INTRODUCTION
Glenohumeral (shoulder) dislocations are relatively common in the United States, with over 77,000 occurring each year.1 The vast majority of cases are anterior dislocations (95%).2,3 Bankart lesions are frequently present in these anterior dislocations. For cases with minimal glenoid bone loss, arthroscopic Bankart repair (ABR) remains a widely used procedure for shoulder stabilization.4–6
Despite advancements to the procedure, high failure rates leading to recurrent shoulder instability remain a concern in patients returning to collision sports (e.g., rugby, ice hockey, American football).6–10 Current literature reports widely variable ABR failure rates, ranging from approximately 3 to 55% in athletes.11–13 While ABR stabilizes the shoulder, it can fail to address the underlying bone lesions that can promote further instability and delay return to sport in young, athletic patients. Evidence has shown that failure is often driven by morphology due to bone loss on the glenoid and humeral head.14,15
These insights have drawn attention to managing humeral-sided defects that lead to instability. A Hill-Sachs lesion is a compression defect on the humeral head that forms after it comes into contact with the anterior glenoid rim following a shoulder dislocation.16 To address these types of bony defects, remplissage with ABR may help better stabilize the joint, lowering recurrent instability while maintaining a similar range of motion (ROM) compared with isolated ABR.17 The purpose of this clinical commentary is to provide an evidence-based overview of arthroscopic Bankart repair with remplissage, including technique, biomechanics, clinical outcomes, and indications.
TECHNIQUE
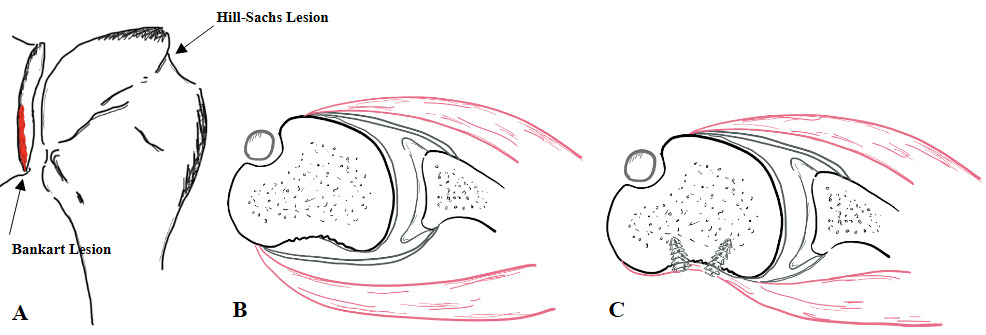
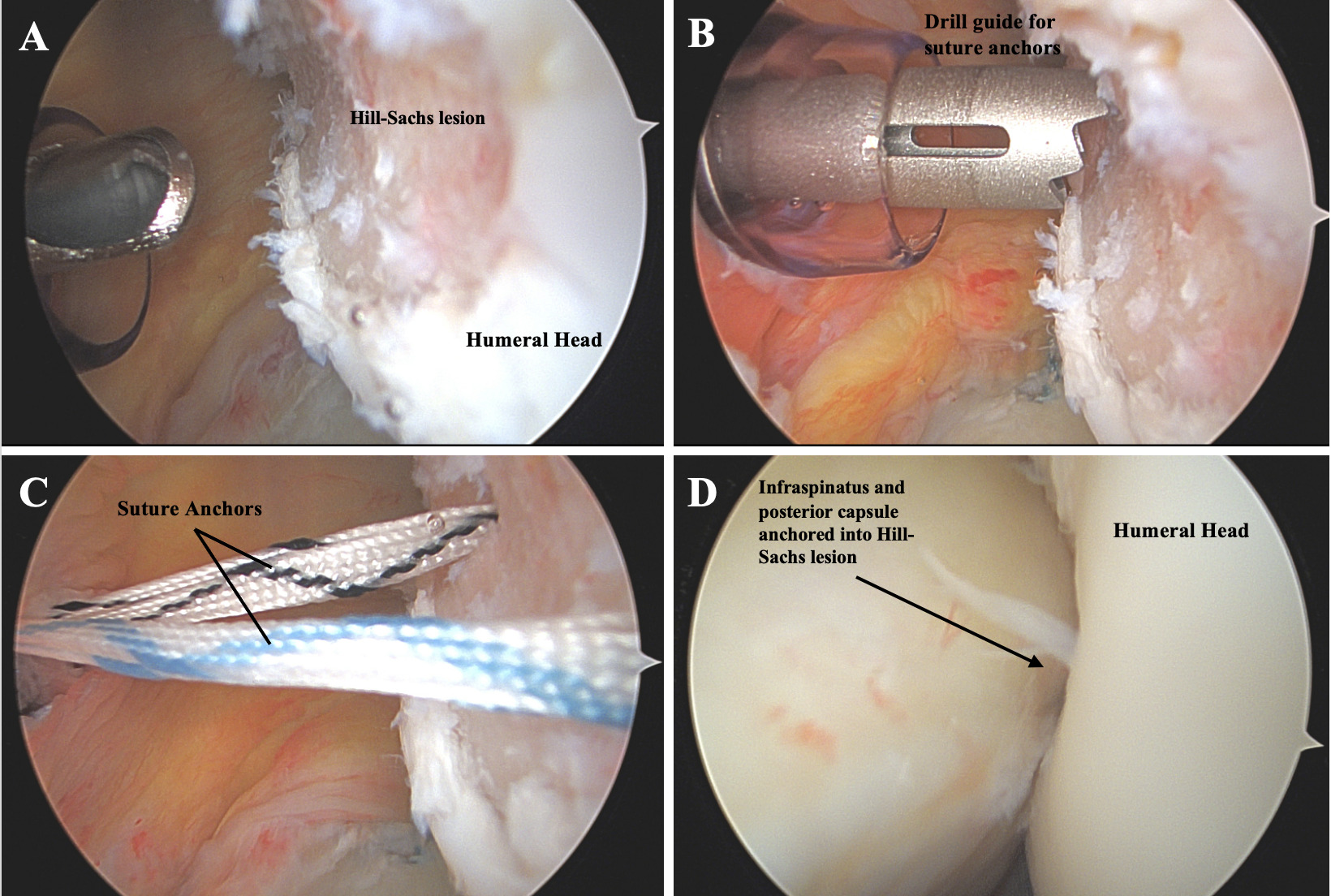
Remplissage entails filling the Hill-Sachs lesion, a posterolateral humeral head defect (Figure 1A, B), using an infraspinatus tenodesis and posterior capsulodesis for joint stabilization to prevent anterior shoulder instability.18 One method for performing a remplissage uses anchors placed into the Hill-Sachs defect (Figure 1C). This procedure