INTRODUCTION
Anterior cruciate ligament (ACL) injury is one of the most common traumatic events in young, physically active populations, particularly those engaged in pivoting sports.1,2 ACL reconstruction (ACLR) is frequently performed to restore knee stability and facilitate safe return to high-level athletic activity.3–5 However, despite advances in surgical techniques and rehabilitation protocols, neuromuscular deficits frequently persist several months after surgery.6–9 These deficits are especially prominent in eccentric force generation, neuromuscular control, and inter-limb symmetry—factors known to influence re-injury risk and long-term functional outcomes.10,11 Even at the time of medical clearance to return to sport, athletes may demonstrate significant functional asymmetries and neuromuscular inhibition, particularly in the quadriceps muscle group.6,12–14
The persistence of these impairments underscores the importance of objective, task-specific assessments that can capture subtle neuromuscular deficits during rehabilitation.15–18 Among such tools, the countermovement jump (CMJ) has gained widespread use for assessing lower limb performance in both athletic and clinical settings. CMJ testing, particularly when performed on dual force platforms, enables precise quantification of kinetic variables related to both concentric and eccentric muscle actions.19,20 This approach allows clinicians to analyze not only overall jump output, such as height or power, but also critical biomechanical features of the eccentric (braking) phase of movement.
Eccentric peak force (EPF), eccentric impulse (EI), and eccentric rate of force development (RFD) are three kinetic variables derived from the eccentric phase of the CMJ that may be particularly informative during post- ACLR assessment.20–22 EPF reflects the maximal force absorbed during the braking phase, EI represents the total eccentric load integrated over time, and RFD characterizes how rapidly force is generated during the initial eccentric deceleration. Each of these variables is theoretically linked to joint stability, neuromuscular control, and injury risk mitigation during dynamic tasks such as landing and cutting.23,24
Despite growing interest in these metrics, their clinical application remains limited, largely due to uncertainties surrounding their reliability, particularly in injured populations.25 While jump height and concentric impulse have consistently demonstrated high reliability across populations and testing conditions, eccentric variables like eccentric RFD are more technically sensitive. Several studies have reported high coefficients of variation (CV) and only moderate intraclass correlation coefficients (ICC) for eccentric RFD, suggesting that it is more vulnerable to intra-individual variability, movement strategy, and task execution errors.25,26 Furthermore, the majority of CMJ reliability research has been conducted in healthy or elite athlete populations, leaving a gap in knowledge regarding typical clinical cohorts undergoing rehabilitation after ACLR.
Importantly, current return-to-sport (RTS) decisions often rely on strength or performance-based criteria such as hop tests or isokinetic ratios, which may not capture the neuromuscular quality of eccentric control.19,27 Given that neuromuscular asymmetries and proprioceptive alterations can persist even after strength appears restored, the inclusion of eccentric kinetic analysis from CMJ could provide a more comprehensive and sensitive assessment of readiness.20–22 It is important to note that measurement reliability is a prerequisite for clinical utility but does not, in itself, establish sensitivity to functional recovery, return-to-sport readiness, or injury risk
The purpose of this study was to evaluate the intra-session reliability and variability of selected eccentric-phase CMJ variables in physically active individuals six months after ACLR.
METHODS
Study Design
This study represents a retrospective secondary analysis of prospectively collected clinical data. Although the CMJ testing protocol was standardized and implemented prospectively as part of routine clinical follow-up, the present reliability analysis was conducted retrospectively using previously collected data. This study followed a retrospective observational design aimed at assessing the intra-session reliability and intra-individual variability of eccentric kinetic variables derived from the CMJ in patients who had undergone ACLR. The methodological framework adhered to the Guidelines for Reporting Reliability and Agreement Studies (GRRAS), ensuring a standardized, transparent, and reproducible approach to data collection and reporting.28
All procedures were carried out in accordance with the ethical principles outlined in the Declaration of Helsinki. The research protocol received approval from a local institutional review board (IRB approval number: PCE-0623-148). Prior to participation, all patients were provided with a detailed explanation of the study’s objectives and procedures and gave written informed consent.
