INTRODUCTION
During overhead throwing, athletes complete coordinated joint movements to transfer energy through the kinetic chain (KC). As a thrower strides forward to initiate the throwing action, energy generated from the lead leg at foot contact (FC) is translated through the lower limb to the core segment of the KC,1 before continuing through to the trunk, scapula and upper extremity. The KC segments have been outlined as lower extremity, lumbo-pelvic hip complex (LPHC), upper extremity and wrist/hand,2 with each segment performing key roles in ensuring efficiency within the upper extremity during overhead sports.3
Varying shoulder injury prevalence has been reported across overhead sports. Between 44-75% of elite handball players have a history of shoulder pain,4,5 with approximately 68% having training impacted as a result of pain.5 Shoulder injuries are the most prevalent injury within tennis, reported to be between 25-47.7%,6,7 and approximately 23% of English county cricketers suffer from a shoulder injury in their throwing arm.8 The high number of rotations that the throwing shoulder undertakes throughout a season in all overhead sports can increase the stress on both the glenohumeral joint (GHJ) and the shoulder girdle and can result in injury (failure).9 For baseball, it has been reported that 16.1% of all injuries at NCAA level between 2014 and 2019 were shoulder injuries, with 18.5% of injuries occurring as a result of pitching.10
Across the overhead throwing movement, upper limb and scapular muscles are active to position and protect the shoulder during movements of high acceleration and force generation. The trapezius and serratus anterior (SA) muscles work to position the scapula, the connection between the trunk and throwing arm within the KC,11 in order to maintain the acromial space as the throwing arm is moved into position.12,13 High levels of supraspinatus (SSP) and infraspinatus (ISP) activity ensure glenohumeral compression14,15 and resistance against humeral head translation,16–18 particularly during the arm-deceleration phase when a thrower is most susceptible to injury. During this phase, both the latissimus dorsi (LD) and pectoralis major (PM) are also active to decelerate the throwing arm.19 However, the LD and PM are also key muscles for energy transfer through the KC,16,20 with both muscles achieving high activity levels during the arm-acceleration phase.14,21 The PM is particularly important as a power-generating muscle22 responsible for generating high internal rotation angular velocities of the throwing shoulder.14
The importance of stability within both the lower limb and the lumbopelvic-hip complex (LPHC) cannot be understated. The LPHC provides the link between the upper and lower extremities within the KC23 and is responsible for maintaining stability of both the spine and pelvis24 as the pelvis and torso pass over the stance leg during overhead throwing.25 Research has shown that high levels of muscle activity are required during the overhead throw to both move and stabilize the lower limb and core. In baseball pitchers, studies have shown that peak activity of the abdominal obliques reached 75-100% MVIC26 and gastrocnemius, rectus femoris and gluteus maximus all exceeding 100% MVIC.27 Deficits in lower limb stability, core strength and scapular movement patterns have been found in 50-67% of athletes with shoulder injuries.28–30 As a result, breaks in efficient KC sequencing require distal segments to increase functional capacity in order to achieve the same force and load within the movement; and this has been described as the ‘catch-up’ phenomenon.31
For an overhead athlete to complete rehabilitation from a shoulder injury, four phases have been proposed: acute, intermediate, advanced strengthening, and return-to-activity.32,33 Each has specific rehabilitative goals, with the intensity and demands increasing to highlight progression throughout the rehabilitation process. Several approaches include whole-body considerations that activate different bodily segments, including the LPHC, while performing shoulder exercises.34 The introduction of an isotonic exercise program is common across the intermediate and advanced rehabilitation phases, with the Advanced Throwers Ten (ATT) being a key component to attaining neuromuscular control and developing strength, power and endurance.33 The ATT consists of ten base exercises, some with variations, requiring participants to perform three set of ten repetitions, with each set allowing a sequential progression that challenges endurance through bilateral and unilateral movements, together with sustained holds. Exercises include shoulder movements across different planes of motion, all in combination with stability and core strengthening.
