INTRODUCTION
Low back pain (LBP) is a debilitating injury for athletes, with an unclear pathway to return to sport (RTS).1 Experts classify pain lasting longer than 12 weeks as chronic low back pain (CLBP).2 CLBP is associated with disability and a low score on the World Health Organization Quality of Life Scale.3 One study measured the point prevalence of CLBP in university athletes to be 20.0% for volleyball, 15.6% for basketball, and 11.4% for football.4 Studies on athletes often focus on LBP rather than the subset of CLBP. Varying rates of LBP in athletes are reported in the literature, influenced by research methods and outcome measurement tools.5 The point prevalence of LBP in athletes ranges from 10% to 67%. One-year prevalence ranges from 17% to 94%, and lifetime prevalence ranges from 33% to 84%.5 Many athletes will face LBP at some point in their careers, and the pain often becomes chronic.4
While previous research estimates that 90% of low back pain cases have no specific cause,2 new research suggests muscular dysfunction may exist in those with CLBP.6 Due to the uncertain nature of LBP, a variety of treatments positively affect pain and disability in athletes.1 Although many interventions are helpful, it remains unknown which is the most effective and disagreement exists on a standard approach for RTS. A systematic review and meta-analysis on the treatment of LBP in athletes by Thornton et al. concludes that while many interventions have a positive effect on LBP, their effect on RTS remains unclear.1 A literature review on LBP in athletes by Mortazavi et al. emphasizes the lack of evidence regarding proper RTS timelines once treatment has concluded.7 As people with persistent LBP experience less improvement in pain and disability over 12 months compared to those with acute LBP,8 RTS treatments and protocols are likely complicated further when LBP becomes chronic. The complexity of returning to sport likely requires an approach that addresses the physical, psychological, and social demands of participating in athletic endeavors.9,10 This case report presents and applies a novel biopsychosocial framework, SPORT, to a young athlete with CLBP.
Biopsychosocial Model
The biopsychosocial (BPS) model is a holistic approach that combines physical, mental, and social components of health.11 Developed by George Engel, the framework considers multiple factors to understand the connection between mind and body in the context of medical care. A systematic review and meta-analysis by Kamper et al. analyzed the effect of BPS rehabilitation involving a physical component and one or both of a psychological component or a social or work component on adults with non-specific CLBP.12 Adults who adhered to a BPS rehabilitation program for CLBP experienced minorly increased long-term benefits in pain and disability compared to those who underwent usual care (care from a general practitioner or medical specialist) and physical treatments (heat, aerobics, strengthening, stretching, manual, and educational). Adults receiving BPS care had a greater chance of returning to work than those receiving physical treatment alone. Furthermore, adults following a BPS approach experienced similar outcomes to those who had surgical interventions with fewer adverse effects.12 While there is limited research on this approach in young athletes with CLBP, the positive outcomes observed in adults suggest BPS care could be beneficial to other populations.
Multiple authors have concluded that addressing BPS elements during sports rehabilitation can help prevent injuries and promote recovery.9,10,13 However, limited knowledge of practical guidelines and application of the BPS approach to treat LBP presents a challenge for practitioners.14 Models by Wiese-Bjornstal, Brewer, Williams, and Anderson have played a key role in integrating psychosocial concepts into athletic recovery.15 However, they primarily demonstrate the interplay among psychological, social, and physical factors rather than providing specific guidelines and protocols for clinical application.
The framework proposed here is named “SPORT”: Systematic Progressive Overload Rehabilitation Training, and it is applied to rehabilitation of the spine in a young athlete. The SPORT framework includes principles in three categories: Biomechanical, Psychological, and Social. The framework is unique due to its originality, target population, actionable design, multifactorial approach, and real-world application. Its ingenuity lies in the combination of evidence-based principles. These principles form a framework designed to treat CLBP in young athletes, which is explored in this case report. The 18 SPORT principles are listed and defined in the tables below.
Athletes recovering from CLBP require a comprehensive approach that considers all aspects of the mind and body. This case report serves to introduce a novel BPS framework that attempts to bridge the gap between literature and practical application. The SPORT framework could provide templates and takeaways for clinicians, distinguishing it from less applied models.
