Introduction
Hamstring injuries may be among the most common injuries to thigh muscles in young, active individuals. Along with the biceps femoris, these muscles work together to extend the hip and flex the knee. These injuries typically occur when the muscle undergoes an eccentric contraction during dynamic movements such as sprinting or kicking.1–4 The late portion of the swing phase of sprinting appears to be the most vulnerable position for the muscles, as the hamstrings produce a violent eccentric contraction to decelerate the forward-moving tibia.5–8 The ability to contract so aggressively may be because, like the biceps femoris, the semimembranosus muscle has large pennation angles, suggesting that it may have more force-generating fibers within each muscle fascicle.9–11
Anatomy of the Medial Hamstring Tendons
The proximal medial hamstrings consist of both the semitendinosus and semimembranosus, which both originate at the posterior, lateral side of the ischial tuberosity of the pelvis.12,13 The distal attachment of the medial hamstrings is as a conjoined tendon with the gracilis, as they form the pes anserine and attach to the medial tibial flare. The semimembranosus has up to five different extensions, which include 1) the direct portion, which is the main insertion, 2) the capsular portion, 3) an extension that joins the oblique popliteal ligament, 4) the anterior portion, and 5) the distal portion.14 The semitendinosus is medial and more superficial, while the semimembranosus is deep to the semitendinosus. Interestingly, the semitendinosus muscle proximally has a connecting ridge located in the proximal quarter of the muscle belly. This ridge separates the muscle into two parts, each innervated by a different sciatic nerve branch. It is the only hamstring muscle with fibers directly reaching the ischial tuberosity, as all the others have tendon-to-bone attachments. It is at the location of the proximal attachment of the semitendinosus and biceps femoris that form a conjoint tendon to attach to the ischial tuberosity.
The Role of MSKUS in Tendon and Muscle Evaluation
Advantages
- Real-Time Imaging: MSKUS allows dynamic evaluation of the medial hamstring tendon while the knee can be manipulated through the available range of motion.
-
High-Resolution Visualization: MSKUS provides detailed images of the medial hamstring tendon and its proximal and distal attachments at the ischial tuberosity and medial tibial flare.
-
Accuracy: MSKUS has been proven to be both a valid and reliable method for examining hamstring architectural properties at rest.15–19
- Accessibility and Cost-Effectiveness: MSKUS is portable, widely available, and less expensive than magnetic resonance imaging (MRI).
Limitations
- Operator Dependency: MSKUS requires skill and experience for accurate interpretation of findings. The ability to sonograph tendons and their respective muscles is largely influenced by the operator and by the availability and technical considerations of state-of-the-art equipment.
- Depth Limitations: Visualization is usually not a problem with MSKUS; however, in some individuals who are older and obese, visualization may be less than ideal due to muscular fatty degeneration and increased soft tissue thickness due to subcutaneous fat.20,21
- Artifacts and Shadows: Bone and calcifications may create image artifacts, requiring adjustments in probe positioning and frequency.
Sonographic Technique for Evaluating the Medial Hamstrings
Equipment Setup
- Probe Type: Because of the depth of the medial hamstring tendons and muscles, a standard high-frequency, linear array probe can usually be utilized. However, in some individuals who have more adipose tissue or larger muscle mass, a lower-frequency curvilinear probe may be required to achieve depth.20–23 This is especially true at the ischial tuberosity.
-
Patient Position: The patient is in the prone position with the feet over the edge of the table.
-
Dynamic Assessment: A passive or active movement of knee flexion and extension can be applied during ultrasound assessment to evaluate for medial hamstring contractile and excursion properties.
