INTRODUCTION
Ankle sprains are among the most prevalent musculoskeletal injuries, especially in physically active athletes, accounting for approximately 16% to 40% of all sports-related injuries.1 Injuries to the lateral ligaments of the ankle are among the most frequently occurring injuries.2–4 These injuries carry a high risk of recurrence if not appropriately managed, potentially resulting in long-term instability and an increased likelihood of developing chronic ankle instability (CAI).5–7 Nearly 40% of individuals who sustain an ankle sprain progress to CAI within one year.8 CAI is a condition characterized by recurrent episodes of ankle sprains or subjective instability, commonly described as “giving way”. This condition can result in persistent pain and a perceived lack of stability in the ankle,9 leading to functional limitations in physical activities and reduced social participation.10 In contrast, some individuals sustain an ankle sprain but do not develop persistent symptoms of instability. These individuals, termed “copers”, successfully return to normal physical activity without experiencing recurrent giving way or chronic pain. Copers have demonstrated neuromuscular adaptations that allow them to maintain function despite their injury.11 However, the long-term consequences of residual impairments in copers remain unclear.12 Although most research on CAI has been conducted in adult populations, emerging evidence highlights its prevalence in pediatric populations as well. A previous study found that approximately 70% of children experienced an ankle sprain, with the prevalence of CAI reported at 36.6% among typically developing children aged 7 to 12 years.13 In sports, the prevalence of CAI is notably higher, particularly in court and indoor sports, where ankle injuries are most common.14,15 Research indicates that approximately 20% of young athletes develop to CAI, with female athletes experiencing a prevalence of 23.6% and male athletes of 16.3%.14 CAI is particularly concerning for athletes, as optimal ankle stability is essential for functional balance during sport-related activities and injury prevention.
Balance control relies on the central nervous system’s integration of sensory inputs from the visual, vestibular, and proprioceptive systems.16,17 Proprioception is defined as the ability to perceive body position and movement in space through the integration of sensory signals from various mechanoreceptors. It plays a crucial role in balance control by providing continuous feedback to the central nervous system, allowing for precise adjustments in posture and movement.18,19 Individuals with CAI often exhibit proprioceptive impairments due to damage to mechanoreceptors within the ligamentous and capsular structures of the ankle.20 These deficits disrupt the central nervous system’s ability to accurately detect joint position and movement, compromising neuromuscular control. Consequently, impaired proprioception in individuals with CAI can hinder their ability to maintain