CASE DESCRIPTION
Subject History
The subject provided informed consent for the use of case data in publication. The subject of this case report was an 18-year-old male who participated in high-level soccer, kicked for his high school football team, and enjoyed competitive powerlifting. He had years of intensive training in soccer and football and was an elite athlete. He notably achieved top regional recognition in soccer and was rated a 4.5-star kicker for recruitment purposes. He also achieved a back squat of 345 pounds (lb) × 5 repetitions (reps) and a deadlift of 445 lb × 5 reps in his first year of powerlifting. He experienced social and internal pressure to perform in these sports, as this was his last year in high school. The individual’s main goal was to compete in powerlifting nationals.
Injury History
This subject’s low back pain began in September 2023, during his junior year of football. Clinicians (including a physical therapist, an orthopedic surgeon, an orthopedic specialist, an athletic trainer, a spine surgeon, and a chiropractor) conjectured that the pain was due to kicking. As the season concluded, the athlete felt better. He started participating in powerlifting in March 2024, which had little to no impact on his CLBP. In August 2024, his football and soccer season began and his pain returned. Once again, the subject noticed pain related to kicking. The pain worsened throughout the season, forcing him to miss games and practices. He also stopped resistance training, as the pain began to affect his ability to squat and deadlift even at low loads.
As the season ended in November 2024, the pain did not subside. The subject’s low back symptoms worsened, interfering with Activities of Daily Living (ADL) such as sitting, bending, and dressing. The subject reported low back pain that began upon waking and persisted throughout the day, worsening with spinal flexion and various movements. As of January 2025, the subject had been experiencing constant pain. The length of the injury meant his low back pain was now classified as chronic.2 He was unable to run for a few minutes in a soccer game without severe, debilitating pain. He stopped sports and powerlifting training completely and failed to participate in school or ADL without severe limitations. Due to his previous identity being rooted in elite physical activity, this took a significant psychological toll on the subject. His baseline discomfort and pain associated with movements caused high levels of fear during any squat, deadlift, sport, or physical activity. His dream had regressed from winning powerlifting nationals to being able to function and participate in physical activities. He consistently reiterated the phrase, “I just want to be healthy again.”
Medical Findings
Lumbar spine radiographs revealed essentially normal findings. Normal lumbar lordosis was maintained, no significant spondylolisthesis was seen, and vertebral body heights and intervertebral disc space heights were maintained. No concerning osseous lesions were seen. A MRI of the lumbar spine showed normal vertebral body heights, bone marrow signal, and alignment, with a normally positioned conus medullaris and unremarkable nerve roots. There were mild degenerative changes with minimal facet arthrosis and disc bulging causing slight ventral canal flattening with minimal narrowing. Overall, findings were consistent with mild age-related degeneration without significant spinal stenosis or nerve root compression.
From September 2024 to January 2025, the subject consulted with and received treatment from a physical therapist, an orthopedic surgeon, an orthopedic specialist, an athletic trainer, a spine surgeon, and a chiropractor. The providers did not agree on the diagnosis related to his pain and disability. Posterior pelvic tilt, arthritis, “tight” muscles surrounding the region, and the left side of the subject’s low back being “denser, thicker, and larger” than the right side were all reported by different clinicians as possible findings.
Pre-Case Interventions
The subject received various forms of interventions and instruction over a five-month period from the aforementioned clinicians. (Table 4).
Despite following all listed interventions and recommendations, the subject experienced little to no improvement in pain, disability, and was unable to return to sports. These treatments may not have worked for this subject for many reasons: a lack of progression,43 emphasis on passive treatment,16 repeated messages of fear and avoidance,36 failure to train movements specific to the athlete’s goals,24 and lack of consideration of the body and mind as one system.12
Treatment Plan used during the Case
Subsequent rehabilitation was guided by the author who has experience working with youth and collegiate powerlifting athletes in strength and conditioning and rehabilitation settings. The subject was struggling with CLBP and the associated psychological aspects of limited physical ability, alongside alarming messages from clinicians. He reported having difficulty consistently performing the tasks prescribed to him due to their complexity and volume, citing that he did not have complete confidence in his clinicians. The biomechanically centered pre-case interventions had made little to no difference. The subject’s goals were to return to everyday living and sport participation.