Examination Protocol
Normal Sonographic Appearance
The starting point for examining the proximal hamstring tendon and muscle is at the ischial tuberosity. The ischial tuberosity can almost always be palpated, providing the examiner with a perfect starting point for their scan. The proximal hamstring can be scanned in both the short axis (SAX) and long axis (LAX). In the SAX view, the examination should be proximally just distal to the gluteal fold in the proximal 1/3 of the back of the thigh. In this position, the biceps femoris muscle will be seen laterally, and the semitendinosus muscle, the semimembranosus membrane, and the semimembranosus tendon can be seen. As the probe is moved distally, still in SAX view, the biceps will widen and appear triangular, while the semitendinosus will also enlarge. These tendons will appear hyperechoic. In the LAX view, one can visualize the hyperechoic semitendinosus muscle and its hypoechoic raphe.
As one moves towards the mid-thigh in the SAX, the semitendinosus will start to decrease in size, while the semimembranosus will increase in size. In the distal thigh, the semitendinosus turns to more of an oval shape and is located slightly laterally and superficial to the semimembranosus muscle.
Pathologic Findings in Medial Hamstring Tendon and Muscle Injury
-
Disruption of fibrillar pattern in partial tears and ruptures. Proximally, it is important to determine whether the injury is a free-tendon injury or a purely myotendinous injury.24 In children in particular, the apophyseal region of the ischial tuberosity is the weakest part of the hamstring bone-tendon-muscle unit.25
-
Thickening of the distal tendon and hypoechoic appearance in those with medial hamstring tendinopathy.26
-
Sonopalpation can be used in symptomatic patients to see if pain can be reproduced.27,28
-
An avulsed fragment of the ischial tuberosity and retracted tendon.29
-
Ruptured tendons will demonstrate poorly defined hyperechoic or heterogeneous areas of tendon tissue without muscular architectural alterations. If acute, these injuries will also include an anechoic hematoma. These ruptures can be confirmed by an active dynamic muscle contraction.14
-
Associated effusion.
-
Calcifications due to deposition of calcium hydroxyapatite crystals within the tendon can be seen in the proximal hamstrings. Like other calcifications, these are most painful during the resorptive phase of healing.22,30
Clinical Implications for Rehabilitation Providers
MSKUS provides real-time feedback for rehabilitation professionals, facilitating early diagnosis and intervention. Key applications include:
-
Early Detection of Injury / Accurate Injury Grading: MSKUS can quickly differentiate between a tendinopathy versus a strain, or more severe tendon rupture or muscle tear, to help guide treatment planning.
-
Dynamic Functional Testing: Rehabilitation professionals can use MSKUS during physical therapy sessions to monitor recovery and assess tendon and muscle function dynamically. Serial MSKUS imaging aids in assessing muscle healing and remodeling, helping determine readiness for rehabilitation progression.
- Guided Interventions: MSKUS imaging assists in dry needling and precision-guided injections, such as corticosteroids for inflammation.
- Patient Education: Real-time MSKUS imaging serves as a visual aid to explain the nature of the injury and set realistic expectations for recovery.
Limitations and Challenges
Despite its advantages, MSKUS cannot entirely replace MRI for complex cases, especially when examining the origin at the ischial tuberosity.31 Additionally, the expertise required for optimal imaging techniques limits its immediate adoption across all rehabilitation settings.
Conclusion
In summary, diagnostic MSKUS is a valuable, non-invasive tool for evaluating medial hamstring tendon and muscle pathology, offering real-time, high-resolution, dynamic imaging that can enhance diagnostic accuracy, guide clinical decision-making, and support patient education throughout rehabilitation. When integrated with a thorough history and physical examination, MSKUS can help differentiate tendinopathy, strain, and rupture, monitor healing over time, and inform progression to function and sport. Although operator dependence and depth-related challenges limit its use in some patients, and MRI remains important for complex proximal cases, ongoing training and wider access to high-quality equipment will continue to expand the role of MSKUS in evidence-informed hamstring injury management.
