
INTRODUCTION
Multiligamentous knee injuries occur when there is an insult to two or more of the main ligamentous structures of the knee.1,2 The main ligaments of the knee include the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), fibular or lateral collateral ligament (LCL), and medial collateral ligament (MCL).1,2 Multiligamentous knee injuries are rare. The mechanism of injury varies ranging from an ultra-low energy fall, to a high energy traumatic mechanism seen in sports.3 This case aligns with the Knee Ligament Sprain Clinical Practice Guideline (CPG) diagnostic classification of knee stability and movement coordination impairments, which was used to describe the patient’s impairments and functional limitations.4
Infection following knee ligament reconstruction is rare, estimated to occur 0.14 -0.18% of cases,5–7 however, septic arthritis is a potentially devastating complication that can lead to graft failure, instability, chondral degradation, pain, arthrofibrotic changes, and the potential need for additional surgery.8,9 Many investigators have reported suboptimal functional outcomes when managing patient with post-operative infections.8,10,11 One of the most common causes of nosocomial infections, is due to Staphylococcus epidermidis. This is a gram-positive cocci, nonmotile, non-spore forming bacteria and is frequently associated with clinical infections in prosthetic joints and surgical sites.12 Staphylococcus epidermidis is part of normal human skin flora and is typically benign, but it can enter the bloodstream and become pathogenic.13 When introduced into the host it develops a biofilm for protection and accumulates, which protects it against host defense and can lead to sepsis.13
This case report describes the rehabilitation management and outcomes following multiligament knee reconstruction complicated by septic arthritis that developed during the early postoperative period and shortly after an elective cosmetic procedure.
CASE DESCRIPTION
A 22-year-old female recreational athlete (1.753 m, 73 kg, BMI = 22.4) was involved in a motorcycle accident resulting in polytrauma to her pelvis and multi-structural damage and dislocation of her right knee. Prior to her injury, the subject was physically active in recreational athletics involving running and gymnastics, therefore had high functional expectations for return to sport and activity after injury as she wished to return to her prior level of function. Past medical history included anxiety, depression and ADHD without a significant medical or family history of immunologic or autoimmune conditions. Psychosocial factors were screened using the Optimal Screening for Prediction of Referral and Outcome Yellow Flag (OSPRO-YF) and improved over the course of rehabilitation. No relevant genetic conditions were reported.
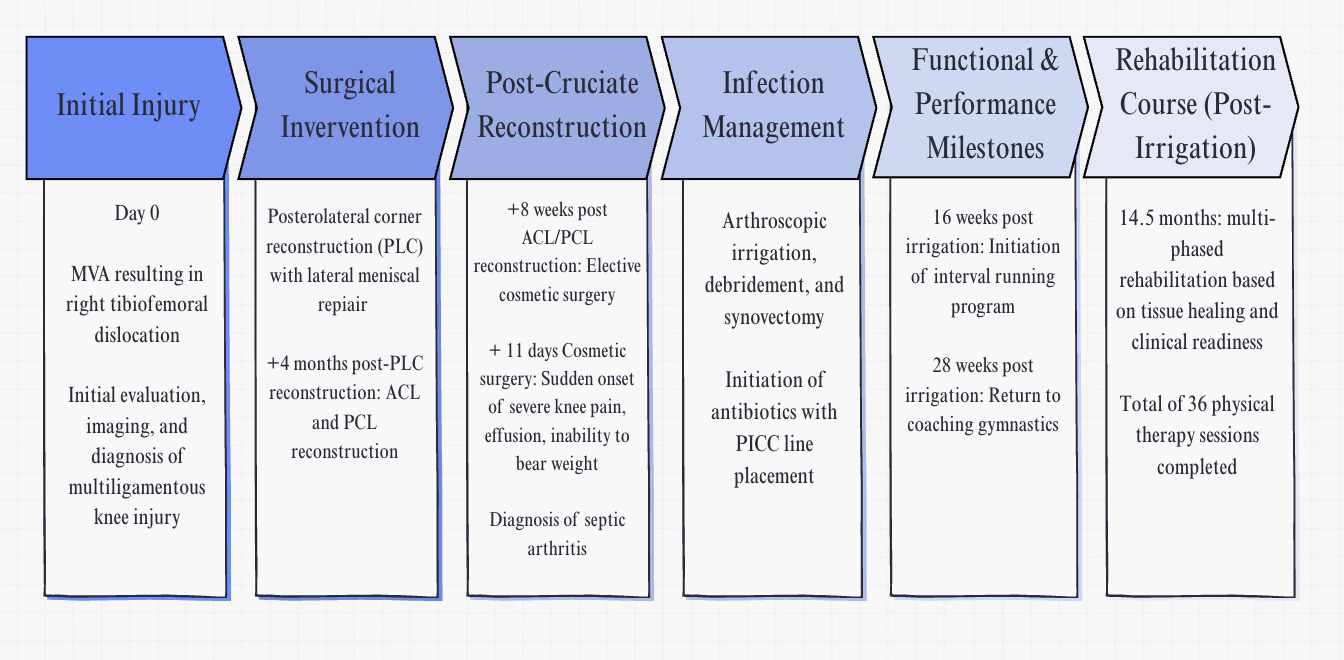
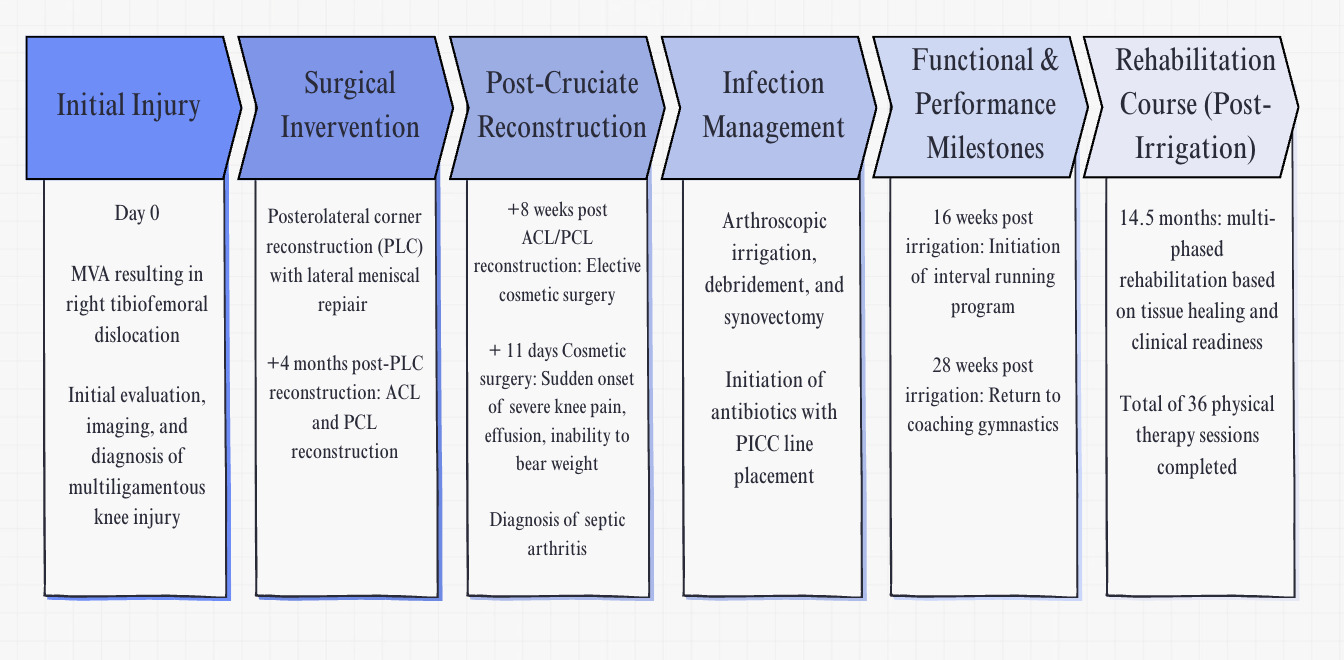