dynamic stability during weight-bearing activities. The impact of CAI in children studied by comparing balance, muscle strength, and physical activity levels between those with CAI and copers showed that children with CAI demonstrated impaired standing balance, lower limb muscle weakness, and reduced physical activity levels, highlighting the functional consequences associated with this condition.21 Although previous research has examined children with CAI, its prevalence and consequences among young athletes remain insufficiently understood, raising concerns about long-term functional impairments and injury risk in this population. The extent to which CAI affects static and dynamic balance in young athletes remains an important area for investigation. Therefore, this study aimed to investigate static and dynamic balance performance in young athletes between 8 and 16 years of age with and without CAI.
METHODS
Study design and participants
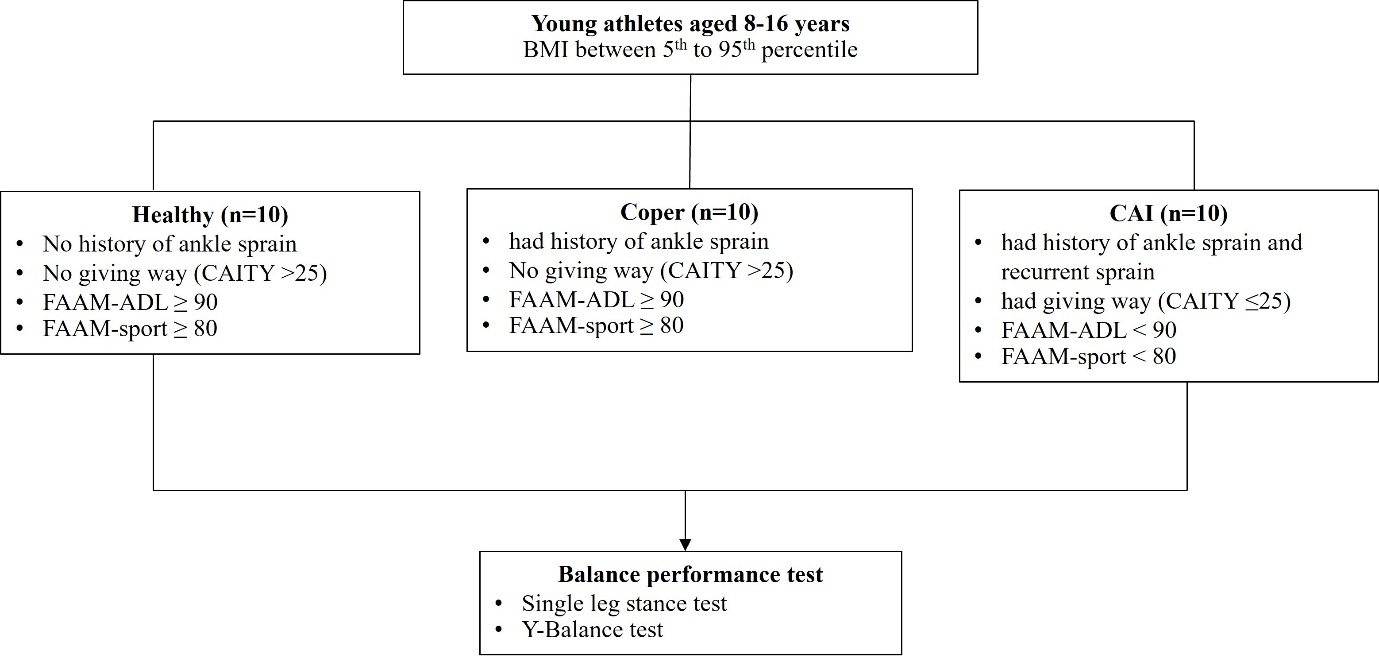
This study was a cross-sectional study. The setting areas of the study was sport training schools in Chiang Mai, Thailand. The sample size was calculated using the G-Power software version 3.1.9.4 with effect size = 0.6, power = 0.8, and α = 0.05. Consequently, a total of thirty participants were required (10 participants without ankle sprain, ten copers and ten participants with CAI). The study aimed to compare balance performance among these groups, providing insights into the impact of previous ankle sprain on postural control and stability. This study employed a convenience sampling method, recruiting participants from sport training schools (Taekwondo and Badminton) in Chiang Mai. All participants were enrolled using the inclusion criteria as follows: young athletes aged from 8 to 16 years, with a body mass index (BMI) ranging from the 5th to the 95th percentile. Participants were excluded from this study if they had a prior history of musculoskeletal surgery or fractures to either lower limb, bilateral CAI, or experienced an acute musculoskeletal injury in the lower extremities within the previous three months. Participants were interviewed to collect characteristic information and detailed histories of ankle sprains, including the onset of the first sprain, frequency of recurrent sprains, and episodes of ankle giving way. The Cumberland Ankle Instability Tool-Youth (CAIT-Y)22 was used to assess perceived ankle instability. Additionally, the Foot and Ankle Ability Measure (FAAM) was employed to evaluate ankle function, specifically in terms of activities of daily living (FAAM-ADL) and sports performance (FAAM-Sport). Participants were categorized into three groups based on the guidelines of the International Ankle Consortium.10,23 as detailed in the study protocol. (Figure 1)
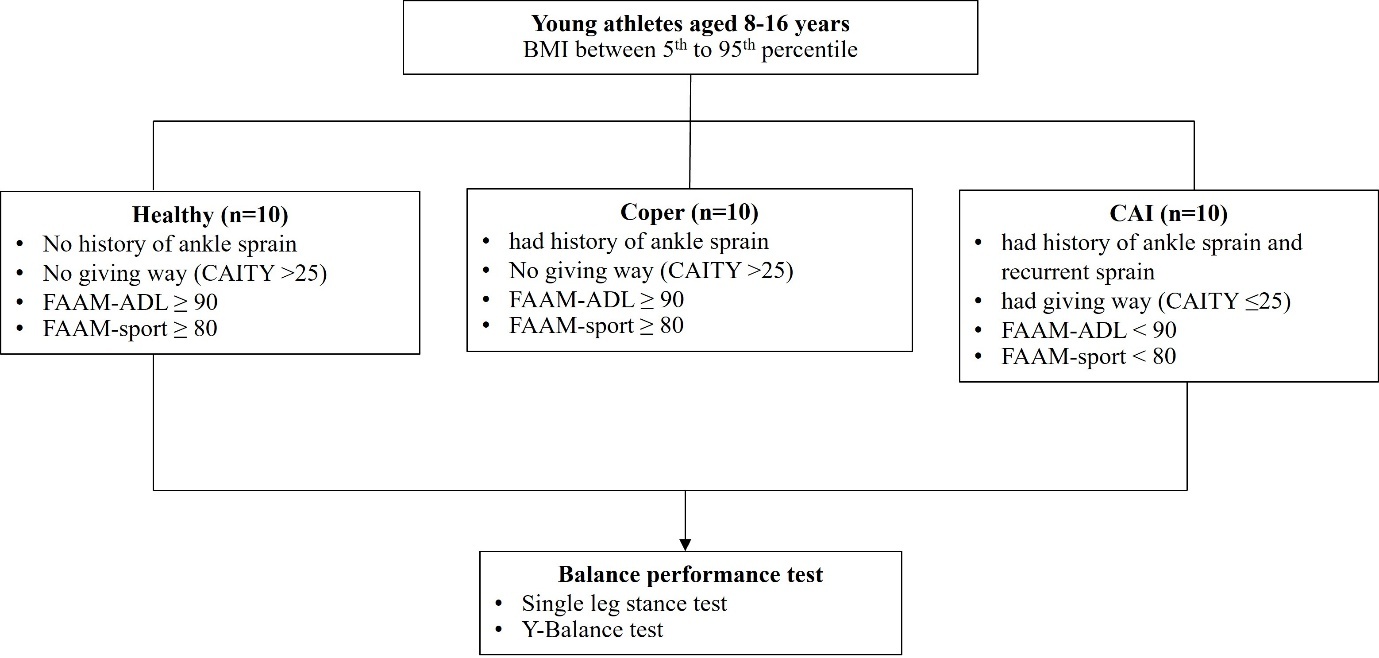
BMI, Body mass index; CAIT-Y, Cumberland ankle instability tool-youth; FAAM-ADL, foot and ankle ability measure-activities of daily living; FAAM-sport, foot and ankle ability measure-sport.