Participants
Participants were retrospectively identified from a clinical database using a consecutive sampling approach. All patients who met the inclusion criteria and completed the standardized six-month postoperative testing battery during the study period were included in the analysis. Data were collected between 09/01/2025 and 05/12/2025 at Clinic of Domont, Domont, France, where all CMJ assessments were performed using dual force platforms under standardized testing procedures.
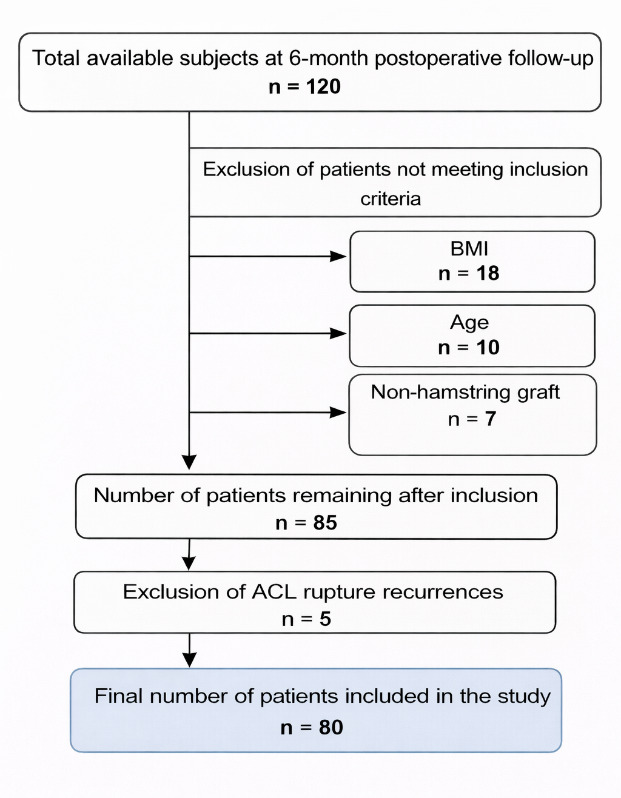
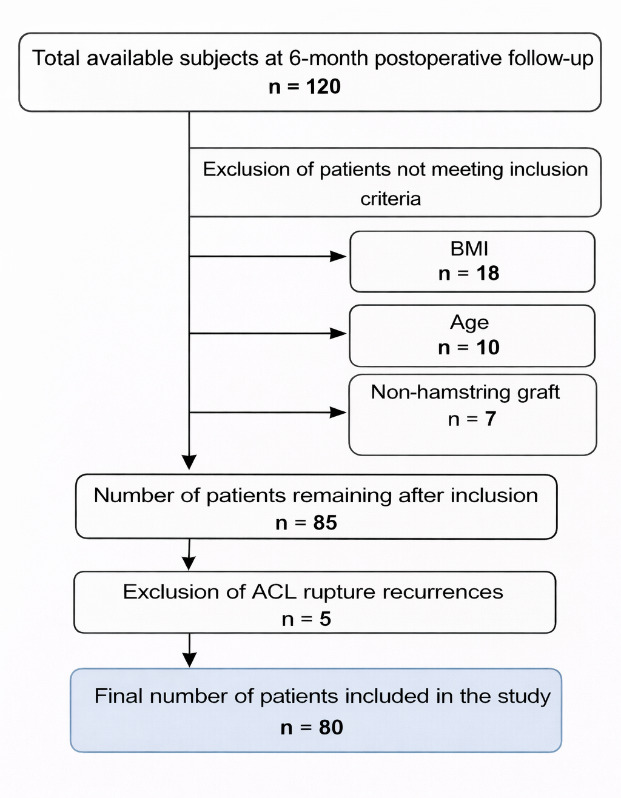
Eligible participants were aged between 18 and 50 years and had a body mass index (BMI) below 30 kg/m². They were also required to be physically active, as evidenced by a minimum score of 4 on the Tegner Activity Scale. Exclusion criteria included a history of ACL injury on the contralateral limb, revision ACL surgery, and any concomitant musculoskeletal injuries such as meniscal tears or collateral ligament damage. Concomitant ligamentous or meniscal injuries requiring surgical repair were excluded to ensure a homogeneous ACLR cohort and to minimize potential confounding effects on eccentric kinetic performance and reliability metrics. While this approach may limit generalizability to more complex injury presentations, it was considered necessary to isolate the reliability characteristics of eccentric CMJ variables in a standardized post-ACLR population. Patients who had presented post-surgical complications that could have impacted functional testing were also excluded. (Figure 1).
