Introduction
Anterior cruciate ligament (ACL) injuries are one of the most common knee injuries occurring in the United States with a reported incidence of about 68 per 100,000 people each year.1 ACL injuries are associated with substantial financial and clinical burden, including an estimated annual economic cost of approximately $7 billion in the United States, and potentially significant long-term morbidity, particularly when associated with concomitant meniscal or chondral injury.2 In response to this burden, the sports medicine community has emphasized injury-prevention programs such as the FIFA 11+ and PEP (Prevent Injury, Enhance Performance) protocols, which have demonstrated significant reductions in ACL injury rates.3–5
Patellofemoral conditions (PFC) represent a spectrum of anterior knee disorders, ranging from idiopathic patellofemoral pain to instability-related diagnoses including subluxation and dislocation. These conditions are common, particularly in young, physically active females.6 Idiopathic patellofemoral pain is primarily diagnosed clinically and is characterized by insidious onset of retro- or peripatellar pain.7 Patellofemoral conditions are multifactorial in origin and are commonly managed nonoperatively with individualized exercise-based rehabilitation targeting the hip and knee musculature.8 The prevalence of PFC ranges between 15–45% annually depending on the studied population with a reported average prevalence of 22.7% in the general population.7 Although PFC has historically been considered self-limiting, longitudinal data challenge this assumption. In one adolescent cohort, 65% of patients continued to report knee pain two years after diagnosis, and long-term follow-up studies have reported persistent symptoms in 20% to 91% of individuals 5 to 8 years after pain onset.9,10
Prior literature has suggested overlap between PFC and ACL injury with respect to neuromuscular and movement-related factors. Although multiple studies have documented shared biomechanical and neuromuscular features in PFC and ACL-injured populations, direct longitudinal evidence evaluating whether a prior PFC diagnosis is associated with increased subsequent ACL injury risk remains limited.11–14 The purpose of this study was to determine whether prior diagnosis of patellofemoral conditions (PFC) is associated with an increased risk of subsequent ACL injury and other intra-articular knee pathology.
Methods
Study Design and Setting
This retrospective cohort study was conducted within a large, multi-state integrated health system. Eligible patients were identified through the electronic medical record (EMR) within the health system. The observation period included index diagnoses of patellofemoral conditions (PFC) between January 1, 2014, and December 31, 2016, with follow-up for subsequent knee injuries or procedures extending through December 31, 2024. This study was approved by the institutional review board (Protocol #2022.106).
Participants
Inclusion criteria required patients aged 14 to 40 years at the time of PFC diagnosis and to have clear documentation of symptomatic PFC confirmed by International Classification of Diseases, Tenth Revision (ICD-10) codes (Table 1). ICD-10 codes were selected a priori to capture diagnoses considered clinically consistent with the patellofemoral spectrum, including instability, subluxation, dislocation, and chondromalacia, while excluding diagnoses such as fracture and tendinopathy. Exclusion criteria included a documented history of prior major lower extremity injury or surgery, systemic rheumatologic disease, degenerative joint disease, inaccessible medical records, or an initial PFC diagnosis outside the 2014–2016 study window. Follow-up was defined as continued EMR availability within the health system through the end of 2024. Patients with BMI values <18 kg/m2 or >50 kg/m2 and those with missing anthropometric data were excluded from BMI-specific analyses.
Variables
The primary exposure was a clinical diagnosis of PFC. The primary outcome was incident ACL injury. Secondary outcomes included meniscal, chondral, medial patellofemoral ligament (MPFL), and other knee injuries, as well as knee-related surgical procedures. A composite outcome was defined as the occurrence of at least one major knee injury or major knee procedure during the follow-up period. Major knee injuries were defined as a subsequent diagnosis of ACL tear, meniscal tear, chondral injury, or MPFL injury confirmed by ICD-10 code and/or surgical procedure code. Major knee procedures were defined as knee surgical procedures including ACL reconstruction, meniscectomy, chondroplasty, or MPFL reconstruction captured by CPT code. Covariates included sex, age at diagnosis, height, weight, body mass index (BMI), and laterality of symptoms. BMI categories followed World Health Organization thresholds.