Key considerations for injury prevention and rehabilitation have been outlined in numerous studies, including specific exercises to develop strength and functionality of upper limb muscles through open- and closed-KC chain approaches.35–38 While studies have investigated the effectiveness of the Throwers Ten39 and proposed alterative Arm Care Programs, such as the Nicholas Institute of Sports Medicine and Athletic Trauma (NISMAT) program,40 no study has investigated muscle activity levels across KC segments during the Advanced Throwers Ten program for shoulder rehabilitation collectively, particularly focussing on both healthy and injured throwers. Therefore, this research study aimed to measure the activation levels (%MVC) of key KC muscles in healthy and injured overhead throwing athletes during selected exercises within the ATT program. The authors hypothesized that different activations levels would be apparent between throwing groups across exercises, and that strengthening levels of activity would be evident in both groups across all KC segments.
METHODS
Participants
A total of thirty-three male overhead throwing athletes participated in this study; seventeen were healthy and sixteen were injured. All participants were overhead athletes recruited from local and regional baseball, cricket, and handball sports clubs, and were allocated into two groups; healthy and injured. Inclusion criteria was based on shoulder injury history, with healthy defined as those who had no history of injury to their throwing shoulder or upper limb. Injured participants had a clinical history of shoulder injury (i.e. shoulder instability [n = 3] or rotator cuff disease [n = 13]) within the previous three years, as well as difficulty or pain during performance as indicated in the Sports Module section of the quick Disability of the Arm, Shoulder and Hand (qDASH) questionnaire.41 The Sports Module consists of four questions, which assess a participant’s physical ability to play their sport in the past week. Participants are required to provide a score for each question (1 – No difficulty; 2 – Mild difficulty; 3 – Moderate difficulty; 4 – Severe difficulty; 5 – Unable). When scoring the responses, participants who scored zero were assigned to the healthy group, with participants scoring greater than zero assigned to the injured group. Overhead athletes were excluded if they had no history of shoulder injury but registered difficulty or pain when completing the qDASH. The study received ethical approval from the National Research Ethics Committee. All participants were provided with a detailed information sheet at least 72 hours before their participation outlining the main details of the project and measurement procedures. All participants gave written consent before undertaking any data collection.
Exercises
Participants completed one set of selected exercises within the Advanced Throwers Ten (ATT) Exercise Program. The selected exercises included Seated Full Can, Seated Lateral Raise, Sidelying ER, T-Raises, Y-Raises, Prone Row into ER (all using 1kg dumbbells), Seated External Rotation (ER), Seated Extension into ER, Seated Extension into 45o ER, Standing Low Row (using standardized resistance tubing) and Wall Circles (clockwise and anti-clockwise). The dumbbell weight was standardised to ensure all participants, regardless of injury status, could comfortably hold them throughout the duration of the exercises. This is consistent with the ATT protocol.33 One set consisted of ten repetitions, with each exercise explained to the participants and followed by a familiarization session. A metronome set at 60 beats per minute was used to aid participants in the speed at which they completed each repetition of each exercise. In accordance with the ATT program, a stability ball was used during all seated and prone exercises. For seated exercises, participants were required to maintain good posture throughout with both feet planted on the floor at shoulder width apart. For exercises requiring the participant to lie prone on the stability ball, the abdomen needed to be in contact with the ball and the trunk in a parallel position to the floor. Two minutes rest was permitted between exercises during which instructions were given about the next exercise.
Measurement Protocol
A 16-channel TeleMyo TDS System (Noraxon USA, Inc., Scottsdale, Arizona, USA) and associated MyoResearch software (version 3.8.6) were used for signal acquisition, processing, and analysis. Raw EMG signals were amplified (CMR: > 100 dB; input impedance: > 100 Mohm; and Base Gain: 200 dB), with signals collected at 1500 Hz and band-pass filtered at 20 to 250 Hz for surface electrodes and at 20 to 350 Hz for fine-wire electrodes.