Eighty participants were included in the study, each at six months after a primary ACLR performed using a hamstring tendon autograft. All surgeries were conducted in the same clinical setting by one of three experienced orthopedic surgeons using a standardized surgical protocol. All reconstructions were performed using a single-bundle arthroscopic technique with ipsilateral hamstring tendon autograft fixation following the same institutional surgical protocol. The graft was harvested from the involved limb. This time point—six months postoperatively—corresponds to an advanced phase of rehabilitation during which neuromuscular evaluation is clinically relevant for guiding return to sport decisions.19,29
Post-operative rehabilitation followed a structured, criteria-based framework aligned with contemporary ACLR rehabilitation guidelines.30–32 While progression was individualized according to clinical presentation and objective recovery milestones (e.g., pain, swelling, strength, functional capacity), the overall ACLR rehabilitation phases and exercise progression model were standardized across patients.33,34 ACLR rehabilitation was supervised by four licensed physiotherapists with five to seven years’ experience in ACLR rehabilitation. During the early post-operative phase, participants typically attended supervised sessions three times per week, with frequency adjusted progressively based on recovery status.31,33,35,36
Sample Size Calculation
The sample size was determined using the formula proposed by Walter et al. for reliability studies involving ICC.37 Assuming a minimally acceptable ICC of 0.75 and an expected ICC of 0.85, with a statistical power of 80% and a significance level of 0.05, the recommended sample size was 77 participants (G3 Power v3.1).38
Protocol and Measured Variables Test
Biomechanical testing was conducted during a single standardized session using dual force platforms (K-Deltas V3, Kinvent Biomechanics, Montpellier, France) sampling at 2000 Hz.39,40 Participants performed three maximal bilateral CMJs, with a 60-second rest interval between each trial to minimize fatigue.13 Limb dominance was recorded based on the participant’s self-reported preferred kicking leg.
Prior to testing, all participants completed a structured warm-up consisting of five minutes of low intensity cycling on a stationary bike, followed by ten bodyweight squats performed to approximately 90 degrees of knee flexion. They then performed three submaximal CMJs to become familiar with the test conditions and reduce learning effects.41
During the jump trials, During the jump trials, CMJ testing procedures were standardized. Participants received scripted verbal instructions and were instructed to jump “as fast and as high as possible” while keeping their hands on their hips. A demonstration was provided prior to testing, and all assessments were conducted by the same examiner to ensure procedural consistency. All movements were supervised by a licensed physiotherapist with 15 years of clinical experience in ACLR rehabilitation to ensure consistency and compliance with testing instructions.
Force-time data were sampled at 1000 Hz and processed using a low-pass second-order digital Butterworth filter with a cutoff frequency of 50 Hz, consistent with the manufacturer’s CMJ signal-processing procedures. The selected cutoff frequency preserves the rapid characteristics of eccentric force development while minimizing high-frequency signal noise. Event detection (e.g., movement onset, initiation of the eccentric phase, and transition from eccentric to concentric phase) was determined using force threshold and velocity-based criteria derived from the vertical ground reaction force signal. Body weight was established during a quiet standing period prior to each trial and used to define movement onset. All data processing and metric calculations were performed using K-Force software (Kinvent, Montpellier, France; version 2.20.0).