After the accident, MRI results revealed a complete disruption of the ACL, PCL, LCL, anterolateral ligament, popliteus tendon, and iliotibial band. Other findings included an avulsion fracture of the medial femoral condyle and a peripheral lateral meniscus tear. The subject underwent posterior lateral corner (PLC) reconstruction and lateral meniscus repair surgery eight days after the accident. She completed approximately four months of physical therapy before undergoing her second staged procedure where she underwent an ACL reconstruction with hamstring autograft and PCL reconstruction with allograft with both grafts being reinforced with suture augmentation. The subject completed two months of postoperative physical therapy before presenting with acute knee swelling, pain, and inability to bear weight. Knee aspiration and laboratory findings were consistent with septic arthritis, and she underwent emergent irrigation and debridement. This occurred six months after posterolateral corner (PLC) reconstruction with lateral meniscal repair and eight weeks after the ACL/PCL reconstruction. One week prior to symptom onset, she underwent elective cosmetic surgery with fat autograft harvested from the contralateral thigh. She was admitted to the hospital for five days and treated with knee arthroscopy including irrigation, debridement, and synovectomy, followed by peripherally inserted central catheter (PICC) placement for intravenous antibiotic therapy (Figure 1). This case report describes the management of a multiligament knee reconstruction complicated by septic arthritis following elective surgery performed shortly after orthopedic reconstruction.
Outcome Measures
The subject was examined at various time points during the rehabilitation process due to the complexity of her pathology. Five months after the ACL/PCL reconstruction, and three months after the surgical irrigation and debridement, the subject was evaluated with patient-reported outcome measures and performance measures, and then re-examined at eight months, 11 months, and 13 months post-cruciate ligament reconstruction until the final physical therapy visit (Table 1).
Patient Reported Outcomes
To assess symptoms, function, and sports activity, the International Knee Documentation Committee (IKDC) Subjective Knee Form was utilized. This questionnaire is both reliable and valid for patients with various knee issues.14–17 The IKDC consists of 18 questions, which include seven items related to symptoms, one item regarding sports participation, nine items focused on daily activities, and one item addressing current knee function. The scoring ranges from 0 to 100, where a score of 100 indicates no limitations in daily or sporting activities and no symptoms present.16 Irrgang et al. determined that the normal IKDC score for individuals who have undergone ACL reconstruction is 95.2, a nearly normal score is 91.2, while an abnormal score is 84.9, and a severely abnormal score is 75.4.14 Additionally, based on test-retest reliability, the Minimal Clinically Important Difference (MCID) is 9.5 points.18