CAI group: Participants had a history of ankle sprains that resulted in at least one day of disrupted physical activity, with the initial injury occurring at least one year prior to study enrollment. Additionally, participants in this group exhibited a history of ankle giving way, recurrent ankle sprains (at least two occurrences), and/or a perceived sense of instability in the previously sprained ankle. Ankle instability was assessed using CAIT-Y, with an eligibility score of ≤ 25. In addition, the FAAM-ADL score was < 90, and the FAAM-sport score was < 80.
Coper group: Participants had a history of ankle sprains that disrupted physical activity for at least one day, with the initial sprain occurring at least one year prior to study enrollment. However, they did not report a history of ankle giving way or perceived instability in the previously injured ankle. Ankle instability assessed by CAIT-Y score >25. Additionally, participants in this group had successfully returned to their pre-injury level of physical activity without experiencing any functional limitations. Participants were required to have the FAAM-ADL score ≥ 90 and the FAAM-sport score ≥ 80.
Healthy Group: Participants had no history of ankle sprains. The CAIT-Y score > 25. The FAAM-ADL score ≥ 90 and FAAM-sport ≥ 80.
This study was performed consistent with the principles of the Declaration of Helsinki. Approval was given by the Ethical Committee Board of Date. 26 December 2024/No. AMSEC-67EX-101**.**
All participants provided a signed assent form, while their parents or legal guardians provided written informed consent before study enrollment.
Static balance assessment
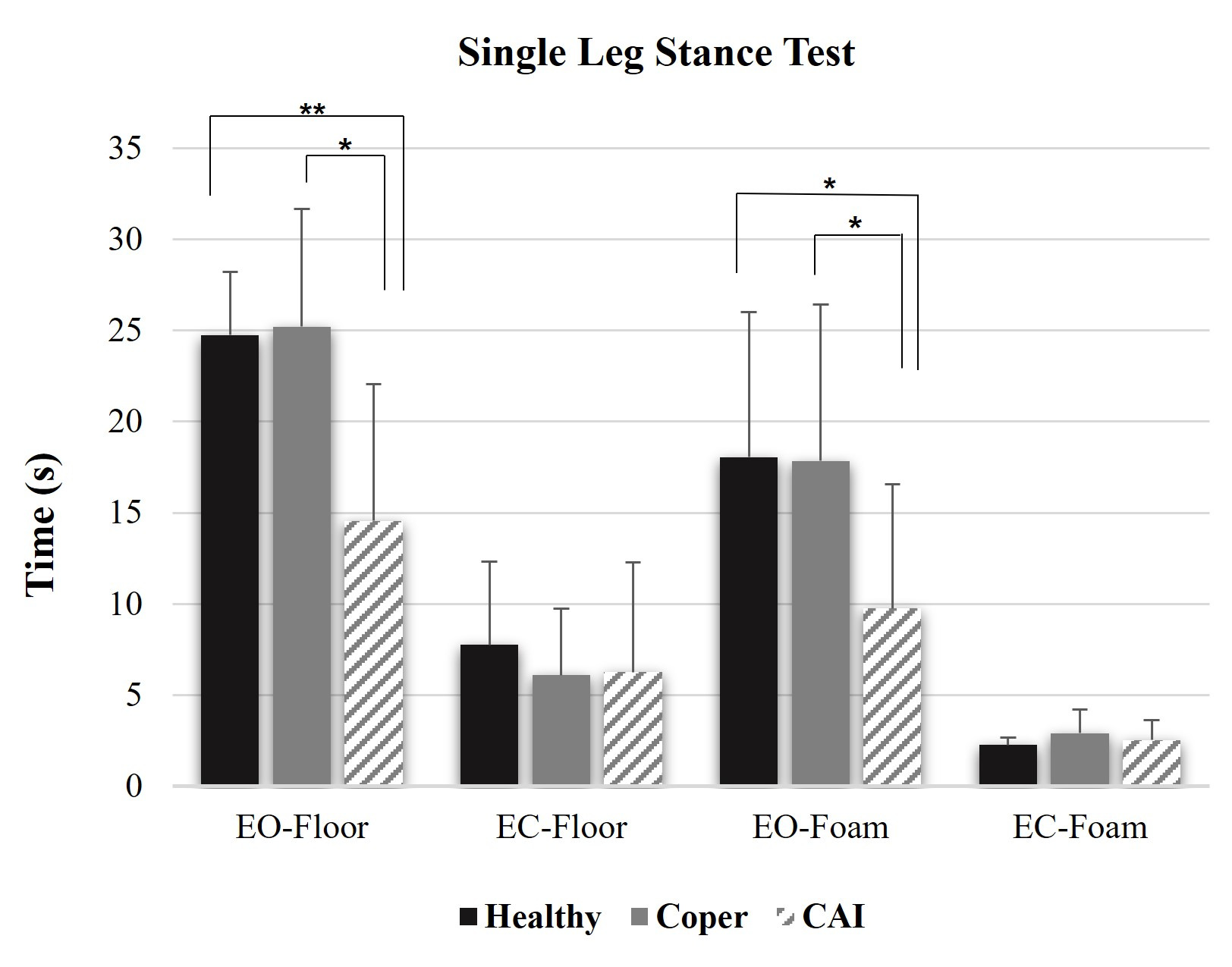
The Single-Leg Stance Test (SLST) was chosen for measuring static balance. Unipedal standing with eyes open and eyes closed was performed on a firm surface and an Airex balance pad (thickness: 6 cm). Four specific conditions, including 1) Single-leg stance on a firm surface with eyes open (EO-floor), 2) Single-leg stance on a firm surface with eyes closed (EC-floor), 3) Single-leg stance on a foam surface with