Data Sources and Measurement
Diagnostic codes and procedure codes were extracted from the EMR and verified by manual chart review to confirm symptomatic presentation and accurate classification. The same protocol was applied across all patients, and uncertain cases were adjudicated by two board-certified orthopaedic surgeons with subspecialty clinical experience in patellofemoral conditions and knee injuries. ICD-10 codes used to define PFC are listed in Table 1.
Bias
Potential sources of bias included diagnostic misclassification of PFC, incomplete capture of injuries treated outside the health system, and systematic exclusion due to missing BMI data. These were mitigated by applying strict inclusion and exclusion criteria, using code lists standardized a priori, performing manual verification of diagnoses, and comparing injury incidence in excluded and missing-data groups.
Study Size
No a priori sample size calculation was performed. The study size reflected the entire available population of patients diagnosed with PFC within the health system during the study window.
Statistical Analysis
Cumulative incidence was estimated for each individual outcome and for the composite outcome and reported using 95% confidence intervals (CIs). Continuous variables were assessed for normality using the Shapiro-Wilk test. Because age, BMI, and weight were non-normally distributed, continuous variables were summarized as medians with interquartile ranges (IQRs) and compared using Wilcoxon rank-sum tests. Categorical variables were summarized as counts and percentages and compared using chi-square tests. Multivariable logistic regression was performed to evaluate independent associations between demographic variables and incident ACL injury, with age, sex, and BMI included as covariates. Crude and adjusted odds ratios (ORs) with 95% CIs were reported. Patients lacking valid anthropometric measures were excluded from BMI-specific analyses and from regression models including BMI but were retained in all other analyses. Statistical significance was defined by a 2-tailed alpha level of 0.05. No sensitivity analyses were conducted.
Results
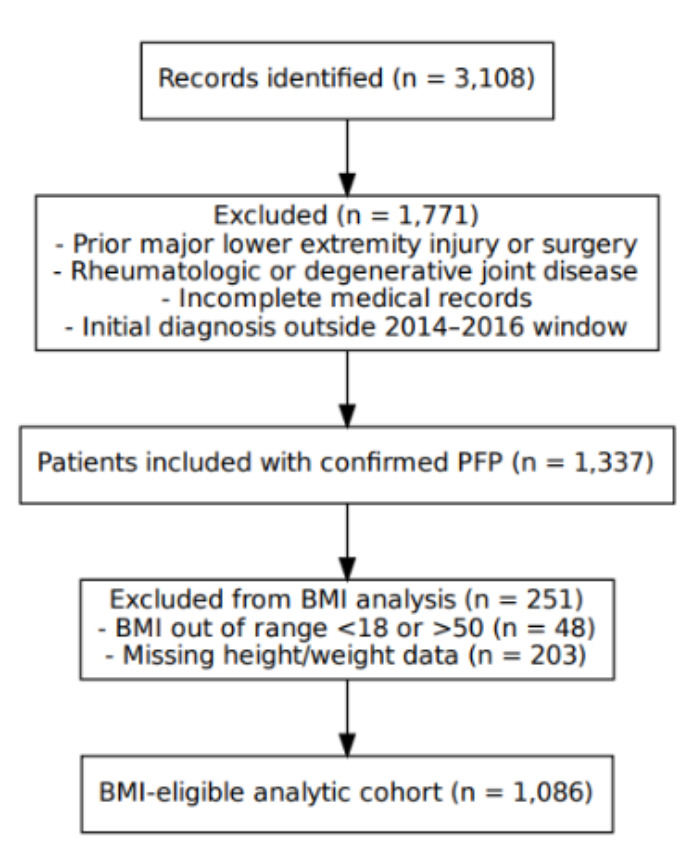
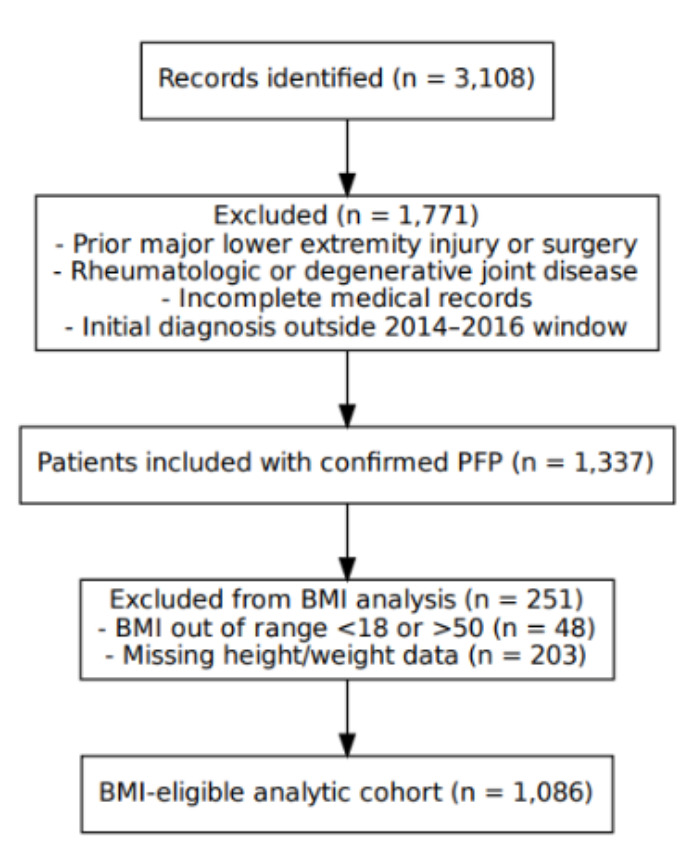
A total of 3,108 charts were screened; 1,232 patients met inclusion criteria following manual review, and 1,876 were excluded primarily because of unrelated diagnoses or index events outside the study window (Figure 1). Among the 1,232 patients with patellofemoral conditions (PFC), the median age at diagnosis was 19 years (interquartile range [IQR], 16–26), and 69.2% (n = 853) were female. Complete height and weight data were available for 1,086 patients (88.2%), who comprised the BMI-eligible cohort. Forty-eight patients had BMI values outside the prespecified analytic range (<18 or >50 kg/m²), and 203 had missing anthropometric data.