Due to these factors, a comprehensive BPS approach focused on a RTS was implemented. The tracked outcomes were strength, sport participation, and reported pain and function. In this case, rehabilitation was split into three phases. In the first phase (weeks 1-3), daily movement was prioritized to increase the subject’s activity level and movement confidence. The subject performed daily bodyweight squats, bodyweight Romanian deadlifts (RDL), and several daily short walks (5-10 minutes each). The movements were enjoyable, scalable and easily incorporated in his life. Further, they replicated the demands of his sports, albeit at a low level. In the second phase (weeks 4-17), a return to lifting and basic sports was prioritized. The subject performed two progressive lower-body resistance training sessions per week, while also continuing his daily home exercises from phase one.18 In the third post-case phase (weeks 18-25), performance and sustained improvement were prioritized to return the athlete to full strength and sport abilities. The subject continued to perform two lower-body resistance training sessions per week. The training increased in intensity. It is important to note that the subject’s symptoms dictated the speed and phases of the BPS intervention. For example, phase two began in Week 4 because that was when the subject could first perform a bodyweight squat reliably and comfortably, providing information on the proper timeline to begin loading that specific movement pattern. The warm-up protocol for each resistance training session consisted of a short form of light cardio to increase body temperature44 and movement-specific warm-ups that progressed to prescribed loads.45 Detailed information regarding interventions in phase two (weeks 4-17) is presented in Tables 5-7. The following is an explanation of the notation used in the tables:
Set × repetition @ load format used throughout (e.g., “3×5 @ 95” represents 3 sets of 5 repetitions at 95 pounds). All loads are in pounds. “x” indicates an exercise not performed that week. “→” indicates same load, sets, and repetitions maintained for the following week(s). yd: yards. In Table 7 “+” indicates the amount of weight added since the introduction of the movement.
Application of SPORT Biomechanical Principles
Active Exercise The training program began with a daily protocol consisting of several short walks, 10-20 reps of bodyweight squats, and 10-20 reps of Romanian deadlifts (RDL). After Week 3, the treatment continued to be active, focusing on resistance training. The process consisted of little to no passive interventions. These exercises were chosen because they were active,16 aligned with the subject’s goals,24 and yielded positive feedback regarding pain relief.30
Posterior Resistance Training The subject performed posterior resistance training, including RDL, single leg RDL, lying hamstring curls, and trap bar deadlifts. These movements progressed throughout the program, increasing in load and exercise complexity.17 The posterior movements were selected to allow the subject to train his posterior chain on load-limiting movements at a higher intensity, far before the inclusion of sumo deadlifts.
Continuing Effective Rehabilitation The subject continued to perform the initial daily interventions (walking, RDL, bodyweight squat, deep breathing) throughout all phases of rehabilitation. He also performed these exercises as a warm-up to lower-body resistance training, providing the athlete with direct feedback on his low back symptoms before each session. This protocol was implemented to continue treatment that previously had a positive effect18 and to keep the subject active.16 In addition, the continuation of these movements provided active exercises for the athlete to fall back on in case of setbacks and flare-ups.