Self-adhesive Ag/AgCL snap, surface dual electrodes (Noraxon USA, Inc) were placed parallel with the muscle fibers in accordance with SENIAM guidelines, with an inter-electrode distance of 20mm, to record EMG from muscles across KC segments. Surface EMG was collected for sixteen muscles; biceps brachii (BB), anterior, medial and posterior deltoids (AD, MD, PD), upper and lower trapezius (UT and LT), pectoralis major (PM), latissimus dorsi (LD), serratus anterior (SA), infraspinatus (ISP), contralateral external oblique (EO), gluteus maximus (GM), biceps femoris (BF), rectus femoris (RF) and lateral gastrocnemius (LG). Skin preparation included shaving the site and cleaning by an alcohol-free moist tissue (Kay’s Medical, UK). A disposable bi-polar hook intramuscular fine-wire electrode (size: 0.50x30mm (10cm wire) (Spes Medica S.r.l., Genova, Italy) by hypodermic needle42 was administered by one member of the research team (OK), and used to record signals from the supraspinatus (SSP).
Raw EMG signals from ten repetitions of each exercise (the first and last repetitions were omitted for consistency purposes) were smoothed (1500 sample/window), full-wave rectified (400 sample/window) and a root mean square (RMS) amplitude algorithm with a window size of 100ms applied. EMG from each muscle was recorded during Maximal Voluntary Contraction (MVC) during a manual muscle test for normalization purposes. Manual muscle testing was performed by the lead investigator using procedures previously reported in functional exercise research.43–46 Two, five second efforts, with verbal encouragement, were recorded for each muscle, with the mean calculated for normalization during each exercise and reported as %MVC. A one-minute rest period was permitted between each MVC trial.
Data Analysis
A three-way ANOVA test was performed to determine group, exercise and muscle effects, and interaction between them. Mauchly’s Test of Sphericity was performed to assess the variance of within-subject conditions47 and on occurrences of violation (p < 0.05), the appropriate epsilon correction was chosen. One-way ANOVA tests were performed to identify muscle activity differences between exercises for injured and healthy groups. Post-hoc independent t-tests were performed to assess the statistical differences between groups for muscle activity during each exercise. The level of statistical significance was set to p < 0.05.
In order to compare directly between exercises and to ascertain the functionality of a muscle in that given movement/exercise, muscle activity levels were quantified. Several studies have outlined a classification system to quantify muscle activation levels during rehabilitation exercises: 1) 0-20% MVC: low activity, 2) 20-40% MVC: moderate activity, 3) 40-60% MVC: high activity, 4) over 60% MVC: very high activity.14,48 It has been reported that high activity levels between 40-60% MVC muscle activity should be elicited when performing exercises for strength-based development.49
RESULTS
Participant Characteristics
Healthy throwers (n: 17; age: 24.6 ± 6.5 years; height: 181.6 ± 4.9 cm; weight: 87.1 ± 23.0 kg) and injured (n: 16; age: 31.8 ± 10.1 years; height: 182.6 ± 8.1 cm; weight: 87.9 ± 17.5 kg) completed all exercises. The qDASH Sport Module Scores used to assign participant groups were recorded as 0.00 (± 0.00) for healthy throwers and 35.29 (± 26.42) for injured throwers.
Muscle Activity Comparisons
Main effects were present between groups, exercise, and muscle (all p < 0.001). Significant interaction effects were evident between group and exercise (p = 0.009), group and muscle (p < 0.001) and exercise and muscle (p < 0.001). However, no significant interaction effect was evident between group, muscle, and exercise (p = 1.000).
Muscle activities differences were evident when comparing all exercises in both groups, with all muscles recorded as p < 0.001, except for BB (p = 0.023), SSP (p = 0.004) and EO (p = 0.098) for injured throwers and EO (p = 0.143) for healthy throwers. Injured throwers elicited higher muscle activity for ISP during T-Raises (p = 0.042) and Prone Row into ER (p = 0.022), recording high activity levels compared to moderate levels in healthy. AD activity during Seated ER (p = 0.040), Y-Raise (p = 0.030) and Seated Extension into ER (p = 0.035), BF during Wall Circles (ACW) (p = 0.011) and LG during Wall Circles (CW) (p = 0.040) were all higher for injured throwers, although all recruitment levels were very low (< 11%MVC).