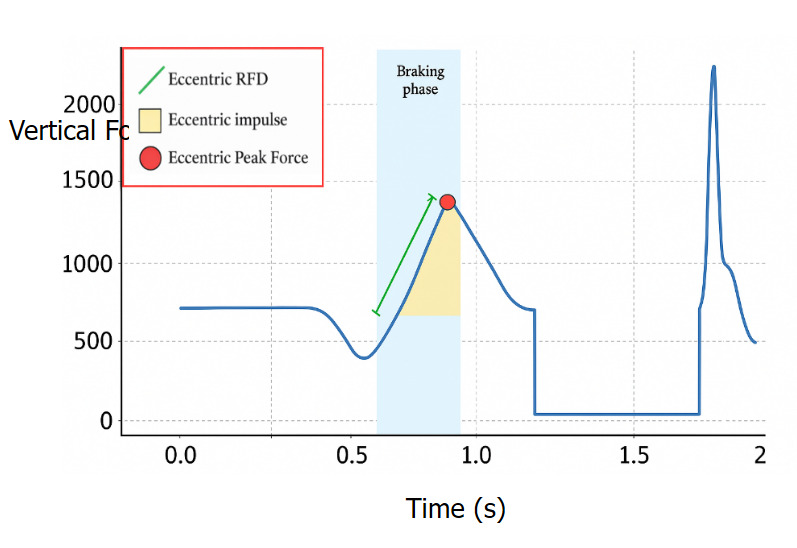
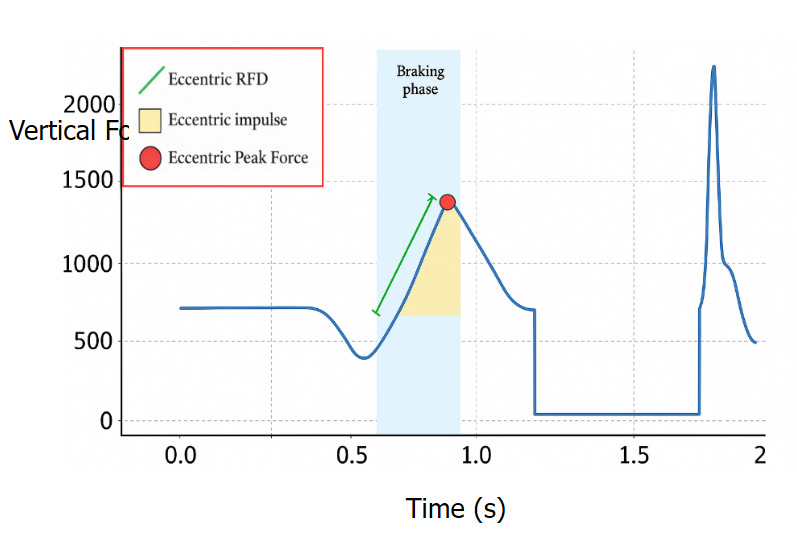
Three eccentric kinetic variables were extracted from the vertical ground reaction force (vGRF) data collected during the braking phase of the CMJ (Figure 2):
-
Eccentric RFD was calculated as the slope of the force-time curve over the first 200 milliseconds after the vGRF exceeded body weight. This measure reflects the rapidity with which force is produced during the eccentric phase and is expressed in Newtons per second (N·s-1).42–44 A fixed 200-ms window was used to standardize RFD computation across participants and trials. However, because RFD is derived from the slope of the force–time curve, it is sensitive to signal noise and to small variations in movement execution and phase timing.45
-
EI was defined as the area under the vGRF curve during the braking phase, specifically from the moment the force surpassed body weight to the point of zero center of mass velocity. It quantifies the total force absorbed eccentrically and is reported in Newton-seconds (N·s).46
-
EPF was measured as the highest vGRF value recorded during the eccentric portion of the movement, just before the concentric phase began. This value reflects the peak eccentric load and is expressed in Newtons (N).43
All variables were recorded simultaneously and analyzed separately for the operated (OP) and non-operated (NOP) limbs to explore asymmetries and assess reliability within a clinical rehabilitation context.
Statistical Analysis
All statistical analyses were conducted using JASP software (version 0.19.3, JASP Team, Amsterdam, Netherlands). Preliminary data processing, including the calculation of mean values from the jump trials and formatting the data for analysis, was performed using Microsoft Excel.
Descriptive statistics were calculated for each kinetic variable, including means and standard deviations. In addition, 95% confidence intervals were reported to provide an estimate of the precision of the mean values. These values were computed separately for the operated and non-operated limbs.