eyes open (EO-foam), and 4) Single-leg stance on a foam surface with eyes closed (EC-foam), were randomly measured to mitigate any order effects. Participants with CAI and copers performed barefoot on the leg with a history of ankle sprain, whereas participants in the healthy group performed on their dominant leg with their hands placed on their hips. The dominant leg was tested by kicking a ball.24 The dominant leg was defined as the leg preferred for kicking a ball. During the test, participants were asked to remain as still as possible. The criteria for ending the test: participants stand finish 30 seconds, the weight-bearing foot position was altered, a hand moved from their hips, or they opened their eyes before 30 seconds. A minimum rest period of one minute was provided between each trial to ensure that participants could perform the test without undue fatigue. The average score obtained from the three trials for each condition was subsequently used for analysis.
Dynamic balance assessment
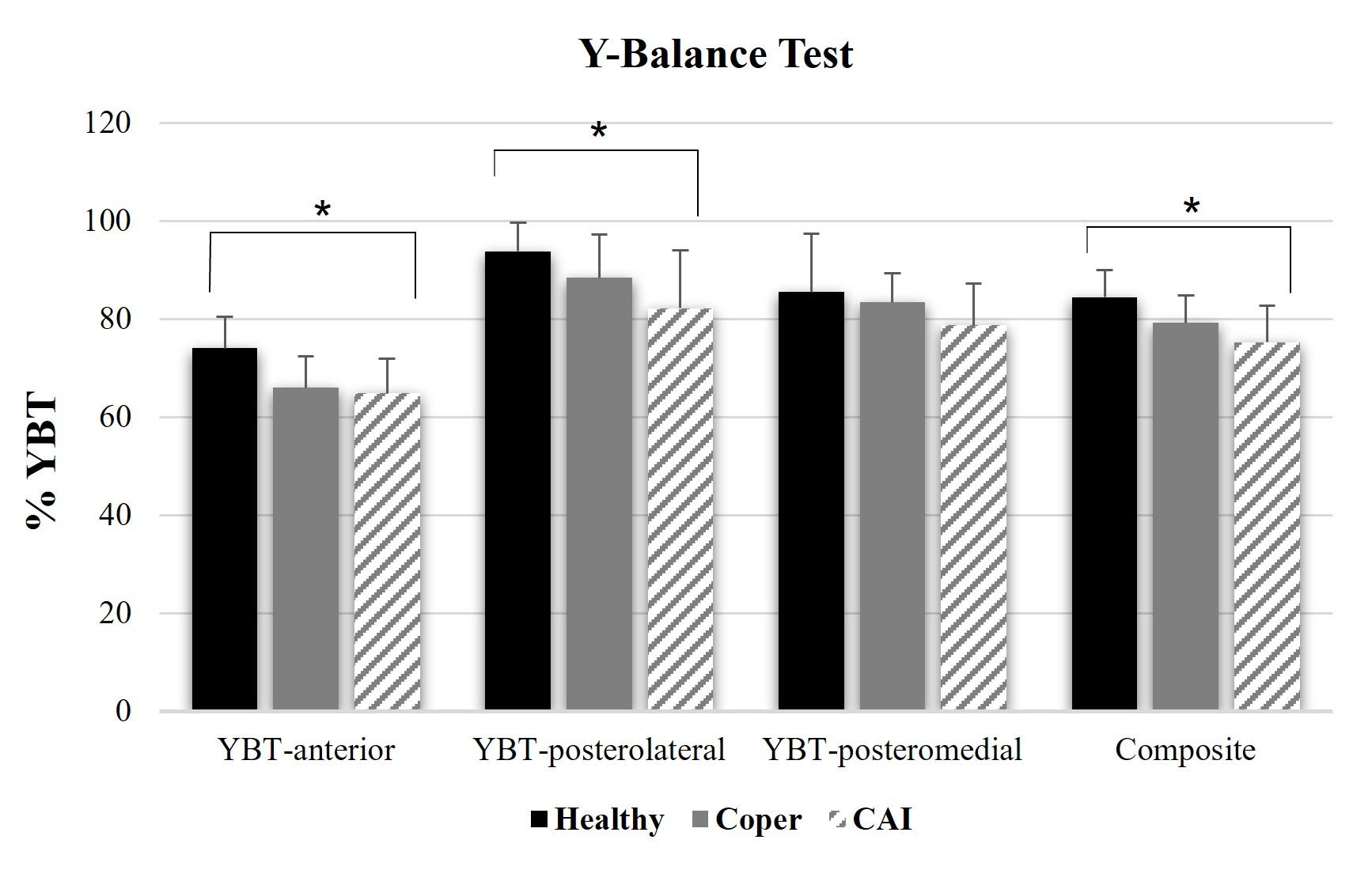
Dynamic balance was assessed using the Y-Balance Test (YBT), a shorter version of the Star Excursion Balance Test (SEBT). A systematic review has demonstrated that the YBT is a reliable tool widely used to measure dynamic neuromuscular control at the limits of stability in both injured and healthy athletic populations.25 The YBT evaluates dynamic balance in three directions: anterior, posterolateral, and posteromedial. In this study, participants with CAI and copers performed the test on the leg with a history of ankle sprain, while participants in the healthy group were assessed on their dominant leg. Each participant was instructed to stand barefoot on one leg with both hands placed on their hips while lifting the opposite leg off the floor. They were then asked to reach with the free limb as far as possible in three directions: anterior, posterolateral, and posteromedial directions, lightly contacting the floor and returning to the starting position without losing balance. Participants were allowed to practice six times in each direction before