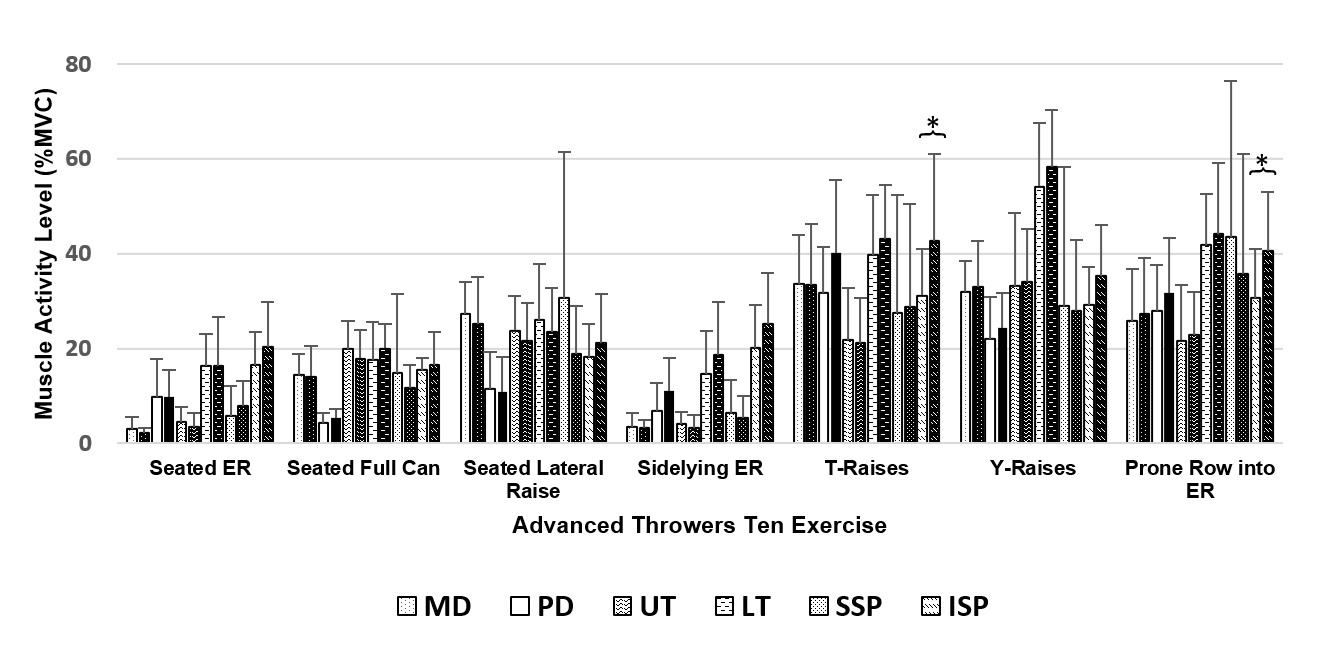
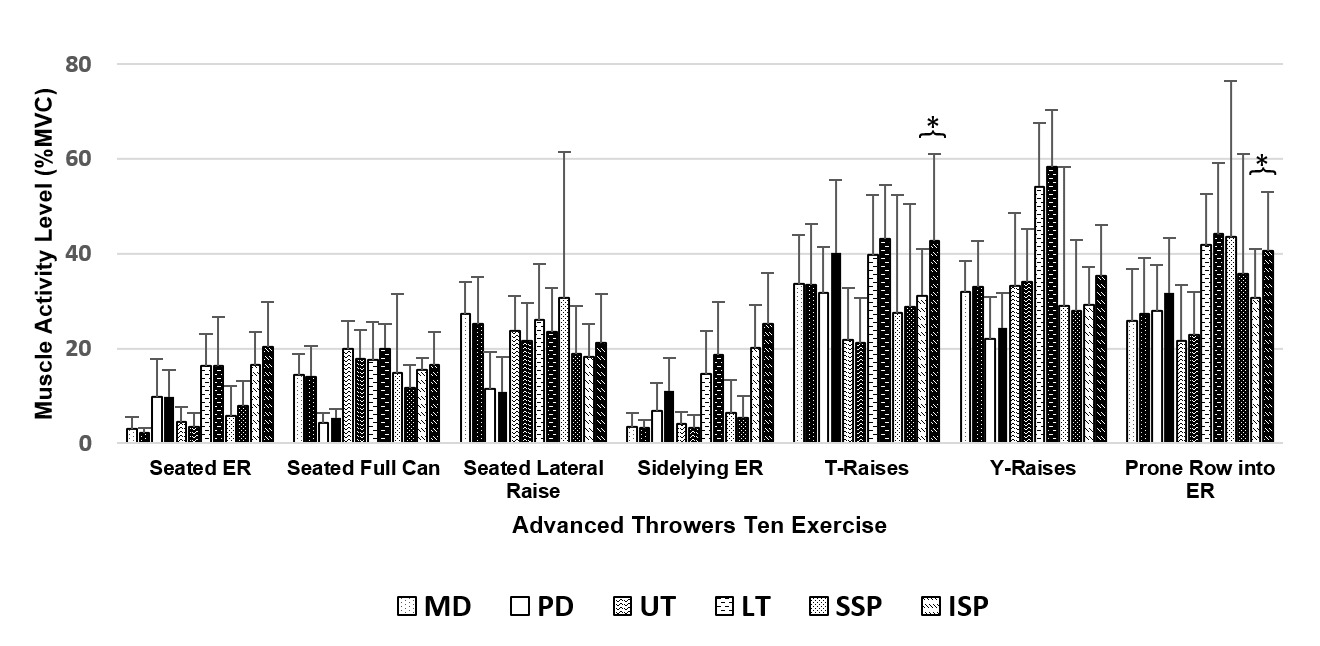
Strengthening levels of activity (> 40%MVC) were evident for several muscles in both groups. For healthy throwers, strengthening levels were achieved for LT during both Y-Raises (54.2 %MVC ± 13.5) and Prone Row into ER (41.8 %MVC ± 10.9), and SSP also during Prone Row into ER (43.5 %MVC ± 33.0). Injured throwers also elicited strengthening levels of activity for PD during T-Raises (40.1 %MVC ± 15.4), LT during T-Raises (43.1 %MVC ± 11.5), Y-Raises (58.4 %MVC ± 11.9) and Prone Row into ER (44.2 %MVC ± 15.0), and ISP during T-Raises (42.7 %MVC ± 18.4) and Prone Row into ER (40.6 %MVC ± 12.4).
Muscle Activity during Rehabilitation Exercises for Healthy and Injured Throwers
Deltoids
Both groups elicited higher MD activity during Seated Lateral Raise, T-Raises, Y-Raises and Prone Row into ER compared to all other exercises (healthy: p < 0.001 – 0.014; injured: p < 0.001 – 0.037). T-Raises elicited the highest PD activity in both groups when compared to all other exercises (healthy: p < 0.001 – 0.007; injured: p < 0.001), except for Prone Row into ER (healthy: p = 0.925; injured: p = 0.148).
Trapezius Muscles