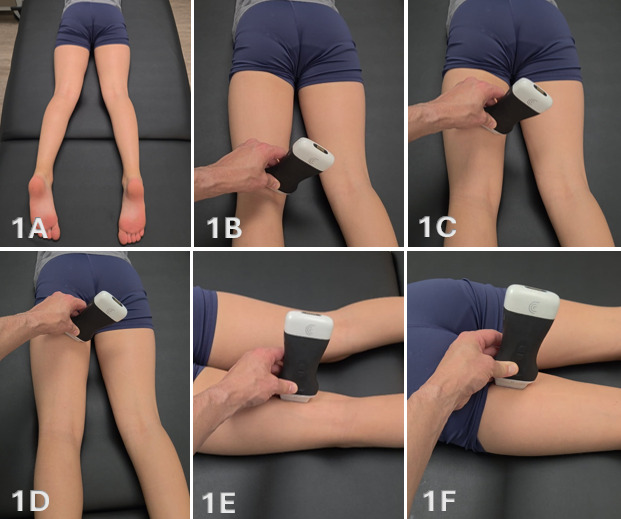
Figure 1A: Patient Positioning
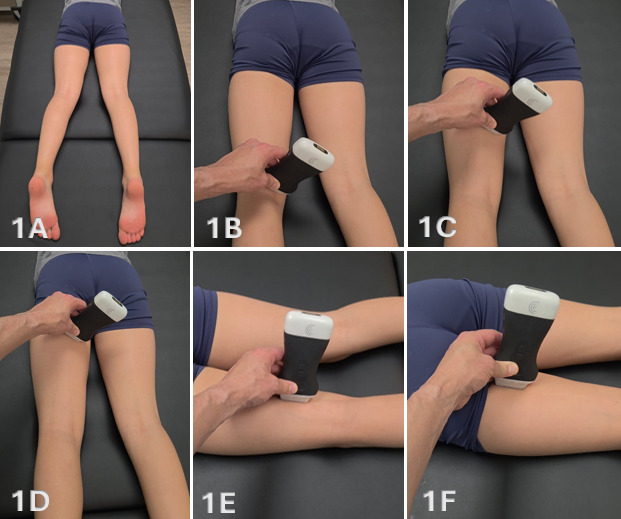
The patient is positioned prone with the feet hanging slightly over the edge of the examination table to allow passive tension across the hamstring musculature. The knee may be placed in slight flexion to reduce passive tension if needed. Imaging is typically performed at rest; however, dynamic knee flexion may be utilized to improve visualization of muscle contraction, excursion, and fiber organization. Side-lying positioning may also be used as an alternative depending on patient comfort and examiner preference.
Figures 1B-1D: Transducer Placement for Medial Hamstrings in SAX
For short-axis imaging, a high-frequency linear transducer is placed transversely at the posterior medial knee, just proximal to the joint line. This location serves as a reliable anatomical starting point for identifying the medial hamstring musculature. The semimembranosus is visualized as a deeper, larger, and more triangular structure, while the semitendinosus is positioned superficial and slightly medial with a smaller and more rounded morphology. The transducer is then translated proximally along the posterior medial thigh while maintaining a transverse orientation. Medial-to-lateral sweeping and proximal progression should be performed to evaluate muscle size, organization, and continuity.
Figures 1E-1F: Transducer Placement for Medial Hamstrings in LAX
For long-axis imaging, the transducer is rotated 90 degrees with the marker oriented proximally and aligned parallel to the muscle fibers. In this orientation, the semitendinosus is typically assessed distally initially and demonstrates a linear fibrillar architecture and may exhibit a characteristic internal fascial band. The semimembranosus appears deeper with a more complex fiber orientation as it transitions proximally. From the distal assessment, the transducer is moved to a proximal position to assess the two medial hamstrings. Subtle heel-toe angulation is required to maintain perpendicular insonation and minimize anisotropy. Long-axis imaging is used to confirm fiber continuity and evaluate the myotendinous junction.
