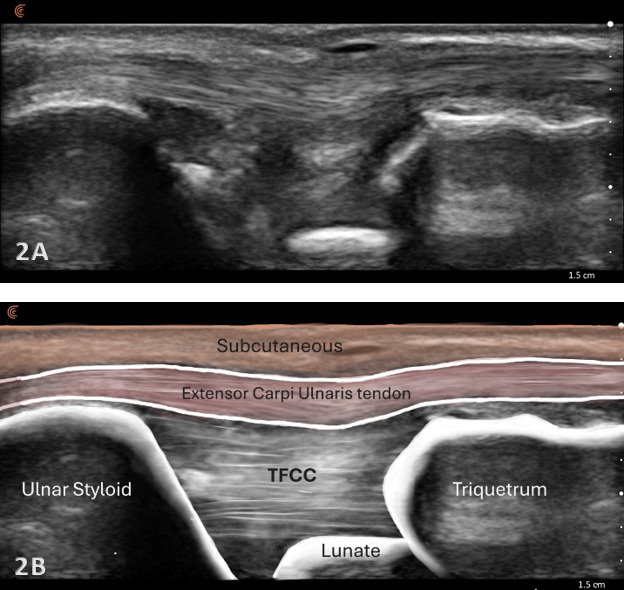
Normal Sonographic Appearance
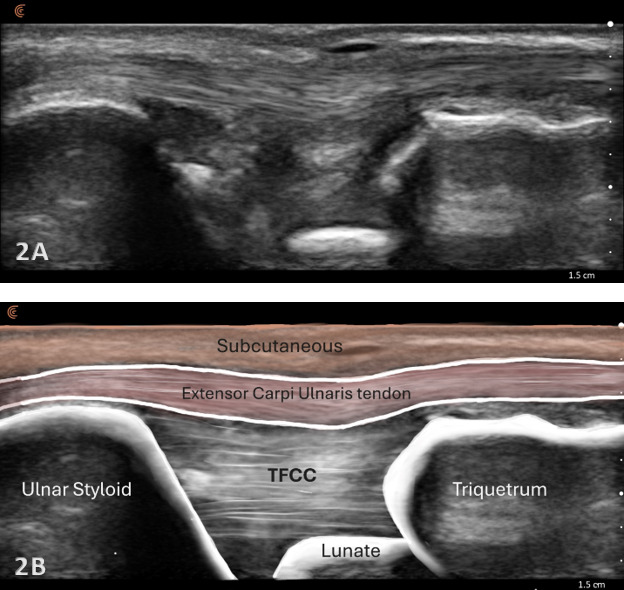
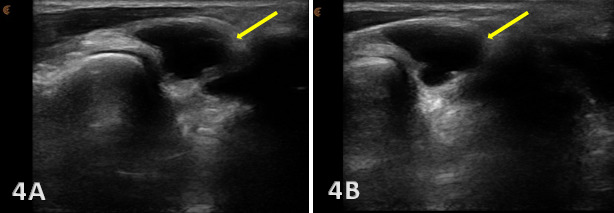
Normal TFCC appears as a thin, continuous, triangular band of homogeneous echogenicity extending from the distal ulna toward the ulnar carpal bones. The margins are smooth and well defined, without fiber disruption or adjacent fluid collection. No abnormal gapping is observed at the ulnocarpal interface, and the surrounding joint recess remains collapsed in the absence of effusion.
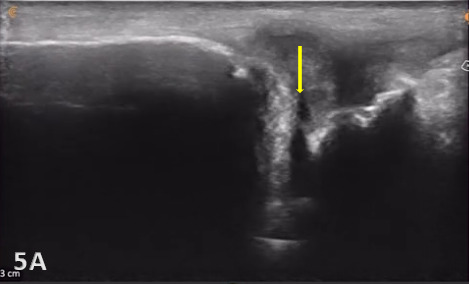
Pathologic Findings in Injured TFCC
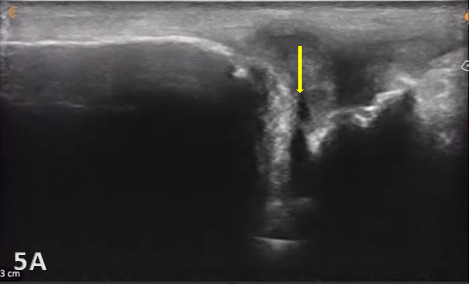
Direct ultrasound findings of TFCC injury include:
-
Hypoechoic or anechoic cleft seen within the normal fibrillar pattern of a normal TFCC.