Although originally developed for ACL injury, the ACL-RSI is a reliable and validated measure of psychological readiness to return to sport and was included in this case because surgical complexity, prolonged rehabilitation, and postoperative complications may reduce confidence with higher-level activity and return to running and gymnastics.19 This scale measures three critical domains: emotions, confidence, and risk appraisal. Scores from these domains are combined and averaged to produce a total score ranging from 0 to 100, with higher scores indicating a stronger psychological readiness.19 In this case, the shortened version of the scale, which includes six core items, was employed. A cutoff score of 60 on this short version, assessed at six months post-op, possesses high specificity and moderate sensitivity for predicting whether an athlete will return to their pre-injury level of sport within 12 months after ACL reconstruction.20 Furthermore, Webster et al. established that the minimally important change (MIC) for the short form is 15.1 points, highlighting its significance in monitoring recovery progress.19 However this may require further investigation, as the scores for the short form were derived from the full version, therefore responses may differ when given this shortened version independently.19
The Optimal Screening for Prediction of Referral and Outcome Yellow Flag (OSPRO-YF) tool is designed to assess negative mood, fear avoidance, and positive coping in individuals with musculoskeletal pain.21 It is a reliable and valid psychological assessment that evaluates three main domains including: self-efficacy and acceptance, negative pain, and negative mood.21 Of the three domains, the OSPRO-YF generates scores for 11 psychological distress constructs based on subjects’ responses. Scores that exceed the 75th percentile in negative pain coping or negative mood constructs or fall below the 25th percentile in self-efficacy and acceptance, indicate a “yellow flag” in those areas.22 The summary score of the OSPRO-YF counts the number of yellow flags identified. A greater number of yellow flags signifies elevated pain associated distress, providing insights into the subjects’ treatment response and need for psychologically informed intervention.22
Psychological factors, including elevated fear and reduced readiness, influenced pacing and communication throughout parts of the rehabilitation process. Early in the rehab process, the subject presented with questions at the beginning of each session, and time was intentionally dedicated to addressing concerns and providing reassurance. Throughout rehabilitation, education was emphasized regarding anatomy and postoperative healing timeframes, while later phases focused on performance testing and graded exposure to progressively demanding tasks to support confidence and psychological readiness alongside physical recovery.