Intra-session reliability was assessed using ICC (3,1), based on a two-way mixed-effects model for absolute agreement of single measurements. For all these measures, 95% confidence intervals were also calculated to indicate the precision of the reliability estimates. The interpretation of ICC values followed the classification proposed by Koo and Li , in which ICC values < 0.50 indicate poor reliability, 0.50–0.75 indicate moderate reliability, 0.75–0.90 indicate good reliability, and values > 0.90 indicate excellent reliability.47
To quantify the magnitude of measurement error, the SEM was calculated using the formula SEM = SD × √(1 − ICC).48 SEM was also expressed as a percentage of the mean score for each variable, facilitating comparisons across variables and supporting clinical interpretation.
To assess absolute intra-session reliability, the CV was computed for each kinetic variable as the ratio of the standard deviation to the mean, expressed as a percentage. A CV of less than 10% was considered low variability, between 10% and 20% as moderate, and greater than 20% as high, in line with established guidelines by Atkinson and Nevill and Cormack et al.49,50
All reliability and variability analyses, as well as performance values, were computed separately for the operated and non-operated limbs. This approach allowed for the detection of inter-limb discrepancies and performance asymmetries, while also providing insight into the potential impact of surgical intervention on the consistency and robustness of eccentric force measurements. Between-limb comparisons were conducted for descriptive purposes only and were not intended to establish clinical asymmetry thresholds or recovery criteria.
RESULTS
Participant Characteristics
A total of 80 participants were included in the final analysis (47 males, 33 females). ACLR was performed on the dominant limb in 56 participants (70%) and on the non-dominant limb in 24 participants (30%). The mean age was 29.2 years ± 8.367 years. The average height was 1.74 m ± 0.094, and the mean body mass was 72.8 kg ± 12.844, resulting in a mean body mass index of 23.80 kg.m-² ± 3.227. The average time elapsed since surgery was 195.20 days ± 22.362 (Table 1).
Kinetic Descriptive Data
Kinetic variables were recorded for each limb during three CMJ trials, focusing on the eccentric phase (Table 2). EPF on the OP limb had a mean of 631.71 N ± 53.79, while the NOP limb showed a mean of 745.48 N ± 47.85. The EI, , was 119.56 N·s ± 11.82 for the OP limb and 141.25 N·s ± 15.39 for the NOP limb. The eccentric RFD had a mean of 1055.76 N·s⁻¹ ± 351.75 on the OP limb and 1352.32 N·s⁻¹ ± 343.74 on the NOP limb.
Intra-Session Reliability
For EPF, the ICC was 0.87 on the OP limb (95% CI: 0.82–0.91) and 0.89 on the NOP limb (95% CI: 0.85–0.93). The SEM was 19.5 N for the OP limb and 15.5 N for the NOP limb. For EI, the ICC was 0.87 (95% CI: 0.82–0.91) on the OP limb and 0.84 (95% CI: 0.78–0.89) on the NOP limb. The SEM was 4.3 N·s for the OP limb and 6.2 N·s for the NOP limb. For RFD, the ICC was 0.62 (95% CI: 0.49–0.73) on the OP limb and 0.71 (95% CI: 0.61–0.80) on the NOP limb. The corresponding SEM values were 217 N·s⁻¹ and 184 N·s⁻¹ for the OP and NOP limbs, respectively (Table 3).
Intra-session variability
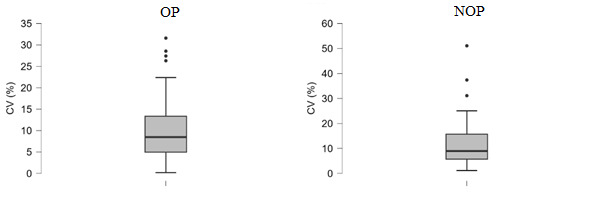
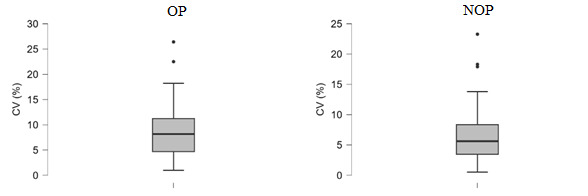
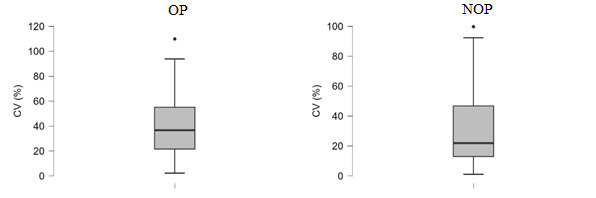
Intra-session variability was assessed using CV across the three CMJ trials (Table 4). For EI, the CV was 10.08% on the OP limb and 11.53% on the NOP limb (Figure 2). The CV for EPF was 8.58% on the OP limb and 6.41% on the NOP limb (Figure 3). For RFD, the CV was 39.81% on the OP limb and 30.83% on the NOP limb (Figure 4).