testing, so that the participant was familiar with the test. Each participant was tested in three trials in each direction. During testing, the trial was excluded and repeated if the participant failed to maintain a unilateral stance, such as touching the floor with the reaching foot or being unable to return to the starting position. Reach distance was recorded in centimeters. The normalized reach distance score was calculated by dividing the average reach distance by limb length and then multiplying by one hundred to express as a percentage (%YBT) in each direction. The composite score was computed by averaging the three normalized reach directions that represent the overall performance on the test.26
Intra-rater reliability of the assessor was evaluated before data collection. SLST demonstrated good to excellent intra-rater reliability across all conditions: EO-floor, EC-floor, EO-foam, and EC-foam, with ICC (3,1) values of 0.907, 0.948, 0.928, and 0.738, respectively. Similarly, the YBT showed good to excellent intra-rater reliability across the three reach directions of anterior, posterolateral, and posteromedial with ICC (3,1) values of 0.940, 0.922, and 0.876, respectively.
Statistical analysis
The data were assessed for normality using the Shapiro-Wilk test, which confirmed a normal distribution. Characteristic variables, including age, weight, height, and BMI, were analyzed using descriptive statistics. A one-way ANOVA was conducted to compare differences among groups, followed by LSD post hoc tests for comparing between groups. Statistical significance was set at p < 0.05.
RESULTS
All participants engaged in regular sports training for a minimum of one hour per day, at least three days per week, and maintained continuous training for at least one year. The mean and standard deviation of participant characteristics are presented in Table 1. Statistical analysis revealed no significant differences in these characteristics among groups in terms of age, weight, height, and BMI. However, a significant difference was observed in CAITY scores, FAAM-ADL, and FAAM-sport among the groups.