Performance Measures
A battery of tests were used to objectively test muscular strength and performance to help assess physical readiness for returning to running. Performance testing included objective strength and balance testing. Isokinetic strength testing was measured at 60 deg/sec with an isokinetic dynamometer (Biodex System 3; Biodex Medical Systems Inc, Shirley, New York). Peak torque to body weight and a comparison to the uninvolved limb was recorded and analyzed. In previous literature, it has been suggested that subjects’ quad strength exceeding a magnitude greater than >60% of the uninvolved side is required to initiate jogging.23,24 In addition, the Y-Balance test was used to gauge the subject’s readiness for running, given prior research suggesting a correlation between functional performance and muscle strength.25 Although hop testing is recommended by the Knee Ligament Sprain CPG, it was not performed due inconsistent attendance during later rehabilitation phases, which limited a safe progression in rehab.
EXAMINATION
One week status post cosmetic surgery, the subject reported rapidly increasing pain and swelling, loss of range of motion, and an inability to bear weight through the knee without an acute injury. The subject utilized standard axillary crutches and was weightbearing as tolerated with an immobilizer locked in extension. She reported knee stiffness and pain at rest with significantly diminished functional capacity. During the initial examination, post-operative dressings were removed, and new dressings were applied to the incision sites. The subject displayed a large knee effusion, as noted with sweep testing. Her post-operative pain during the evaluation was rated a 10/10 and was described as sharp and stabbing along the incisions with symptom exacerbation with motion of the knee joint and/or volitional contraction of the surrounding musculature. Due to high levels of resting pain during the early postoperative phase and insufficient quadriceps control, functional testing (e.g., step-down assessment or squatting) was deferred. The subject demonstrated movement coordination impairments with noted impairment in neuromuscular control, reduced single-limb stability, and reliance on compensatory strategies during gait and transfers. Objective measures are presented in Table 2. Subject’s goals were to return to running and recreational gymnastics.
CLINICAL IMPRESSION
Consistent with the Knee Ligament Sprain CPG, the subject presented with knee stability and movement coordination impairments following surgery, including strength deficits, decreased knee ROM, pain, effusion, and gait deviations. The subject attended physical therapy twice weekly and was prescribed a home exercise program to be performed 3-5x/day, seven days per week, to restore full ROM and improve quadriceps neuromuscular control. Of note, a change in insurance coverage resulted in fewer authorized physical therapy visits, which temporarily limited rehabilitation frequency.