Sleep Improvement The subject was frequently encouraged to improve his sleep, as a focus on perfect sleep numbers could have increased psychological stress due to extensive academic involvement and various commitments alongside the BPS plan. Sleep improvement was encouraged because of the negative impact that poor sleep habits can have on pain perception and rehabilitation,19 particularly on a high school athlete aiming to avoid reinjury.20
Avoiding Dehydration Throughout rehabilitation, the subject consumed approximately 2.9 L (100 oz) of water daily, aligning with hydration guidelines to support metabolic function and fluid balance.46 Proper hydration can improve the athlete’s perception of pain,21 potentially allowing him to engage in physical activity more comfortably and consistently.30
Increasing Protein Intake Due to the inverse correlation between CLBP and adherence to a high protein diet,22 the subject, who weighed 79 kilograms (kg), consumed a high-protein diet of 150-200 g (roughly 2.2 g/kg/day) of protein per day.47
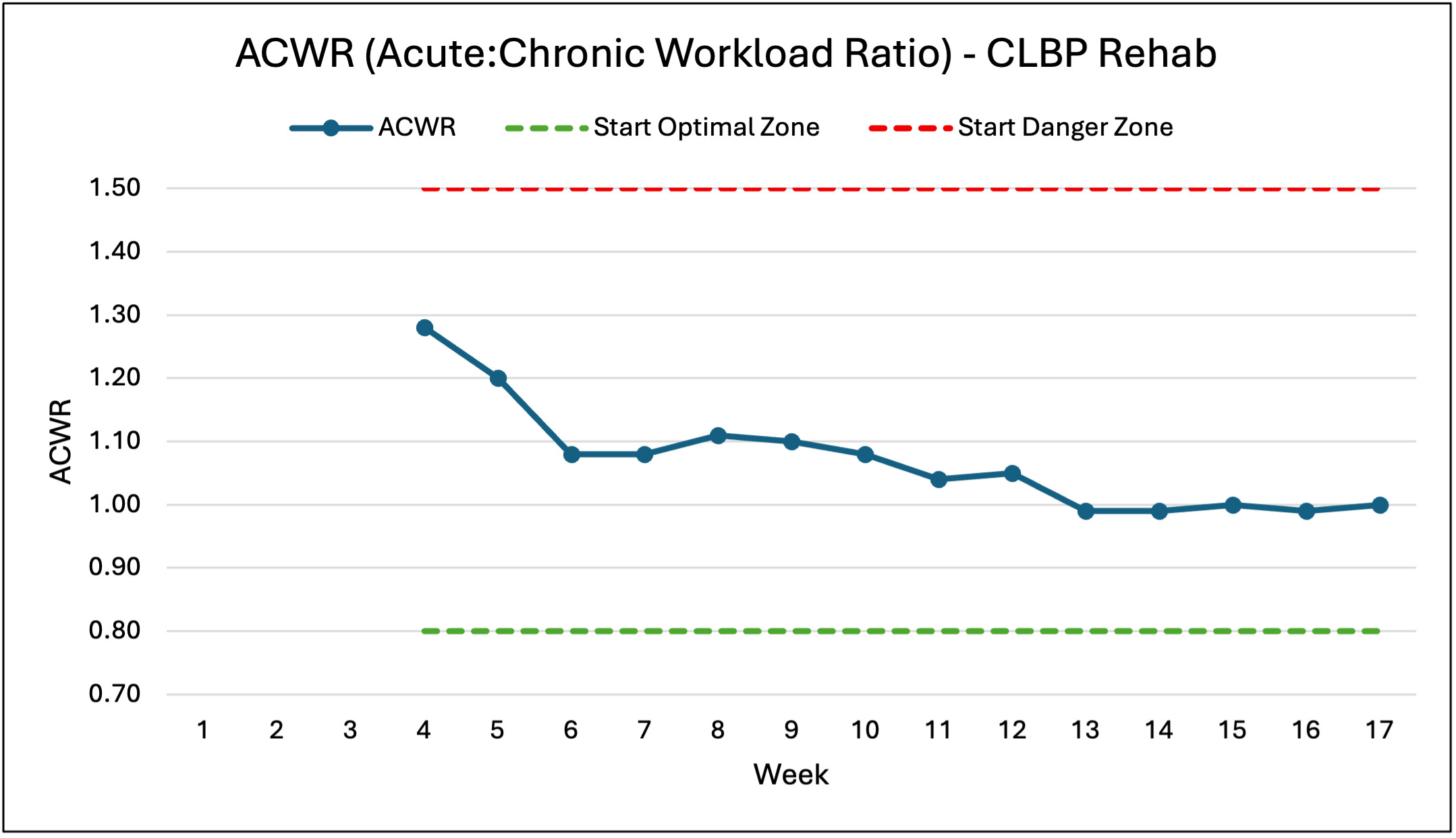
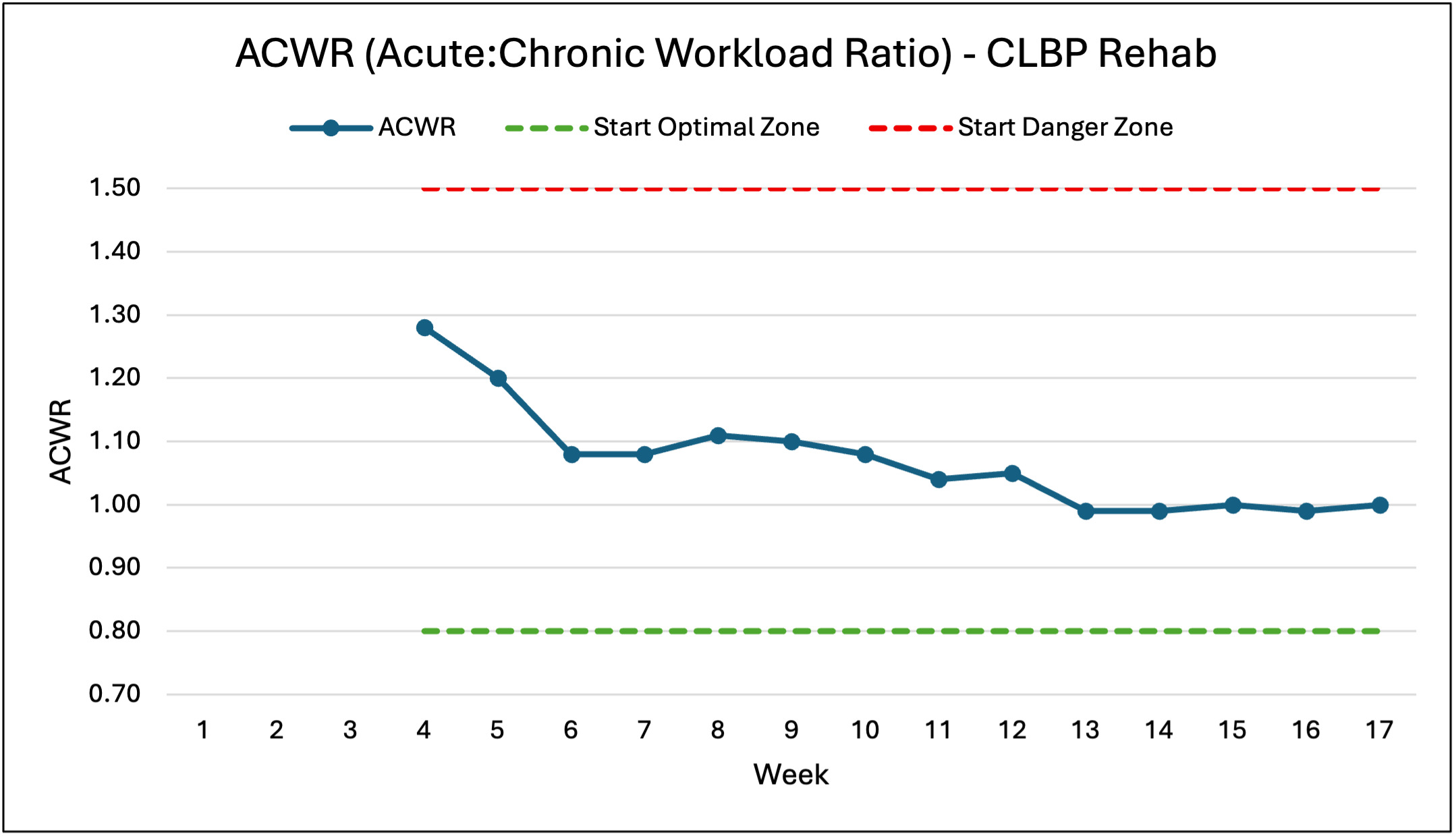
Safe Progressive Loading For sports activities outside of resistance training, the subject followed a more general approach of gradually and comfortably building up over time rather than a specific progression scheme. This protocol was implemented to allow for more athlete decision-making41 and to reduce the fear induced by strict time limits on play.36 The squat and deadlift load progression was chosen to stay within the Acute Chronic Workload Ratio (ACWR). The previous week had to be comfortable as reported by the subject, and the new week targeted a maximum increase of 15% in a specific variable.23 Because the set-and-rep scheme remained consistent, the programmed load remained within the 15% target. Outliers in these weekly increases occurred because the subject started at roughly 20% of his previous one-rep max, as the 15% target is a protocol for a healthy athlete rather than one rebuilding from the beginning. The accessories followed a similar progression plan. Introduced at a comfortable load, these exercises needed to be pain-free and have a Rate of Perceived Exertion (RPE) of 7-8 or lower to increase by no more than 5-10 lb per week.