_-_eccentric_impulse.png)
_-_eccentric_peak_force.png)
_--_eccentric_rfd.png)
DISCUSSION
This study assessed the intra-session reliability of three eccentric kinetic variables—EPF, EI, and eccentric RFD—derived from bilateral CMJ in individuals six months after ACLR. It is essential to distinguish measurement reliability from clinical relevance. While reliable variables are necessary for longitudinal monitoring, reliability alone does not imply sensitivity to functional recovery, return-to-sport readiness, or ACL reinjury risk. The present findings therefore inform the consistency of eccentric CMJ metrics within a single session rather than their prognostic or decision-making value.
EPF showed good intra-session reliability, with ICC values of 0.868 for the OP limb and 0.895 for the NOP limb. The SEMs were 19.5 N and 15.5 N, respectively, representing less than 7% of the mean force values. Similarly, EI demonstrated consistent performance across trials, with ICCs of 0.868 for the OP limb and 0.840 for the NOP limb, and SEMs of 4.3 N·s and 6.2 N·s, respectively. These findings are consistent with previous studies conducted in healthy athletic populations showing that force- and impulse-based CMJ variables tend to be stable within a single testing session. Mizuguchi et al. reported ICC values greater than 0.89 and CV under 5.1% for net impulse and related parameters, suggesting low measurement error for these types of kinetic metrics.51 Merrigan et al. similarly observed that eccentric impulse and eccentric peak force were among the most reliable CMJ variables in healthy collegiate athletes, consistently achieving ICC values above 0.80.25
Eccentric RFD demonstrated the lowest intra-session reliability and the greatest variability among the kinetic variables examined. This finding is consistent with prior CMJ force–time reliability research conducted in healthy athletic populations, which have reported that RFD-derived metrics are typically among the least stable outcomes.17,18,25,51 In the present post-ACLR cohort, reliability values were of similar or slightly lower magnitude, which may reflect greater movement variability and neuromuscular alterations during ACLR rehabilitation. From a measurement standpoint, RFD is a derivative-based variable and is therefore inherently sensitive to signal noise, filtering decisions, and small timing errors around key event detection, which can amplify trial-to-trial dispersion even under standardized conditions.51 From a motor-control perspective, eccentric braking RFD is strongly influenced by jump strategy (e.g., countermovement depth and velocity, braking duration, and coordination of the descent-to-ascent transition), meaning that minor within-subject adjustments across repetitions may substantially alter the slope of the force–time curve without reflecting meaningful changes in eccentric capacity. Consistent with this interpretation, previous investigations have reported comparatively lower reliability and higher coefficients of variation for eccentric RFD compared with force- or impulse-based metrics, with CV values frequently exceeding 20% even in trained athletic populations.25,26 Collectively, these findings suggest that eccentric RFD—at least as operationalized in the present study—should be interpreted cautiously for within-session monitoring in post-ACLR assessment and may be less suitable than EPF or EI for detecting meaningful short-term changes at the individual level unless methodological refinements and inter-session responsiveness are further established.