involves standard arthroscopic Bankart preparation using anterior portals, preparation of the Hill-Sachs defect via a posterior working portal, and placement of one or two anchors in the defect. Sutures are passed through the infraspinatus tendon and posterior capsule and then tensioned to compress the tendon and capsule into the lesion (Figure 2). This effectively converts the lesion from intra-articular to extra-articular, preventing engagement of the anterior glenoid rim with the Hill-Sachs defect.16,18,19 It also serves as a check rein for the humeral head from sliding too anteriorly. Figure 2 shows arthroscopic pictures of a remplissage procedure performed in a patient.
_bankart_and_hill-sachs_lesion._(b)_illustration_detailing_axial_views_of_a_hill-sachs_.png)
_the_posterolateral_humeral_head_has_a_large_hill-sachs_lesion._(b)_a_guide_is_placed_t.png)
BIOMECHANICS OF REMPLISSAGE
Biomechanically, adding remplissage to Bankart repair aims to prevent Hill-Sachs engagement in the apprehension position (abduction-external rotation), restore normal shoulder stability, and reduce end-range laxity that predisposes patients to an anterior shoulder dislocation.20,21 Engagement refers to the Hill-Sachs lesion catching or locking onto the anterior glenoid rim, which can lever the humeral head anterior to the glenoid risking subluxation or dislocation. Cadaveric studies investigating these biomechanical benefits of remplissage generally support its use with ABR in cases where Hill-Sachs lesions are prone to engagement. In a bipolar-bone loss model (combined glenoid and humeral head defects), ABR alone failed to prevent engagement at end-range external rotation, whereas ABR with remplissage restored biomechanical stability in all specimens.22 A similar cadaveric study using models with moderate to large Hill-Sachs defects demonstrated that remplissage consistently prevented engagement, unlike the isolated ABR group.23 These biomechanical studies support ABR with remplissage as a humeral-side augmentation that consistently neutralizes engagement mechanics and thereby reduces the risk of recurrent instability.