INTERVENTIONS
Rehabilitation following a knee arthroscopic irrigation focuses on restoring joint function, managing inflammation and gradually returning to activity. Rehabilitation followed a 3-phase, criteria-based progression: (1) acute phase, (2) progressive strengthening and power, and (3) plyometrics and return-to-running phase. The interventions utilized in this case were guided by the knee ligament sprain CPG for knee instability and movement coordination impairments and were selected to align with the biomechanical roles of the reconstructed ligaments. The subject in this case underwent arthroscopic irrigation approximately six months after the primary PLC reconstruction with lateral meniscus repair, and eight weeks following an ACL and PCL reconstruction. The protocol emphasized restoring strength and resolving residual ROM impairments between weeks 8–12 in preparation for plyometrics. In cases of septic arthritis, early and structured rehab is crucial due to risks of stiffness, arthritic changes and poor functional outcomes.26,27
Phase I: Acute Phase (0–6 weeks post-irrigation)
In the early post-operative phase, the knee ligament sprain for movement coordination deficits from the CPG model suggests cryotherapy, early weight-bearing, and continuous passive motion.4,28 Knee extension was prioritized, given its correlation with long-term joint health.29 Quadriceps strengthening and neuromuscular control exercises progressed as tolerated.30 Rehab was adapted based on PICC line placement and fluctuating lab values, occasionally requiring temporary pauses in activity during antibiotic treatment due to extremely low white blood cell count during which exercise was contraindicated.
Phase II: Strengthening/Power Phase (6–12 weeks post-irrigation)
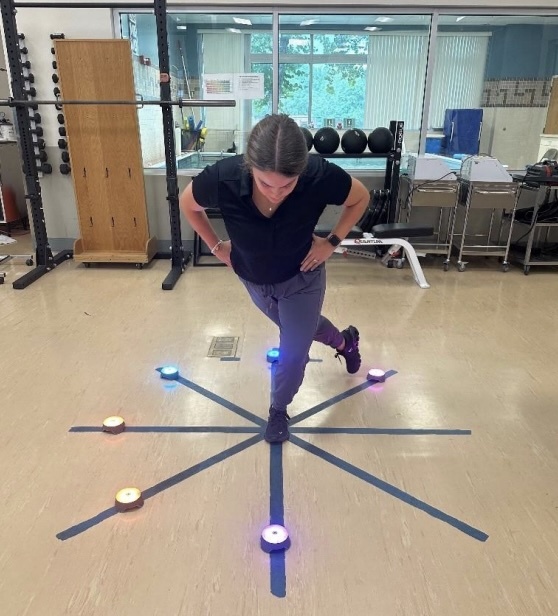
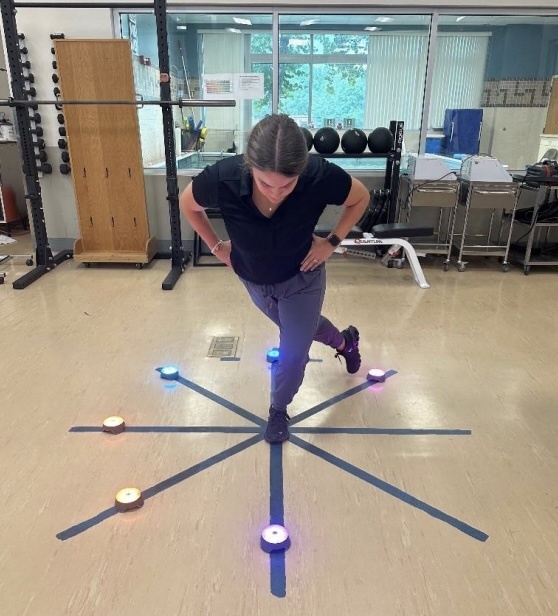
As ROM and quad function normalized, open and closed kinetic chain strengthening focused on hypertrophy, endurance, and neuromuscular control.31–33 PICC line removal and lab value stabilization allowed increased load and functional exercise progression. Isolated hamstring strengthening was avoided during this phase, as the surgical protocol restricted isolated hamstring loading for six months following PCL reconstruction due to the potential for increased posterior tibial translation with higher knee flexion angles.34 In this phase, co-contraction exercises of the quadriceps and hamstrings were emphasized in this phase with progressions as tolerated such as calf raises, mini squats, step ups, leg press, and reactive star excursion (Figure 2). At 12 weeks status post PCL reconstruction, posterior chain exercises were progressed in volume and intensity, with addition of closed kinetic chain (CKC) exercises from 0°–30° of knee flexion as the hamstring cannot produce a posterior shear force that will impair the PCL graft at these angles.34
Phase III: Plyometrics/ Return to Running Phase (12+ weeks post-irrigation)
In this phase, focus shifted to plyometrics, strength and ROM normalization, and running readiness. Objective testing tracked ROM, balance, strength, and perceived function (Table 3). Criteria for initiating running included full ROM, >90% limb symmetry index (LSI) Y-Balance scores, >60% quadriceps peak torque-to-bodyweight ratio, and subjective readiness (Table 3, Figure 3). The subject met all criteria 12 weeks post-infection and began a progressive return-to-jog program.