Among the BMI-eligible cohort, most PFC diagnoses were unilateral (80.1%, n = 987), with 41.2% involving the left knee and 38.2% the right; 17.6% of patients reported bilateral symptoms. The median age at initial PFC diagnosis was 20 years (IQR, 16-27). Treatment was recommended for 96.7% (n = 1,050) of the included cohort and consisted of supervised physical therapy, activity modification, bracing, or a combination of these at the discretion of the treating clinician. In the excluded and missing-data groups, treatment was recommended for 95.8% and 73.9% of patients, respectively.
Injury Incidence and Timing
Across the full cohort, 146 patients (10.9%; 95% confidence interval [CI], 9.1%-12.6%) experienced a subsequent knee injury or underwent a knee-related surgical procedure during follow-up. ACL injuries occurred in 2.5% of patients, and meniscal injuries occurred in 4.1%. Less frequent events included medial collateral ligament injuries (0.7%), osteotomies (0.6%), and patellar tendon injuries (0.2%). The median time from PFC diagnosis to any subsequent knee injury or procedure was 10 months (IQR, 1-41), and the median time to ACL injury was 10.5 months (IQR, 0-28).
Among patients with unilateral PFC (n=987), 12.1% sustained a subsequent knee injury, compared with 5.8% of those with bilateral symptoms. Among injuries with assignable laterality, 83.3% (n=100) occurred ipsilateral to the initial PFC diagnosis.
Injury Risk by Patient Characteristics
Patients who sustained a knee injury had significantly greater median weight at PFC diagnosis than those who did not (173 lb [IQR, 138–219] vs 159 lb [IQR, 133–194.5]; p = .0239). Median BMI was also significantly higher among injured patients than non-injured patients (26.74 kg/m² [IQR, 23.24–32.79] vs 25.40 kg/m² [IQR, 21.79–30.46]; p = .0250). No statistically significant differences were observed for age at PFC diagnosis (p = .3693), sex (p = .8775), or height (p = .8104) between patients who sustained a knee injury and those who did not (Table 2). Although not statistically significant, a greater proportion of injured patients were classified as obese (29.1% vs 22.95%), and BMI category distribution showed a trend toward higher injury prevalence with increasing BMI. Among patients who sustained ACL injuries (n = 26), 67.7% (n = 21) were female, and the median age at ACL injury was 20 years (IQR, 16–29).
Multivariable Regression for ACL Injury
Multivariable logistic regression adjusting for age, sex, and BMI did not identify any statistically significant independent predictors of ACL injury (Table 3). All 95% confidence intervals for the crude and adjusted odds ratios crossed 1.