UT activity was significantly higher for Y-Raises compared to all other exercises for injured throwers (p < 0.001 – 0.004) and healthy throwers (p < 0.001 – 0.014), with the exceptions of Seated Lateral Raise (p = 0.110) and Seated Extension into 45o ER (p = 0.383) in the latter group. Highest LT activities levels were also evident during Y-Raises and significantly higher compared to all other exercises for both groups (healthy: p < 0.001 – 0.012; injured: p < 0.001 – 0.007).
Rotator Cuff
For SSP, Prone Row into ER elicited the highest muscle activity in both groups, although was only significantly higher compared to Seated ER (healthy: 0.010; injured: p = 0.022) and Sidelying ER (healthy: p = 0.020; injured: 0.006). T-Raises elicited the highest ISP muscle activity in both groups, yet no statistical differences were evident between the T-Raises, Y-Raises and Prone Row into ER, (healthy: p = 0.999 – 1.000; injured: p = 0.810 – 1.000).
Core and Lower Limb
Differences between muscle activities for GM RF, BF and LG were evident between all exercises for healthy (all p < 0.001) and injured throwers (all p < 0.001), but not for EO muscle activity for any exercise for either group (healthy: p = 0.143; injured: p = 0.098). Muscle activities for EO, GM, RF, BF and LG showed low activity across all exercises.