Intra-session variability for the three eccentric kinetic variables—EPF, EI, and RFD—was evaluated using the CV across three CMJ trials on both the OP and NOP limbs. EPF showed relatively low variability, with CVs of 7.8% on the OP limb and 6.4% on the NOP limb. EI demonstrated slightly higher variability, with CVs of 10.2% and 11.3% for the OP and NOP limbs, respectively. These values fall within ranges generally considered acceptable for CMJ force-time variables, as previous studies in healthy athletic populations have reported CV values typically below 10–12% for force- and impulse-based metrics.49,50 Eccentric RFD demonstrated the highest variability, with a CV of 30.1% on the OP limb and 22.4% on the NOP limb.
In contrast, CVs for EPF and EI in this study remained below 12%, aligning with previously reported benchmarks. For example, Chang and Chiang demonstrated that eccentric peak force and mean force metrics from CMJs typically yield CVs under 10%, reinforcing their suitability for reliable within-session assessment.52 Nibali et al. also also confirmed that EPF and EI maintain relatively low error margins across trials, whereas eccentric RFD consistently displays larger fluctuations, likely due to its dependence on precise timing and greater sensitivity to small variations in movement execution.53
This pattern aligns with previous findings in the literature. Kotsifaki et al. observed significant limb asymmetries in athletes at RTS after ACLR, highlighting persistent reductions in concentric and eccentric impulse, as well as peak landing force, on the involved limb during bilateral CMJ and drop jump tasks, despite athletes meeting return-to-play criteria.20 Similarly, Read et al. reported asymmetries in eccentric deceleration impulse and RFD in professional soccer players more than nine months after ACLR, suggesting compensatory offloading strategies on the operated limb.54 In adolescent populations, Bakal et al. found exaggerated asymmetries in eccentric impulse and peak ground reaction force compared to healthy controls, especially during landing, further supporting the persistence of neuromechanical deficits post-ACLR.55
Persistent neuromuscular deficits after ACLR are likely multifactorial. Arthrogenic muscle inhibition, altered quadriceps motor unit recruitment, and changes in cortical excitability have all been reported to contribute to impaired voluntary activation and force production capacity in this population.8,35,56 Additionally, compensatory movement strategies and chronic underloading of the involved limb during dynamic tasks may reinforce asymmetrical braking mechanics and limit full restoration of eccentric control.17,18 These interacting factors may help explain why kinetic deficits persist even during advanced ACLR rehabilitation phases and underscore the importance of integrating neuromuscularly targeted interventions within return-to-sport decision frameworks.7,8,35,57
While these results confirm the presence of between-limb asymmetries, a key contribution of the present study lies in its analysis of intra-session reliability. EPF and EI demonstrated good reliability and low variability (ICC > 0.84, CV < 12%), supporting their suitability for clinical monitoring of eccentric performance. In contrast, eccentric RFD exhibited only moderate reliability and high variability (ICC < 0.72, CV > 20%), aligning with previous findings that highlight its sensitivity to execution inconsistencies and reduced reproducibility, particularly in clinical or high-velocity contexts.26,53
The bilateral CMJ protocol used in this study ensures high reproducibility and ease of standardization. Previous research has emphasized the value of unilateral jump tasks, such as single-leg CMJs or hop tests, to expose side-to-side differences in force output, timing, and strategy, particularly in post-ACLR populations.21,22,53 Including such unilateral assessments could enhance the sensitivity of eccentric phase analysis and better inform return-to-sport decisions.
Moreover, the present findings do not differentiate between active voluntary deficits, reflecting limited intentional output, and involuntary neuromuscular inhibition, typically linked to central factors. This distinction is crucial, as two individuals with similar eccentric force deficits may require different therapeutic approaches depending on whether the limitation stems from mechanical weakness or persistent neuromotor inhibition. As highlighted in recent work by Moiroux-Sahraoui et al., integrating electromyographic or neurocognitive tools may help characterize the nature of eccentric impairments and guide more personalized rehabilitation protocols.7,8,35
Despite the presence of clear performance asymmetries—consistent with previous literature on post-ACLR deficits17,18,21,22 — the ICCs and SEMs were remarkably similar between limbs. This suggests that measurement consistency remains intact, even on the reconstructed limb, supporting the use of these metrics for reliable within-limb and between-limb comparisons.