The rationale behind this process was to potentially regain strength and neurological adaptations through lighter loads24,25 and help the subject regain confidence through previously painful and feared movements.38 By adhering to objective targets for safe and appropriate progression, the lower-body exercises remained within the optimal ACWR range (0.8-1.3).23 Given the relatively short timeline, ACWR was calculated by comparing the current week to the average of the preceding three weeks. The graph displays the ACWR of all lower-body exercises that affected the subject’s low back, calculated using total load (sets x reps x weight).
Goal-Specific Exercise As stated, the subject desired a return to high-level powerlifting and sports. Closely aligned with the desired goals, the first exercises introduced were bodyweight squats and bodyweight RDL. Cossack squats replicate movement patterns similar to lateral motion in sports, and cable chops have a movement pattern closely related to kicking in soccer and football. These multi-directional exercises were also chosen to better replicate the loads of daily living. Because the evidence suggests that variations of active exercises elicit similar long-term positive results in CLBP,16 it follows to choose exercises that closely align with the subject’s desired goals and outcomes. Applying this concept to sports outside of powerlifting would involve using regressions of foundational sports movements. For example, a soccer player aiming to RTS could begin rehabilitation with low-effort passing or juggling drills, while a basketball player might start with gentle dribbling exercises. This method also provides a psychological advantage for athletes, as they gain the opportunity to do what they love in a conservative, regressed and pain-free manner early in the BPS treatment.
Low-intensity Exercise Rebuilding the individual’s one-repetition maximum (1RM) on the squat and deadlift during rehabilitation required unique interventions. Maximal strength requires a high level of force production. As fatigue accumulates, the ability to produce force decreases, meaning that force output is generally highest during the earlier reps of a set taken to failure. Once the subject reached week 10 of rehabilitation, his strength had returned to nearly 80% of his previous 1RM. At this point in rehabilitation, his lower body sets were classified as challenging working sets. The program incorporated low RPE backoff sets at this stage. The progression of the back squat is an example. In week 10, there were three sets of five reps with 285 lb. Then, in week 11, there was one set of five reps with 305 lb and two sets of five reps with 275 lb. The progression focused on the higher RPE top sets, with little progression on backoff sets. Including low-intensity sets minimized weekly fatigue and training loads while maximizing strength gains,25 helping the subject return to an elite level. While this principle is centralized around strength training, it can be utilized for other sports. Athletes recovering from an injury can benefit from low intensity work specific to the skill they are trying to relearn.24 In this case, the strategy was employed due to the subject’s previous high strength levels, which allowed for neurological adaptations to “relearn” the movement pattern.
Application of Psychological Principles
Goal Setting The subject set several goals for himself throughout rehabilitation. One of the most impactful goals was trying to increase his bench press. The subject intensely trained his upper-body three times per week in addition to the lower body program. To reduce the stress on the subject’s low back in the initial phase, the program included adjustments such as feet-up benching and an emphasis on machine training rather than free weights. Focusing on achieving this goal resulted in significant improvement from a 190 lb three-rep max bench press to a 220 lb three-rep max bench press over the 17 weeks. By setting a goal unrelated to his injury, the athlete could still feel a sense of high-level performance, purpose, and achievement.26
Avoiding Pain Tracking Pain scale measurements were intentionally omitted during the BPS process. Instead, pain was assessed weekly regarding movements and functions to inform decisions. In the initial consultation, the subject reported that bodyweight squats, bodyweight RDL, and walking produced positive feedback in his low back. These exercises were chosen and prescribed within comfortable ranges of motion. Another example of using pain to guide decision making occurred when the trap bar deadlift caused discomfort and post-session pain, prompting a switch to a different exercise. When the individual reported higher feelings of pain following a session, subsequent workouts were adjusted by slowing down the rate of loading. Weekly reports of discomfort helped identify trends and account for daily fluctuations in pain influenced by factors such as sleep, stress, and changes in activity. Rather than using pain as an obsessive and potentially harmful metric,27 this approach used it as a tool to uncover patterns that drove decisions and interventions.28