Activity Level Classification Differences
High versus Moderate Activities
Differences in activity level classifications were evident for upper limb muscles, with injured throwers recording high levels of activity (> 40% MVC) for PD (40.1 %MVC ± 15.4 v. 31.8 %MVC ± 9.7), LT (43.1 %MVC ± 11.5 v. 39.7 %MVC ± 12.7) and ISP (42.7 %MVC ± 18.4 v. 31.2 %MVC ± 9.7) during T-Raises, and ISP during Prone Row into ER (40.6 %MVC ± 12.4 v. 30.6 %MVC ± 10.3). Both ISP activity differences were significant (p > 0.05) (Figure 1). SSP activity was high in healthy throwers compared to moderate for injured throwers (43.5 %MVC ± 33.0 v. 35.8 %MVC ± 25.3). although this difference was non-significant.
Moderate versus Low Activities
Injured throwers recorded moderate ISP activity during Seated ER (20.3 %MVC ± 9.5) v. 16.6 %MVC ± 6.9) and Seated Lateral Raises (21.2 %MVC ± 10.4) v. 18.2 %MVC ± 6.9), as well as for LT activity during Seated Full Can (20.0 %MVC ± 5.1 v. 17.6 %MVC ± 7.9). Healthy throwers elicited low activity (< 20 %MVC) for these muscles during the same exercises. Moderate SSP activity was evident for healthy throwers during the Seated Lateral Raise (30.7 %MVC ± 30.8) compared to low activity for injured (18.9 %MVC ± 10.1). All differences between moderate and low activity level classifications were non-significant.
DISCUSSION
The “Advanced Throwers Ten” (ATT) is an exercise program designed to challenge neuromuscular and proprioceptive demands while engaging all segments of the KC.33 This research study aimed to measure the activation levels (%MVC) of key KC muscles in healthy and injured overhead throwing athletes during selected exercises within the Advanced Throwers Ten. Findings indicated minimal muscle activity level differences existed between healthy and injured throwers across several exercises. Only three exercises, all performed prone on a stability ball, elicited strengthening-based activity levels (> 40%) in trapezius and rotator cuff musculature, although the activity level differed between groups. While some upper limb muscles reached moderate muscular activity (20-40%MVC) in selected exercises, the majority of muscles investigated, particularly those in the core and lower limb, elicited low (< 20%MVC). These findings suggest the ATT does not adequately provide strengthening stimuli across all KC segments using the dumbbell weight or resistance tubing included in this study, regardless of throwers being in a seated, standing or prone position.
Muscle Activity Comparison Across Throwing Groups
Muscle activity differences (%MVC) between groups were evident for ISP activity during T-Raises and Prone Row, and AD activity during Seated ER and Y-Raises, with injured throwers recording higher activity compared to healthy throwers. While AD activity was very low in both exercises for both groups (< 8%MVC), variation in ISP activity was noted. Injured throwers were found to elicit high levels of activity compared to moderate activity in healthy throwers during both T-Raises and Prone Row into ER. T-Raises, Y-Raises and Prone Row into ER exercises are performed in a prone position, with the participant lying on a stability ball. It has been proposed that these exercises have been shown to reduce the effects of gravity on muscle activation levels,48 while providing challenge across different KC segments, most notably posterior rotator cuff muscles, periscapular muscles and lumbar and gluteal muscles.50 The activity levels recorded for the ISP during Prone Row into ER were similar to those previously reported by Alizadehkhaiyat and colleagues51 for participants performing ER at 90o abduction only while prone on a bed (38.0%MVC), but lower than those reported by Reinold and colleagues52 for the same exercise protocol. During Prone Row into ER, higher levels of SSP and ISP activity are needed to dynamically stabilize the shoulder.53 When comparing groups, injured throwers recorded high levels of ISP activity compared to moderate levels in healthy throwers during this exercise, whereas healthy throwers recorded high levels of SSP activity compared to moderate levels in injured throwers.