Comparisons With Excluded and Missing-Data Cohorts
The group excluded because of out-of-range BMI values (n = 48) was younger, had a lower mean BMI, and included a greater proportion of males compared with the BMI-eligible cohort. The missing-data group (n = 203) had generally similar demographics to the included cohort, although treatment was recommended less frequently (73.9% vs 96.7%). Despite these differences, injury prevalence was similar across groups: 6.3% in the excluded group and 11.3% in the missing-data group.
Discussion
This retrospective cohort study found that patients with patellofemoral conditions had a higher incidence of subsequent ACL injury than that reported in the general population. ACL injuries occurred in 2.5% of the cohort, corresponding to an incidence of approximately 246 per 100,000 person-years, while meniscal injuries occurred in 4.1%. Subsequent injuries occurred relatively early after the index PFC diagnosis, with a median time to ACL injury of 10.5 months, and most injuries with assignable laterality occurred ipsilateral to the index PFC diagnosis.
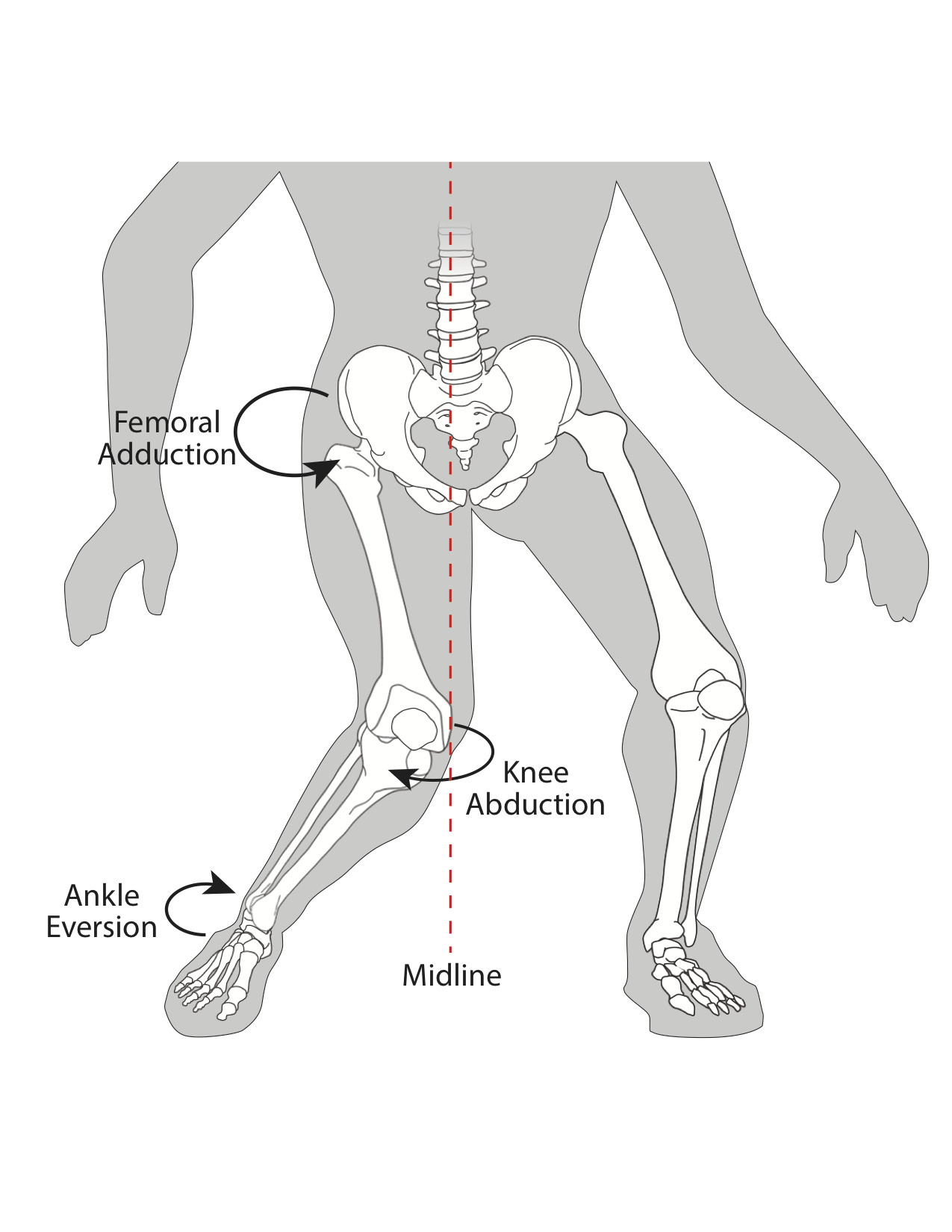
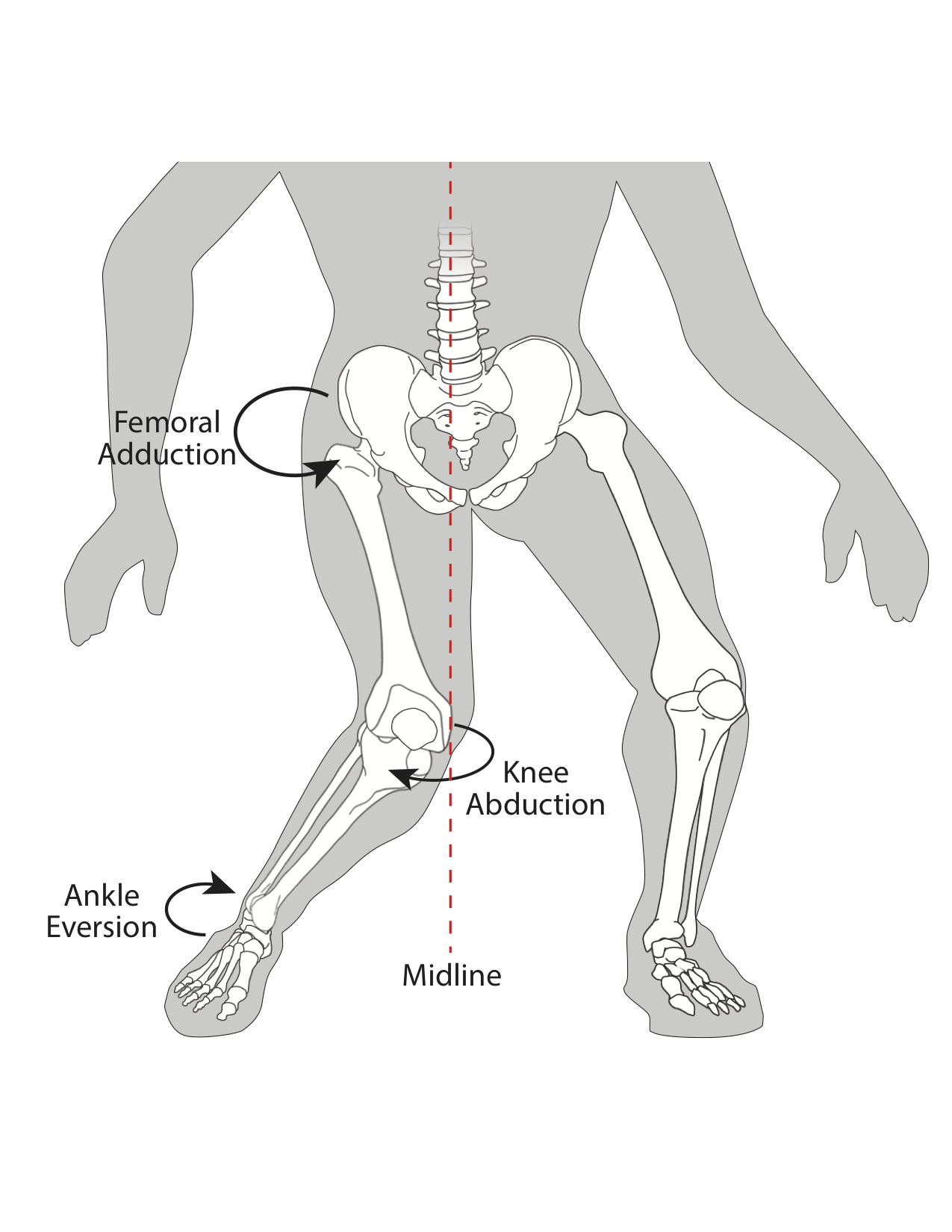
Prior literature has shown that patellofemoral pain and ACL injury share several biomechanical and neuromuscular features, including altered frontal-plane mechanics, dynamic valgus patterns, and deficits in proximal control.11–14 In that context, the increased ACL injury incidence observed in this cohort is biologically plausible, although the present study did not directly measure biomechanics, neuromuscular control, or movement quality. Accordingly, the findings should be interpreted as demonstrating an association between prior PFC diagnosis and later ACL injury, rather than establishing a causal mechanism. A dynamic valgus pattern is illustrated conceptually in Figure 2.