Improving Adherence Due to complaints about exercises, pain, program length, and the perceived “boring” nature of the subject’s previous treatment plans, creating a program that he could easily follow was prioritized for better outcomes and recovery.29 The first three weeks of daily training were brief, with each session lasting 10-15 minutes. Squats, deadlifts, and minimal changes created a simple resistance training plan. The subject performed exercises comfortably, focusing on those for which he reported positive feedback.30 He provided input regarding exercise selection to increase his enjoyment of performing the tasks.30 Encouraging the subject to walk daily while watching television programs and perform bodyweight exercises each morning helped easily integrate the program into his daily life.30
Stress Management The subject reported feeling stressed from academic and athletic pressure. Multiple techniques were utilized to help manage his stress levels. In the first few weeks of recovery, the athlete performed frequent deep breathing for a few minutes.48 He also journaled his workouts to allow for review and reflection.49 As discussed previously, he focused on reducing stress through increased hydration,50 adequate protein intake,51 and sufficient sleep.52 The program mainly consisted of resistance training, which has been shown to have anxiolytic effects.53
Pain Education Reiterating messages of belief and optimism for the outlook of his injury was done regularly. At the initial meeting to discuss his pain, the subject was informed of research-based realities concerning low back pain.33,54 Specifically, he learned how graded spine movement and loading are safe and build structural resilience, as well as how pain flare-ups are more closely related to changes in activity, stress, and mood rather than structural damage. Pain education was particularly beneficial to the rehabilitation process32,33 and was utilized as a tool to increase optimism in the subject.34
Building Confidence The subject was repeatedly exposed to messages of fear and avoidance by several clinicians. The subject developed fearful beliefs about athletic endeavors, specifically surrounding participating in gym class sports, squatting, and deadlifting. His low confidence put him at risk for worse rehabilitation outcomes and higher risks of reinjury.37 Often performed gradually, in vivo exposure is the method of directly facing feared activities.55 The early introduction of squats, deadlifts, and sports at low loads was a key application of this approach. The subject progressed through these activities over time rather than waiting for his pain to subside before returning to them. He experienced less fear that these activities would cause him pain since he engaged with them comfortably and regularly, helping to increase his confidence and reduce his fear of reinjury.
Application of Social Principles
Teamwork The subject and rehabilitation coach worked closely together through weekly check-ins, daily assistance, and feedback on exercise videos. The coach frequently provided emotional support,39 reiterating positive messages34 and pain education concepts.32 Involving the patient can strengthen the connection between the subject and coach,39 further improving treatment adherence and LBP physical function.40
Adaptability The program’s design was subject to modification, as the athlete was involved in exercise selection and weekly training load decisions. The subject was able to choose the days on which he performed lower-body resistance training, aligning with when he felt most physically and mentally prepared. This protocol was implemented to improve adherence,30 increase patient-centered care,41 and promote engagement in active exercise,16 while reducing unpleasant experiences with exercise.30
Accountability The subject updated a Google sheet as he completed each workout, including notes on pain, difficulty, desired changes, RPE, and load. Holding the athlete accountable through these measures provided useful insights for decision-making,28 a platform for the athlete to lower stress,49 and a low-effort meaningful data collection system.42
OUTCOMES
To evaluate the effectiveness of the SPORT framework on treating CLBP in this young athlete, objective and subjective measures were tracked throughout the study. The objective measures were strength in powerlifting movements and participation in recreational sports. Subjective measures were tracked weekly through self-reported pain and function. The table below summarizes the baseline, interim, and final outcomes reported by the subject throughout the rehabilitation.
Post-Case Outcomes
The individual continued strength training under the same coach’s direction for seven more weeks after completing the 17-week case treatment. Afterward, the subject continued seeing improvement in strength, activity level, and daily living, despite a temporary setback. A flare-up occurred in week three of the post-case training when the subject’s load on paused sumo deadlifts increased by more than 20%. During this week, the subject made the independent decision to play intense soccer for a few hours and to participate in recreational trampoline activities, where his peers encouraged him to push beyond his current limits. He began to feel the LBP discomfort that he had previously felt. After the minor flare-up subsided, the subject performed an hour of intense soccer on the same day as his lower-body strength workout with no physical discomfort during or after. He also experienced little to no pain during daily life. At the conclusion of the post-case training, the subject was able to perform a 435 lb back squat and a 465 lb sumo deadlift with no discomfort, far surpassing his pre-injury strength. The subject continues to pursue powerlifting goals and play soccer recreationally.