Strengthening Levels of Activity
Limited strengthening levels of activity were evident across several ATT exercises, with surprisingly low activity elicited by the core and lower limb muscles, as well as some upper limb muscles. This was regardless of whether the throwers were seated, prone or standing. Given the intensity of the overhead throwing action, and the high levels of muscle activity required to stabilize the core and lower limb, it was expected that ATT would provide sufficient strengthening levels of stimulus across all segments of the KC to prepare the athletes ahead of returning to activity. Across all exercises, only prone exercises elicited activity that could be considered at a strengthening level. This was for only three muscles in injured throwers (PD: T-Raises; LT: T-Raises, Y-Raises and Prone Row into ER; ISP: T-Raises and Prone Row into ER) and only two muscles in healthy throwers (LT: Y-Raises and Prone Row into ER; SSP: Prone Row into ER).
The rotator cuff musculature is of high importance throughout throwing motions, specifically to ensure glenohumeral compression,14,15,54 but also to resist humeral head translation by generating a posterior force on the joint.15,17,18 In javelin throwers, SSP and ISP activities have been reported to reach 93.4%MVC and 94.7%MVC respectively during arm abduction and elevation.55 In addition, very high levels of activity are required by the posterior muscles (ISP and PD) after ball release to aid arm deceleration and resist humeral head translation,14,21 with PD activity exceeding 100%MVC during this throwing phase.55 Therefore, strengthening of these structures is key to ensure the throwing shoulder can be positioned as required during arm-cocking, as well as cope with the stress that is placed across the shoulder joint during the ballistic forward motion through ball release and follow-through. Strengthening levels of activity were recorded for both the ISP and PD during T-Raises in injured throwers. While it is not expected that the ISP or PD would be the primary target muscles of this exercise, muscle activity differences between groups were evident, with healthy throwers showing moderate activity compared to high activity in injured throwers. The ISP has been reported as the main stabilizing muscle during ER, co-activating with the PD.52 However, increasing PD activity can compensate for ISP weakness56 and it is suggested that is what is occurring during this movement, particularly for injured throwers. As the arms are raised into the highest position, increased activity may be needed to avoid humeral head translation. Therefore, this exercise may be of greatest challenge to injured throwers and may require additional activity to protect the shoulder joint as it is moved into this position.
The high activity levels recorded for the LT during prone exercises in both groups, except for healthy throwers during T-Raises, are similar to those previously reported by Ekstrom and colleagues,35 who found high activity levels during both T-Raise and Y-Raises together with very high UT and high LT activity during prone rowing. The prone lying exercises replicate abduction and ER movements experienced during overhead throwing and the co-ordinated movements of the muscles are essential for assuring the sub-acromial space is maintained.57 The scapular muscles perform a key role of achieving acromial clearance during the different phases of overhead throwing, particularly during arm-cocking,13 arm-acceleration and arm-deceleration.14,58 Therefore, strengthening of the trapezius muscle group and SA should be important considerations for any shoulder rehabilitation program.
Engaging the Core Musculature and Lower Limb
Despite selected ATT exercises requiring participants to be either seated or prone on a stability ball to target the core musculature, findings of this study have shown all exercises failed to elicit activity above ≈11%MVC across the core and lower limb. These activity levels are significantly below considerations for strengthening stimuli. Despite the stability ball being used to provide challenge during seated and prone exercises, minimal muscular activation differences can be observed when comparing exercises completed in a standing position, suggesting only stabilizing and general functioning levels of activity being achieved across the complete set. This is an important finding and has implications for preparing the overhead athlete to return-to-play, with insufficient preparation of the core and lower limb likely to result in vulnerabilities in KC sequencing and increase susceptibility to the aforementioned ‘catch-up’ phenomenon.31
The core musculature is important for both trunk rotation and core stabilization, and is reliant on the co-ordinated activation of the internal and external obliques, rectus abdominus and transversus abdominis.59 Previous research in professional baseball players has shown that peak oblique activities of 75-100%MVC are reached during throwing,26 and this level of activity is required in order to aid the stretch-shortening cycle that is formed as the thorax and trunk rotated away and then towards the target.60 In addition, a direct relationship between GM activity and pelvic rotation has been reported in high school pitchers.61 Therefore, achieving sufficient strengthening of these structures is key for the overhead athlete. However, low activity levels were elicited across all selected exercises for both healthy and injured throwers in this research study for both contralateral EOs (< 5.1%MVC) and GM (< 10.8%MVC). Given the importance of the EOs to KC sequencing for transferring energy during pelvic and thorax rotation towards the target, and of the GM in providing pelvic stability to aid pelvic rotation, additional strengthening exercises across the core should be considered in addition to those in the ATT. Traditional exercises, such as plank, side plank and crunches (both traditional and oblique) have been shown to elicit high levels of EO activity,62 while still engaging muscles across the KC. Alternatives also shown to elicit high or very high EO activity include a roll-out, pike and knee-up position using a Power Wheel,63 and using the CoreX, which is sports performance protocol with resistance bands.62 Exercises that also excite muscle spindle potential as part of pre-stretching would also be beneficial to aid energy transfer through the KC as the pelvis rotates away and then towards the target.