Normal Medial Hamstrings in SAX:
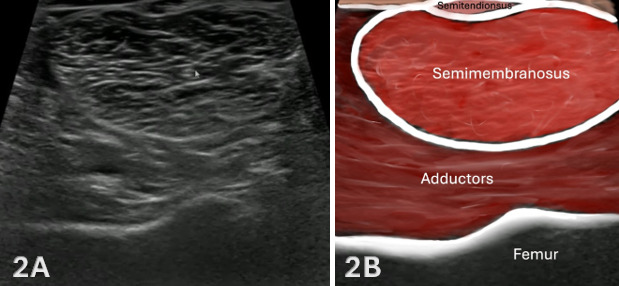
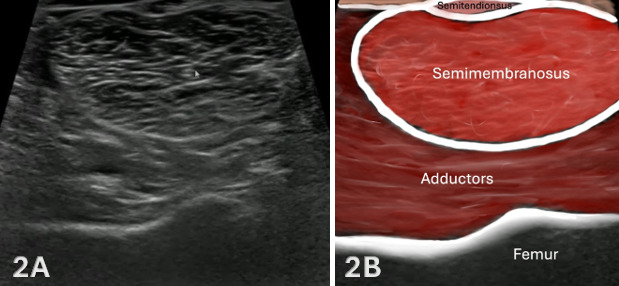
Figures 2A and 2B: Normal Distal, Medial Hamstrings in SAX
Evaluation of the medial hamstring musculature is initiated distally at the level of the posterior knee in short-axis (SAX), where the semimembranosus and semitendinosus can be reliably identified, see Figure 1B for transducer placement. In this region, the semimembranosus appears as a larger, deeper, and more triangular structure, while the semitendinosus is positioned superficial and slightly medial, demonstrating a smaller and more rounded morphology. This location provides a consistent and reproducible anatomical starting point for orientation.
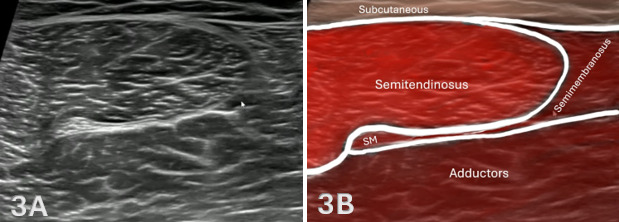
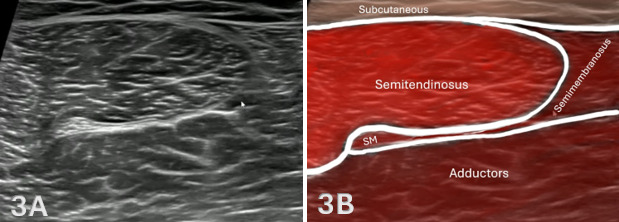
Figures 3A and 3B: Normal Mid-Thigh, Medial Hamstrings in SAX
As the transducer is advanced proximally, as shown in Figure 1C above, the semitendinosus demonstrates a progressive increase in cross-sectional area and may exhibit a characteristic internal fascial band, producing a striated or “venetian blind” appearance. In contrast, the semimembranosus follows an inverse pattern, appearing larger distally and gradually decreasing in size as it courses proximally. The muscle develops a more complex contour, often assuming a curved or comma-shaped configuration before transitioning into a deeper tendon via an aponeurotic extension.
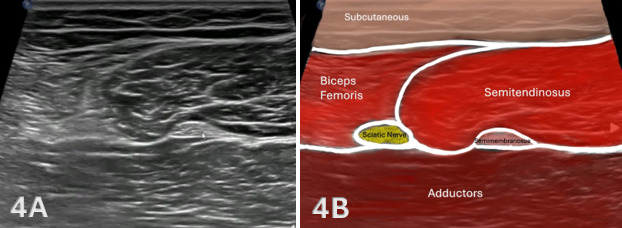
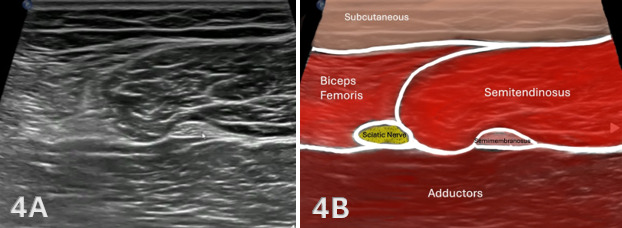
Figures 4A and 4B: Normal Proximal, Medial Hamstrings in SAX
Finally, the transducer is advanced proximally, as shown in Figure 1D above, and the semitendinosus demonstrates a progressive increase in cross-sectional area and the semimembranosus reduces into its proximal tendon. This proximal view allows the sciatic nerve to be visualized along with the biceps femoris to be viewed as well. Throughout the scan, the semimembranosus remains deep to the semitendinosus, and subtle transducer angulation is required to maintain perpendicular insonation and minimize anisotropy. Dynamic knee flexion may be utilized to improve visualization of muscle fiber organization and to assist in differentiating adjacent structures. This distal-to-proximal scanning approach allows for systematic evaluation of the medial hamstring muscle bellies and myotendinous junctions, facilitating identification of architectural disruption, focal hypoechogenicity, or other sonographic features consistent with muscle injury.