OUTCOMES
The subject completed 36 sessions over 63 weeks from arthroscopic irrigation to final visit of physical therapy. The IKDC score increased by 17.24 points (MCID = 9.5), and ACL-RSI improved by 30 points (MIC = 15.1).15,19 Subjects with postoperative septic arthritis following ACL reconstruction have been reported to demonstrate lower IKDC scores (mean 58.9) compared with uncomplicated ACL reconstruction outcomes; therefore, an IKDC score of 55.17 in this case may be consistent with expected patient-reported outcomes following this complication.26 The OSPRO-YF decreased from five yellow flags (Fear-Avoidance Beliefs Questionnaire – Physical Activity Subscale, Tampa Scale of Kinesiophobia –11 item version, Pain Anxiety Symptoms Scale – 20 item, Pain Self-Efficacy Questionnaire, Chronic Pain Acceptance Questionnaire) to 3 (Pain Self-Efficacy Questionnaire, Chronic Pain Acceptance Questionnaire, and Pain Catastrophizing Scale). Isokinetic testing revealed quadriceps peak torque to body weight ratio of 84.2%, with an LSI of 96.6%, surpassing normative values. Isokinetic hamstring strength revealed 55% peak torque to body weight ratio with a quadricep to hamstring ratio of 0.47, reflecting lower hamstring strength compared to the normative value of 0.60.35 She returned to an interval jogging program at 16 weeks and resumed coaching gymnastics at 6.5 months post-irrigation. Risks versus benefits discussions were emphasized throughout the rehab process in accordance with the subject’s high expectations and goals noted at initial evaluation. Given the subject’s injury history and the demands of coaching gymnastics and demonstrating skills, the subject independently elected to resume higher level activities and later reported these attempts to the physical therapist.
DISCUSSION
The purpose of this case study was to describe the unique rehabilitation plan utilized following a multiligamentous knee reconstruction complicated by infection, and to highlight infection as a critical differential diagnosis in individuals with acute joint symptoms, particularly in the setting of recent surgical procedures. The onset of infection after an elective surgery altered the clinical trajectory of this subject, underscoring the importance of early detection, interdisciplinary coordination, and critical thinking related to subsequent subject management.
Early rehabilitation emphasized cryotherapy, early weight-bearing, and controlled range of motion to reduce effusion and restore neuromuscular control while minimizing tibiofemoral shear forces. Given the reconstruction of the PCL and the nature of a multiligamentous knee injury, the role of the PCL in resisting posterior tibial translation was taken into consideration, and early strengthening focused on quadriceps and hamstring co-contraction and hamstring activation in small knee flexion angles (0°–30°), where posterior shear forces on the graft are minimized.34 Isolated hamstring strengthening was delayed until six months postoperatively to allow for appropriate graft protection and progressive tissue loading.36 These biomechanically informed interventions supported safe progressions of knee stability and movement coordination.
Psychosocial factors played an important role in the subject’s recovery and informed clinical decision making throughout rehab. Measures such as the ACL-RSI and the OSPRO-YF tool provided insight into fear of re-injury, confidence with movement, the influence of pain perception, motor control, and adherence to rehabilitation. Elevated fear avoidance and reduced psychological readiness were identified during the early phases of rehab requiring a focus on education and considerations when progressing through the different rehab phases.