CLINICAL OUTCOMES
Clinical evidence supporting remplissage exists across multiple studies. In the largest double-blinded multicenter randomized control trial evaluating remplissage, 108 individuals with minimal glenoid bone loss (<15%) were evenly assigned to ABR alone or ABR plus remplissage. Adding remplissage to ABR reduced redislocation rates at two years (18% ABR vs 4% ABR with remplissage), with no statistical difference in patient-reported outcomes or shoulder function.24 Their medium-term follow-up (≥4 years) yielded similar results, with failure (postoperative redislocation within one year) rates of 22% vs 8%, respectively, and recurrent instability (redislocation or ≥ 2 subluxations >1 year postoperative) rates of 30% vs 10%, respectively.25 Additionally, systematic reviews have also concluded that ABR with remplissage improves return-to-sport rates and reduces recurrent anterior shoulder instability in patients with Hill-Sachs lesions compared to ABR alone.13,26
In a large comparative meta-analysis, recurrent dislocations and revisions were significantly more common in the isolated ABR cohort (n=704) compared to the ABR with remplissage cohort (n=507). Villarreal-Espinosa et al. found higher odds of redislocation (OR = 4.22) and revision (OR = 3.36) after ABR alone, with no significant differences in ROM compared with the remplissage cohort.27
Athlete-focused data parallels these findings. In a systematic review including 538 athletes, 86% returned to sport after ABR plus remplissage, with higher odds of returning to any level (OR = 2.71) or to a previous or higher level (OR = 2.07) compared with isolated ABR. Moreover, recurrence of shoulder instability with remplissage was 5% in athletes and 7.3% overall, while the risk of reoperation (OR = 0.18) was significantly lower in ABR with remplissage when compared to alternative techniques.13
Long-term outcomes appear to remain stable. A systematic review of studies with ≥ 5-year outcomes (mean: 9 years) found that ABR with remplissage resulted in an overall 10% recurrent instability rate, 8% redislocation, and 76% return-to-sport rate, while also preserving external rotation.27 Current clinical evidence indicates that adding a remplissage to ABR decreases recurrent instability and reoperations while maintaining shoulder ROM.28
INDICATIONS
Patients at highest risk of failure after isolated ABR include young, contact athletes, patients with bipolar bone loss, and patients with high Instability Severity Index (ISI) scores.6,7,29–33 The senior author of this paper (AMM) considers adding remplissage for young high-risk patients and athletes in contact or overhead sports. Common indications for remplissage include engaging Hill-Sachs lesions with subcritical glenoid bone loss (<20%), contact athletes, high ISI scores, and revision after failed primary ABR (Table 1).20,34,35
Risk stratification tools like ISI aid clinicians in making informed decisions on surgical technique selection. ISI scores correlate with instability recurrence after ABR, with recurrence rising sharply with higher scores (i.e., 15% for ISI 0-3, 41% for ISI 4-6, and 71% for ISI >6), suggesting remplissage for management in high-risk profiles.36 In the setting of revision, remplissage has shown favorable stability and return-to-sport, further supporting its role when prior ABR has failed.26
REHABILITATION
Historically, one concern of ABR with remplissage was the possible loss of external rotation. Early literature identified conflicting limitations with internal and external ROM during abduction. However, more recent large comparative studies have demonstrated no difference in postoperative external rotation constraints between ABR and remplissage.17,37 Athlete and mixed-cohort meta-analyses further support these findings, depicting no clinically meaningful external rotation deficits with remplissage.27 Thus, conventional rehabilitation protocols used for isolated ABR are not typically changed for individuals undergoing ABR with remplissage.38 However, close communication between the surgeon and rehabilitation team should guide recovery based on the patient’s intraoperative findings and concomitant procedures for optimal recovery.
CONCLUSION
When paired with ABR, remplissage may reduce the risk of recurrent instability without a clinically meaningful loss of external rotation and may improve return-to-sports-rates compared to isolated ABR in athletes.