Normal Medial Hamstrings in LAX:
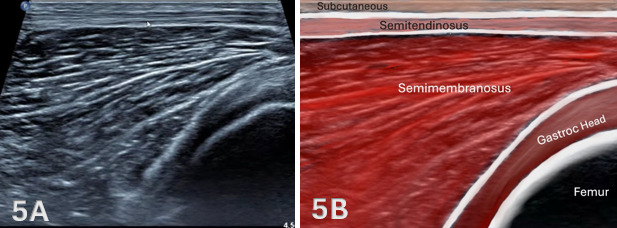
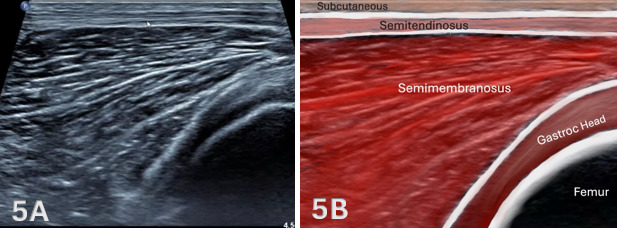
Figures 5A through 5B: Normal Medial, Hamstrings Distally in LAX
In long-axis (LAX) imaging, the medial hamstring musculature is first assessed distally, as shown in Figure 1D above, corresponding to the region previously identified in short-axis (SAX). At this level, the femoral condyles serve as a deep osseous landmark, with the medial gastrocnemius visualized superficial to the posterior femur. The semimembranosus muscle belly appears as a broad, fan-shaped structure that begins to taper as it progresses distally toward its myotendinous junction. The semitendinosus is identified as a more superficial and slender structure, maintaining a linear course along the medial posterior thigh.
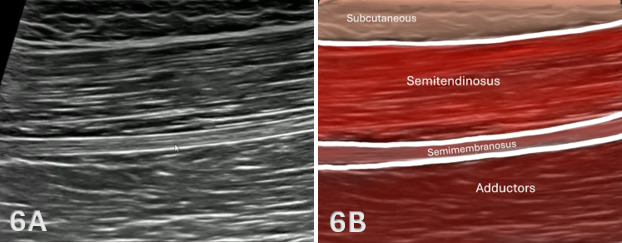
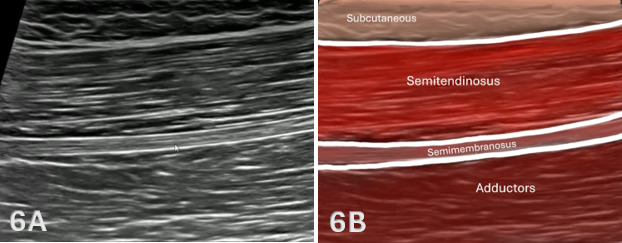
Figures 6A through 6B: Normal Proximal, Medial Hamstrings in LAX
As the transducer is advanced proximally in long-axis, shown in Figure 1E above, the medial hamstring musculature demonstrates progressive transition from muscle belly to aponeurosis and tendon as it approaches the ischial tuberosity. The semimembranosus continues to course deep and becomes more narrow and organized, forming a distinct aponeurotic structure that converges into a deeper tendon. The semitendinosus remains superficial and may continue to demonstrate its characteristic internal fascial band, although it becomes less prominent as the muscle transitions toward its proximal tendon.