CPG elements such as hop testing were intentionally omitted in this case due to many factors. Hop testing and movement coordination assessments were deferred because the subject had not yet achieved the strength, confidence, or psychosocial readiness required for safe and valid performance. Although these measures were planned for later phases of rehabilitation once physical and psychological prerequisites were met, the subject independently returned to coaching gymnastics at 28 weeks post irrigation and subsequently did not return to rehabilitation, precluding further objective testing.
Infection following multiligamentous knee surgery is a rare but devasting occurrence that contributes to complications and diminished functional outcomes post operatively.5–8,10,11 Some reports estimate infection occurs in less than 1% of surgical cases; however, infection has the potential to lead to graft failure, chondral degradation, arthrofibrosis, and other complications possibly warranting additional surgical intervention.8,9 In this case, septic arthritis following multiligament knee reconstruction resulted in a significant setback in functional tolerance, requiring emergent surgical management and temporarily limiting rehabilitation progression. Following irrigation and debridement, treatment emphasis shifted toward restoring knee range of motion and controlling joint irritability, with a gradual and conservative reintroduction of strengthening to avoid symptom exacerbation. As pain and effusion decreased, strengthening progressed to single-limb loading with an emphasis on neuromuscular control and movement quality. Interventions were also individualized to the patient’s perceived deficits and sport-related goals, with focused training on single-leg squatting mechanics to support return to running and recreational gymnastics. Given that postoperative infection is associated with poorer short and long-term outcomes after multiligament knee reconstruction, rehabilitation required a calculated, phase-specific exercise progression while the subject completed infection management and gradually restored functional capacity for return to sport and coaching activities.26,27
Timing of elective surgery following orthopedic surgery is debated. Some evidence suggests that between six and twelve weeks is sufficient to prevent infection in the joint affected by the orthopedic surgery.10 In this case report, the subject presented with clinical symptoms after an elective cosmetic procedure, which she underwent eight weeks after her ACL/PCL ligament reconstruction. The infection occurred in accordance with the recommended timeframe suggested to prevent infection, and resulted in a five-day hospital admission, and treatment including knee arthroscopy with irrigation, debridement and synovectomy and a PICC line placement for antibiotic treatment. In this case, septic arthritis developed 11 days after an elective cosmetic procedure performed eight weeks after ACL/PCL reconstruction. While causation cannot be established, this timeline highlights the importance of shared decision-making regarding the timing of additional elective procedures during early postoperative recovery. This timeline highlights the potential consequences of scheduling elective procedures soon after major orthopedic reconstruction and may help guide shared decision-making regarding surgical timing. Patients who have undergone sequential surgical procedures, may be at an increased risk of delayed infection and post-operative complications that may warrant ongoing monitoring throughout their recovery.
This case report highlights the need for collaborative interdisciplinary care and holistic exercise prescription to address the subject’s deficits to adequately progress toward returning to sport.
This case report describes a single subject, limiting generalizability to broader populations or procedures. Outcomes in other patients may vary due to infection timing, injury severity, graft type, and type of elective surgeries. While clinical assessments and interventions were well documented, long-term patient reported outcomes and strength metrics could not be discerned, limiting conclusions about long term recovery. However, this report raises important considerations regarding the appropriate timing of elective procedures following orthopedic surgery and highlights the importance of structure therapy in return to function following a deviating complication like infection.
CONCLUSION
The results of this case report demonstrate the ability of a female recreational athlete who sustained a multiligamentous knee reconstruction and subsequent infection to return to running and coaching gymnastics. Although return to sport testing criteria were not fully completed and the subject returned to coaching, this case report provides information to help direct physical therapists and orthopedic surgeons alike on considerations regarding timing of elective surgeries after orthopeadic procedures.
Corresponding Author
Maria J. Rademacher
Department of Rehabilitation- Duke Physical Therapy Sports Medicine at the Center for Living 3475 Erwin Rd, Durham, NC 27705
maria.rademacher@duke.edu
Conflict of interest statement
This case report was completed during the University of Florida Health Sports Residency approved by the American Board of Physical Therapy Specialties (ABPTS). The authors report no conflicts of interest.