Similar findings were reported by Kotsifaki et al., who noted high within-session reliability for eccentric impulse and peak force in both limbs of ACLR athletes.20 Merrigan et al. also observed no significant differences in reliability between limbs in collegiate athletes when analyzing CMJ-derived force-time variables.25 These results collectively imply that limb status (OP vs. NOP) does not substantially affect the technical reliability of eccentric kinetic data when acquired under standardized conditions.
Clinically, these findings reinforce the importance of including both limbs in CMJ-based monitoring protocols and support the use of dual force plate analysis as a precise tool for tracking recovery trends over time. While EPF and EI demonstrated acceptable intra-session reliability in both limbs, the persistence of kinetic asymmetries underscores the need for limb-specific evaluation during rehabilitation. As athletes progress beyond the six-month time point, improvements in quadriceps strength, eccentric control, and limb loading symmetry would be expected to increase both the magnitude and stability of eccentric kinetic outputs. However, the differential reliability observed across variables suggests that not all eccentric metrics provide equivalent clinical insight. In particular, although bilateral CMJ testing offers valuable global information, compensatory force redistribution from the non-operated limb may partially mask persistent eccentric deficits in the operated limb.18 Therefore, good intra-session reliability should not be equated with high sensitivity for detecting clinically meaningful asymmetries. Collectively, these considerations highlight the value of dual force plate analysis not only for identifying kinetic imbalances but also for selecting the most clinically appropriate variables according to the stage and goals of ACLR rehabilitation.
These results emphasize the importance of selecting robust and stable metrics—such as EPF and EI—when assessing neuromuscular recovery and guiding RTS decisions in ACLR populations
LIMITATIONS AND PERSPECTIVES
This study presents several methodological limitations. The retrospective design restricted control over contextual variables during testing, such as neuromuscular fatigue, pain, or psychological readiness—factors known to affect performance in explosive tasks. Their unmeasured influence may have contributed to variability in some outcome measures, particularly eccentric RFD. Only intra-session reliability was assessed. Although this provides useful insight into short-term measurement consistency, the absence of inter-session analysis limits the understanding of the temporal stability of these variables. The absence of inter-session reliability assessment, electromyographic data, minimal detectable change values, and associations with clinical outcomes limits the interpretation of these metrics beyond short-term monitoring. Consequently, these results should not be interpreted as evidence of clinical sensitivity or prognostic validity. This is especially relevant for eccentric RFD, which showed high variability and may fluctuate across sessions. The CMJ protocol used a standardized, symmetrical setup (bilateral jumps with hands on hips) to maximize internal consistency. While this approach reduces technical variability, it may not reflect the dynamic, sport-specific movement patterns athletes encounter during return-to-play scenarios, thereby limiting ecological validity. Additionally, the study focused solely on eccentric-phase variables (EPF, EI, eccentric RFD). Although these are highly relevant to ACLR rehabilitation, omitting other performance indicators such as concentric force, jump height, or rate of force relaxation may have limited the scope of neuromuscular assessment.
Future studies should replicate reliability analyses using ecologically valid and sport-specific protocols, such as unilateral CMJs, drop jumps, or reactive landing tasks, which better simulate athletic conditions and reveal potential compensatory strategies. Expanding the range of performance variables to include concentric output, jump height, and relaxation dynamics could yield a more comprehensive profile of lower limb recovery after ACLR. Finally, to support RTS decision-making and longitudinal tracking, future research should explore the inter-session reliability and responsiveness of these metrics over time, particularly for those showing greater variability within a single session.
CONCLUSION
This study evaluated the intra-session reliability and intra-session variability of three eccentric kinetic variables—EPF, EI, and eccentric RFD—measured during bilateral CMJ in individuals six months after ACLR. The results demonstrated that EPF and EI are reliable within a single testing session supporting their use for short-term neuromuscular monitoring. In contrast, eccentric RFD showed greater trial-to-trial variability and lower reliability, particularly on the OP limb, warranting cautious interpretation and further investigation before clinical integration after ACLR.
Corresponding author
Florian Forelli
Haute-Ecole Arc Santé, HES-SO University of Applied Sciences and Arts Western, Switzerland Delémont, Switzerland
+41 32 930 16 54
Competing interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.