Pathology of Medial Hamstrings:
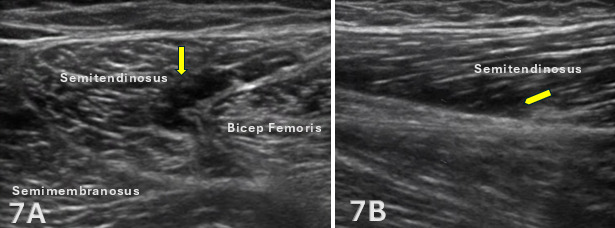
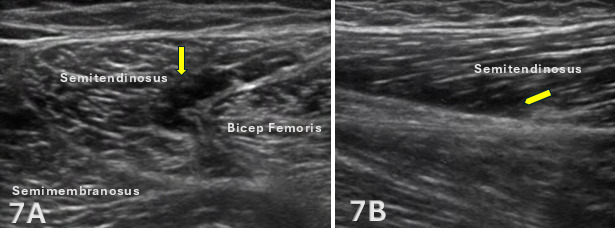
Figures 7A and 7B: Proximal Semitendinosus Muscle Strain, Grade 2
Figures 7A and 7B demonstrates an ultrasound imaging of a 26-year-old male with a grade II strain of the semitendinosus muscle. In short-axis, a focal anechoic region is visualized within the semitendinosus muscle (yellow arrow) at its interface with the biceps femoris long head, consistent with localized edema and hematoma formation. This region corresponds to the patient’s area of maximal tenderness and is outlined by yellow arrows. Long-axis imaging confirms disruption of the normal fibrillar architecture along the undersurface of the semitendinosus (yellow arrow), without evidence of complete fiber discontinuity or proximal tendon involvement.
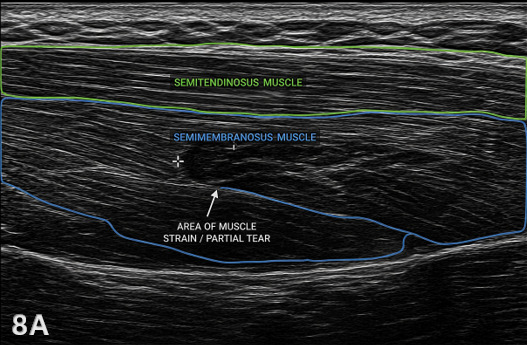
Figure 8A: Mid-Thigh Semimembranosus Strain in LAX
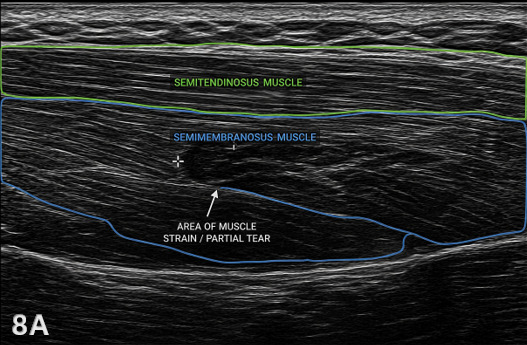
This is a LAX view of the medial posterior thigh. Superficially, we see the semitendinosus, which demonstrates a normal, organized fibrillar pattern. Deep to that is the semimembranosus. Within the semimembranosus, there is a focal hypoechoic area with disruption of the normal parallel fiber alignment indicating a Grade I-II muscle strain. The hypoechoic region may also represent localized edema or hemorrhage, which commonly accompanies acute muscle injury. The surrounding tissue may appear slightly more hyperechoic due to reactive changes. Key things to look for are loss of fibrillar pattern, changes in echogenicity, and comparison to adjacent normal muscle in this case, the semitendinosus helps confirm the abnormality.