CAIT-Y, Cumberland ankle instability tool-youth; FAAM-ADL, foot and ankle ability measure-activities of daily living; FAAM-sport, foot and ankle ability measure-sport.
Static balance
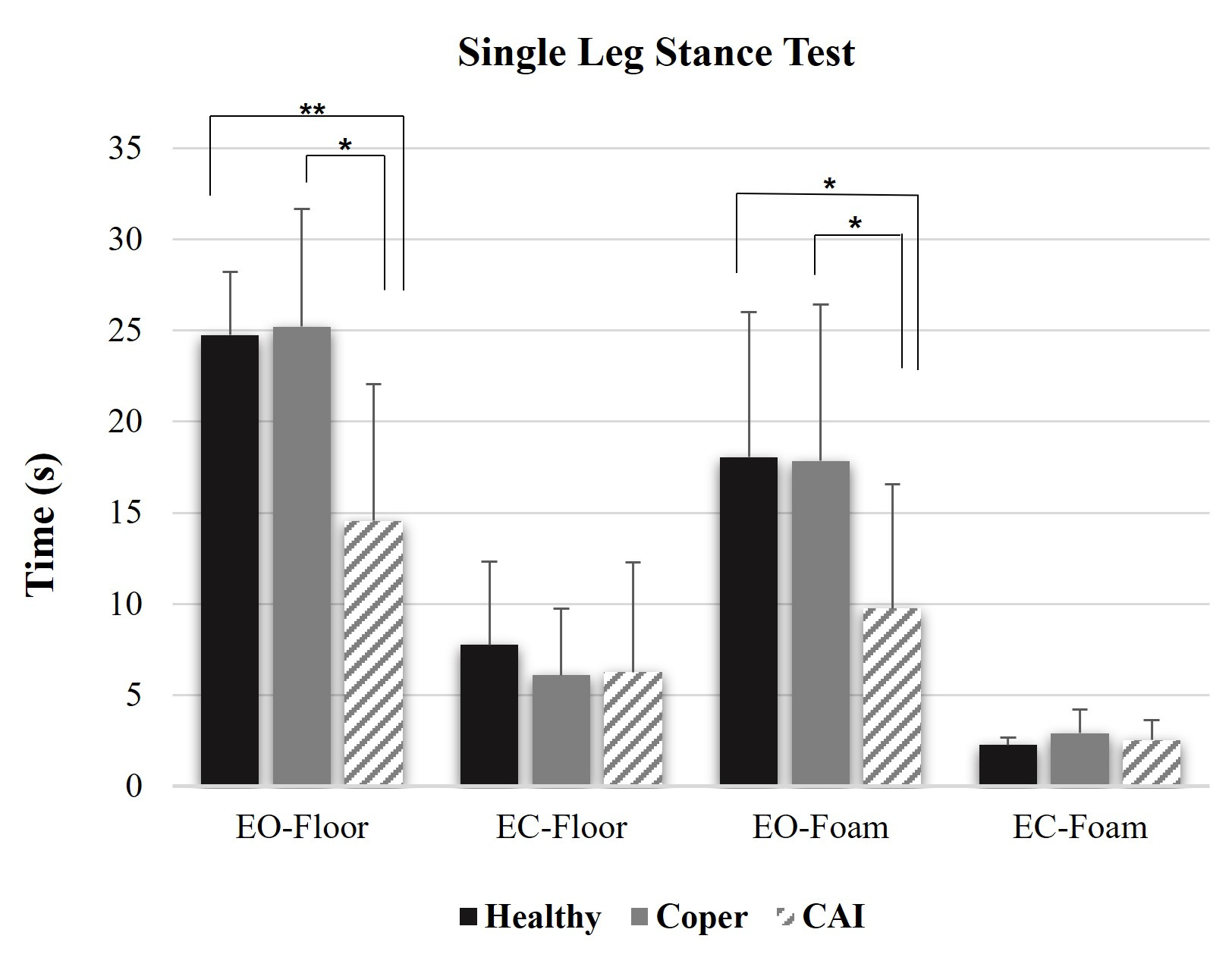
The SLST results are presented in Table 2. Participants in the healthy and coper groups were able to maintain balance for a longer duration when compared to the CAI group. Statistical analysis revealed significant differences among groups in the EO-Floor (p=0.001) and EO-Foam (p=0.039) conditions. However, no differences were observed in the EC-Floor and EC-Foam conditions. Post-hoc analysis revealed significant differences in the EO-Floor and EO-Foam conditions.The difference between the healthy and CAI groups, as well as between the copers and CAI, are shown in Figure 2.