The absence of significant independent predictors of ACL injury in the multivariable model suggests that age, sex, and BMI alone did not explain the elevated ACL injury incidence observed in this cohort. At the same time, higher weight and BMI were associated with subsequent knee injury in unadjusted analyses. Taken together, these findings suggest that additional unmeasured factors may contribute to injury risk in this population and warrant prospective study.
Higher BMI and body weight were associated with subsequent knee injury in unadjusted analyses. Although BMI was not an independent predictor of ACL injury in multivariable regression, the trend toward greater injury prevalence among patients with obesity may still be clinically relevant. Prior work has identified BMI as a risk factor for ACL injury in some athletic populations.16,17 In the present study, BMI may reflect one component of risk, but it did not independently explain ACL injury occurrence after adjustment for age and sex.
The observed timing of injury may have clinical relevance. The median time to ACL injury was 10.5 months after the index PFC diagnosis, suggesting that the period after initial presentation may represent an interval during which clinicians should remain attentive to persistent symptoms, recurrent instability, or worsening functional complaints. However, the present study did not evaluate rehabilitation protocols, adherence, or prevention-program effectiveness, and therefore cannot determine whether specific interventions would reduce subsequent injury risk.
Beyond ACL injury, this cohort also demonstrated a broader burden of subsequent knee pathology, particularly meniscal injury. This finding suggests that the association between PFC and later knee morbidity may not be limited to ACL injury alone. Future studies should prospectively examine the full spectrum of subsequent intra-articular pathology after PFC diagnosis to better define the overall burden and clinical implications of these conditions.
The findings should also be interpreted considering several limitations. The analysis was confined to patients within a single integrated health system, which may limit generalizability. Injuries or procedures treated outside the health system may not have been captured. The retrospective design did not permit reliable accounting for patients lost to follow-up, those who relocated, or those who changed care providers. Diagnostic misclassification is also possible, because PFC represents a heterogeneous group of diagnoses despite the use of predefined inclusion criteria and manual chart review. In addition, important confounders such as sports participation, activity level, rehabilitation adherence, treatment variation, and other medical comorbidities were not available in the dataset. Patients with BMI values >50 kg/m² were excluded from BMI-specific analyses to reduce the influence of likely data-entry errors or physiologic extremes; notably, higher BMI was associated with greater injury prevalence in unadjusted analyses, but not as an independent predictor of ACL injury in multivariable modeling.
Conclusion
Patients with patellofemoral conditions demonstrated a higher incidence of subsequent ACL injury than that reported in the general population. The observed timing of injury and predominance of ipsilateral events suggest that a prior diagnosis of PFC may identify a subgroup at greater risk for later knee injury. These findings support the need to pay closer clinical attention to patients with PFC, but the present study does not establish causation or define the underlying biomechanical mechanism. Larger prospective studies incorporating activity data, functional assessment, and biomechanical analysis are needed to clarify which patients are at greatest risk and whether targeted prevention strategies are effective.
Corresponding author
Anthony Drazick
5444 S Burbank Drive, Baton Rouge, LA 70820
Email: Anthony.drazick@ochsner.org
Conflicts of Interest
There are no conflicts of interest to report.
Data sharing statement
De-identified data from this study, including extracted demographic variables, ICD-10 code classifications, and aggregated injury outcome data, are available from the corresponding author upon reasonable request. Data may be requested by contacting A.T.D. at Anthony.drazick@ochsner.org. Access will be granted for research purposes that are methodologically sound and consistent with institutional and IRB policies. Shared data may be reused for secondary analyses, replication studies, or meta-analytic synthesis, but redistribution of the raw dataset or any attempt to re-identify participants is prohibited. No identifiable patient information will be shared.