DISCUSSION
The SPORT framework was beneficial for alleviating CLBP and achieving a RTS for the subject. Potential reasons for this athlete’s success include exercise progression, active treatments, optimistic messaging, goal-aligned activities, and a holistic BPS approach. Further, the subject reported that education of misconceptions about LBP was helpful, such as 1) LBP will become persistent and deteriorate later in life, and 2) pain related to exercise and movement is always a warning that harm is being done to the spine.33 The remainder of this discussion covers the setback that the subject experienced, the SPORT framework, and the implications and limitations of this study.
Setback
A flare-up occurred in Week 3 of the post-case training period due to a spike in loading, reckless decision-making, and increased stress. The situation provided an opportunity to educate the subject on pain management. During the increased discomfort and stress, the subject returned to the basics of the SPORT framework. He focused on bodyweight exercises, walking, and having an attitude of optimism and belief. Young athletes can make poor decisions about exercise duration and intensity. It is paramount to reframe the scenario rather than blaming the subject. This can be done by focusing on movements that can still be performed during the flare-up and reflecting on progress made. The resolution of the flare-up revealed two key insights. First, the SPORT framework served as a toolbox to manage injuries over the short and long term. Second, for this athlete, load management needed to be expanded to include external factors such as stress, nutrition, sleep, and recreational activities,56 in addition to exercise and sport-specific load.
Framework
This athlete benefitted from a holistic approach to recovery due to unique biomechanical, psychological, and social challenges. Unlike other models that primarily focus on demonstrating interactions between BPS factors, the proposed SPORT framework offers a template that integrates actionable steps for exercise intensity, exercise selection, stress management, pain education, and patient-centered care. Early usage of goal-specific in vivo exposure activity had a positive impact on the athlete, who not only reaped biomechanical benefits (pain free loaded squats and deadlifts), but also experienced a complete restoration of confidence in his body. Utilizing the 15% weekly target and ACWR principles provides a recommendation for loading guidelines23 and resulted in pain-free progression for this athlete. Finally, this case provides an example of the utilization of the SPORT framework, demonstrating the 17-week recovery and return to sport of an elite 18-year-old athlete.
Implications
Because previous interventions such as passive treatment and fear-based messaging failed to treat the subject, practitioners should consider prescribing active, progressive exercise reinforced by positive communication in similar cases. Applying the graded approach to strength training resulted in pain-free function across various activities in this athlete, suggesting that progressive spine loading could be further researched as a tool for young athletes experiencing CLBP. The framework incorporates principles that are helpful for young athletes related to sleep, protein, and hydration. If replicated, additional nutritional protocol specific to the athlete’s needs could be provided by a Registered Dietician Nutritionist. In contrast to the complex and lengthy recommendations previously given to the subject, a plan based on collaboration, adaptability, simplicity, and enjoyment resulted in favorable outcomes and near-perfect adherence.
Limitations
This single case report provides an in-depth examination of one individual, which limits its generalizability to broader populations. The subject’s positive response cannot be considered an effect of the treatment (due to case report methodology) and cannot be generalized to athletes with varying sports categories, abilities, injury types, or ages. The subject was a disciplined athlete with extensive experience in three sports. It remains unclear whether this BPS framework is suitable for athletes with acute low back pain or other chronic conditions beyond the spine, and whether it could be adapted for non-athletes seeking to resume daily activities. The absence of a standardized patient-reported outcome assessment is a limitation of this study and would be recommended in future research. Future studies should compare this framework to other types of treatment for chronic low back pain in young athletes, ideally on a larger scale with diverse populations.
CONCLUSION
This case report indicates that an applied biopsychosocial framework (SPORT) resulted in reductions in pain and a full return to sport in a young athlete suffering from chronic low back pain. The post-case seven-week outcomes included a 435 lb squat, 465 lb deadlift, continued sports participation, sustained improvements in pain and function, and strategies to manage flare-ups. The case introduces SPORT, a biopsychosocial framework for CLBP that could be applied to young athletes desiring a RTS.
Conflict of Interest Statement
The author served as the subject’s strength and rehabilitation coach. He is also a friend of the subject. No financial conflicts of interest are declared.