Dynamic balance
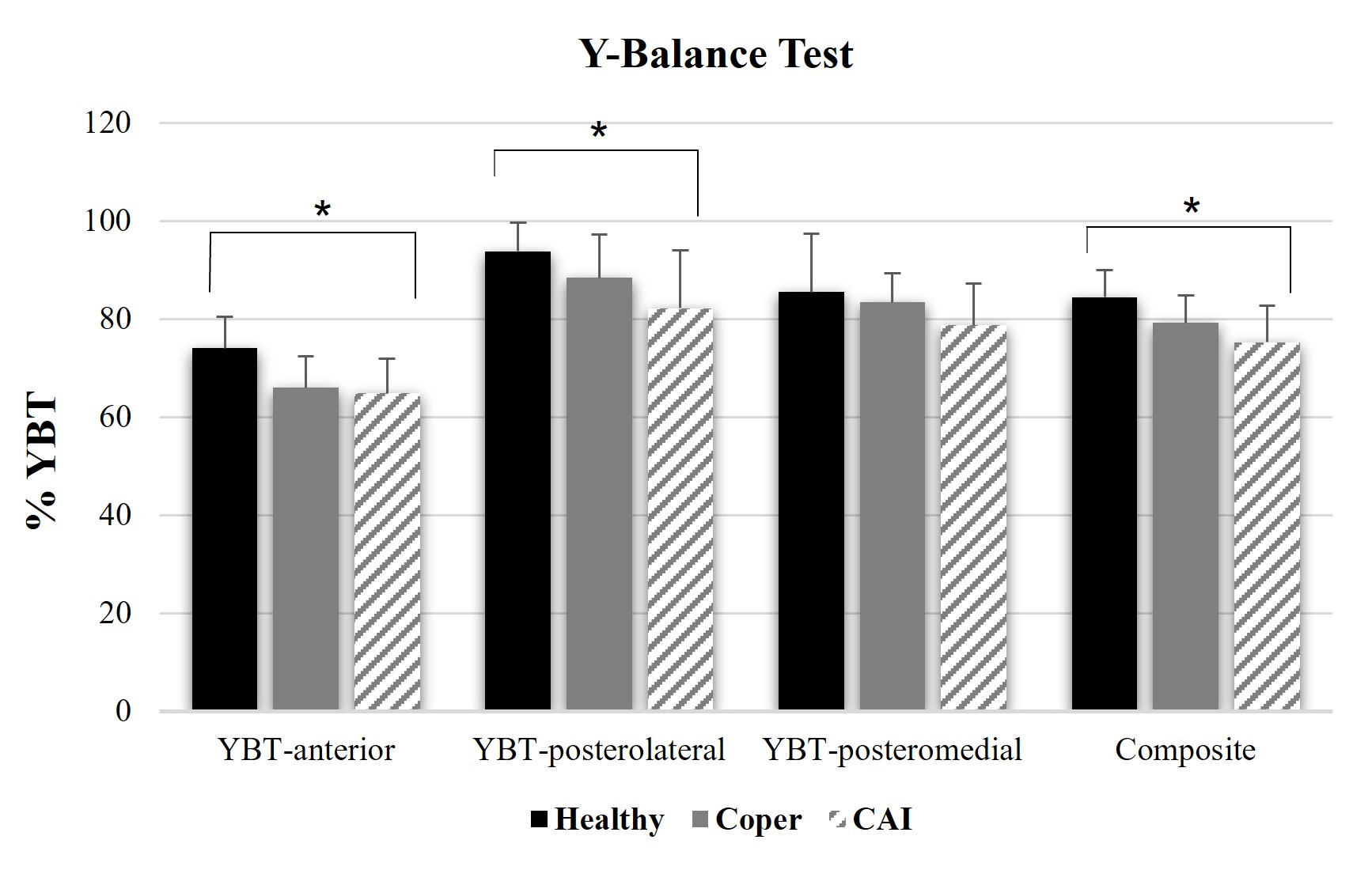
The YBT results are presented in Table 3. Statistically significant differences are identified among groups in anterior reach distance (p=0.009), posterolateral reach distance (p=0.031), and composite score (p=0.01). Post-hoc analysis further revealed differences between groups, as shown in Figure 3.