-
Irregular or disrupted margins of the articular disk.
-
Thinning or fissuring of the TFCC indicates a partial-thickness tear.
-
Abnormal thickness of the TFCC, such as thinning (degeneration) or thickening (edema or chronic overuse), may be seen as pathology.
-
A complete disruption of the continuity of fibers of ligaments or the disk with fluid extending into the joint would indicate a complete full-thickness tear of the TFCC.
-
Associated joint effusion and/or synovitis (synovial hypertrophy) and cysts. Joint effusion will appear as anechoic or hypoechoic fluid within the DRUJ or TFCC area. Joint effusion is somewhat compressible and mobile when transducer pressure is applied to the area. This is different from synovitis, which appears as hypoechoic or isoechoic, non-compressible tissue within the joint recess. Lastly, a ganglion cyst will appear as a well-defined, round or lobulated cystic structure with anechoic or hypoechoic internal contents. The cyst typically has a small, smooth wall and exhibits posterior acoustic enhancement. These cysts will typically be minimally or non-compressible and painful.
Indirect ultrasound findings of TFCC injury include:
-
Anechoic or hypoechoic fluid indicating effusion in the joint.
-
Excessive translation of the ulna relative to the radius during dynamic visualization of the movements of pronation and supination may indicate DRUJ instability.
-
A bony avulsion of the ulnar styloid attachment site would be indicative of an associated peripheral TFCC tear.
Clinical Implications for Rehabilitation Providers
MSK ultrasound provides real-time feedback to rehabilitation professionals, facilitating early diagnosis of TFCC injuries and interventions. Key applications include:
-
Early Detection of Injury / Accurate Injury Grading: MSKUS can detect small anechoic or hypoechoic fluid collections in the ulnocarpal space, indicating injury and effusion in the joint or soft tissues. Identifying this early will help guide treatment planning. Additionally, small ligament sprains or partial tears may be seen on ultrasound as irregular loss of normal fibrillar patterns.
-
Dynamic Functional Testing: MSKUS can be used to dynamically stress the tissues with gentle wrist motion of supination/pronation, ulnar/radial deviation, and wrist flexion and extension to reveal signs of excessive movement or instability at the DRUJ, soft tissue impingement between bones, or abnormal findings such as cysts.
-
Guided Interventions: Ultrasound imaging assists with dry needling or precision-guided injections, such as corticosteroid injections for inflammation.
- Patient Education: Real-time imaging serves as a visual aid to explain the nature of the injury and set realistic expectations for recovery.
Limitations and Challenges
As with any use of MSKUS, image interpretation and quality are operator dependent and rely heavily on experience and skill. The peripheral soft tissues are easier to see than the central portion of the disk, which is deeper and thinner, making visualization more difficult. The TFCC is a complex multicomponent structure of bones, ligaments, and soft tissues, which makes distinguishing its components difficult for the novice. Anisotropy of ligaments and disk from poor transducer placement can make TFCC fibers or ligaments appear hypoechoic or torn. Lastly, because the TFCC is housed in a relatively small area, the field of view is limited.
Conclusion
MSKUS is a valuable, dynamic, and cost-effective imaging modality for evaluating the TFCC. It provides high-resolution, real-time visualization of bones, cartilage, and soft tissues and can be used in both acute and chronic settings. Ultrasound allows dynamic visualization of the ulnar side of the wrist. Incorporating MSKUS into the physical therapist’s clinical practice for distal wrist examination enhances diagnostic accuracy, supports timely management decisions, and ultimately improves patient outcomes in cases of suspected TFCC injury.