DISCUSSION
The present study assessed static and dynamic balance performance in young athletes comprising healthy, coper, and CAI groups. The results revealed that participants with CAI exhibited a significantly poorer balance compared to both healthy and coper participants. This finding was consistent with previous studies that have documented impaired balance in individuals with CAI.27 However, most of the existing research on CAI has predominantly focused on adult populations, highlighting the need for further investigation into pediatric populations. Young athletes are especially vulnerable to sports-related injuries due to skeletal immaturity and underdeveloped motor coordination,28 making it crucial to understand and address CAI in this population.29
In terms of static balance, both healthy and copers demonstrated significantly better balance performance than the CAI group in the EO-floor and EO-foam conditions. This indicated that participants with CAI exhibit deficits in postural control due to sensorimotor impairments and proprioceptive deficits.30,31 However, no differences were observed between groups in the EC conditions on either the floor or foam surfaces. One explanation for this reliance on visual input among young athletes is that the organization of sensory contributions to balance control may differ in this population. Previous studies suggest that younger children tend to rely more on visual cues for postural control, whereas adults primarily depend on somatosensory inputs when all sensory modalities are available.32 In adults, sensory integration on stable surfaces predominantly relies on proprioception (70%), followed by vestibular input (20%) and visual input (10%).33 However, the precise age at which postural control reaches adult-like maturation remains a subject of debate. The previous study suggested that children attain adult-like sensory integration during bipedal stance by approximately 12 years of age.34 This finding contrasts with the theoretical frameworks suggesting that athletes generally rely less on visual input due to enhanced proprioceptive and vestibular adaptations gained through training. However, in high-level or precision sports such as badminton and taekwondo, visual cues become increasingly critical for tasks such as timing, spatial orientation, and hand-eye coordination. In addition, balance challenges were more pronounced when tasks were performed on foam surfaces, emphasizing the increased postural demands in all groups of participants. This finding was consistent with previous research showing that children in the examined age range experience greater difficulty during SLRT with EC.35
For dynamic balance, the CAI group demonstrated reduced reach distance in the anterior and posterolateral directions, as well as a lower composite score, compared with the healthy group when assessed using the YBT. These results aligned with previous studies that have reported significant differences in dynamic balance between copers and CAI group.21,27 However, while prior research identified differences in all directions, the current study found significant differences only in the anterior and posterolateral directions. This discrepancy could be attributed to population differences, particularly in relation to sport-specific adaptations to dynamic balance.36 The reduction in anterior reach distance might be associated with limited ankle dorsiflexion. Several studies have indicated that athletes with CAI often experience long-term consequences, including a reduction in the range of motion of ankle dorsiflexion.37–40 This limitation can negatively impact dynamic balance.12,41 Additionally, anterior reach distance has been identified as a predictor of lower extremity injuries, with studies indicating that an anterior right/left reach difference greater than 4 cm was associated with a 2.5-fold increased risk of sustaining a lower extremity injury.25 Another important factor influencing YBT performance is lower limb muscle strength. Improved muscle strength, particularly in the ankle, knee, and hip, has been associated with better dynamic balance and reach distances in the YBT.
Interestingly, no differences were found between the healthy and coper group when considering overall balance performance. Both groups demonstrated superior static balance compared to the CAI group. However, when evaluating dynamic balance, which is essential for athletic performance and movement, no differences were found between CAI and copers. This contrasted with previous studies that reported that copers exhibited significantly better dynamic balance than individuals with CAI.21 In the current study, the copers demonstrated reduced dynamic balance performance, although the differences between groups were not significantly different. This suggests that even though copers can return to physical activity without recurrent instability, residual deficits in dynamic stability may persist. Consequently, this impairment may contribute to the potential transition from copers to CAI over time. Previous studies have indicated that individuals classified as the coper group may still experience neuromuscular deficits that predispose them to future instability and injury recurrence.11 As a result, targeted interventions focusing on neuromuscular control and proprioceptive training may be essential in preventing the progression from copers to CAI. Thus, it may be important to implement appropriate recovery interventions for both young athletes with CAI and those who are copers.
Despite the valuable findings, this study has some limitations that need to be addressed in future research. The small sample size of thirty participants may limit the generalizability of the results, and a larger sample would provide more statistical power. Additionally, the cross-sectional design restricts causal conclusions about the progression of CAI and its impact on future injuries; longitudinal studies are needed to assess how balance deficits evolve over time. The lack of kinematic and neuromuscular assessments also limits a deeper understanding of the underlying mechanisms of balance impairments in CAI, and advanced techniques like motion capture or electromyography could offer more insight. Addressing these limitations in future research would help provide a clearer understanding of CAI in pediatric populations and improve intervention strategies for preventing injury recurrence.
CONCLUSION
The results of this study indicate that young athletes with chronic ankle instability (CAI) exhibit significantly poorer static and dynamic balance compared to healthy and coper groups, underscoring the need for targeted interventions. Additionally, while copers demonstrate some recovery, they still exhibit residual deficits in dynamic stability that could predispose them to future injuries. These findings highlight the importance of incorporating neuromuscular control and proprioceptive training in rehabilitation programs for young athletes. Addressing these factors may help prevent the progression from copers to CAI, ultimately improving clinical outcomes and reducing the risk of reinjury.
Corresponding author
Jaruta Kunritt
Department of Physical Therapy, Faculty of Associated Medical Sciences, Chiang Mai University, Thailand
Tel: +6653-94-9248
Fax: +6653-93-5072
E-mail address: jaruta.kun@cmu.ac.th
Acknowledgements
All participants and their parents were gratefully acknowledged.
Conflict of interest
The authors declare no conflict of interest.