Both RF and BF are important factors in maintaining the stability around the knee and hip as overhead throwers attempt to create a base of support from foot contact onwards. The importance of maintaining balance during single-leg support while the upper body pivots over the lead leg during the early phases of overhead throw has been reported,64 and the BF and RF play an important role during this time in combination with the GM. Similar to muscle activation levels shown by the core musculature, this study found low levels of activity for lower limb muscles during all exercises. Activity of the RF and LG were recorded to be consistently below 10%MVC in both groups, with BF activity peaking at 11.4% MVC during Y-Raises in injured throwers. These activities suggest that muscles are acting in a stability capacity during each movement. While this activity may be useful for aiding the performance of each exercise, the activity falls significantly below the levels previously reported for these muscles during maximal overhead throwing.26 This may result in inadequate levels of activity to create the base of support required to allow the pelvis and trunk to rotate towards the target, and subsequent energy transfer through the KC.
Exercise Considerations
Given the previously outlined importance of scapular muscles, no strengthening levels of activity could be identified for the UT and SA for any exercises for either group, with only strengthening levels for the LT in the aforementioned prone lying exercises. Activity levels in most exercises were of low or moderate activity, suggesting stability functioning.49 Surprisingly, this was also the case during the Lower Trapezius 5 Series (LT5 Series) exercises, that are included in the ATT to target LT isolation and scapular control.33 The exercises include Seated Extension into ER, Seated Extension into 45o ER, Wall Circles, Standing Low Row and Standing Table Press-downs with Scapula Depression, all except for the latter exercise were investigated in this study. Both groups recorded low LT activity levels for Seated Extension into ER, Wall Circles and Standing Low Row, but moderate levels of activity during Seated Extension into 45o ER. Despite not achieving strengthening levels, it can be proposed that this exercise did achieve sufficient levels to target scapula control. Participants are required to move into shoulder extension, which makes a ‘W-shape’ with the arms through 45o ER. This results in the scapula tilting posteriorly during the ER component of the exercise, activating the LT. The W-shape is of paramount importance during rehabilitation and strengthening programs as it activates muscles that provide scapular stabilisation. Oliver and colleagues37 found that making the W-shape during a lunge activated UT, LT and SA between 22.5-27.6% MVC and thus recommended that the position is used in combination with exercises focusing towards developing the lower extremity segment of the KC. The results of the present study are similar for trapezius muscle activity but not for SA activity. Findings would also support the use of the ‘W-shape’ in both open- and closed- KC exercises to engage the scapular muscles. The Seated Extension into 45o ER exercise did also elicit moderate activity levels of both SSP and ISP, which can be attribute to the prevention of humeral head translation during rotational movements and ensuring stability around the shoulder.65
Finally, given the importance of the LD and PM to energy transfer through the KC during overhead throwing16,20 and their role in arm deceleration after ball release,19 the ATT does not appear to stimulate strengthening stimuli through any of the exercises. Weakness in these muscles could leave the athlete vulnerable to inefficient energy transfer through the KC, and increase the load on the distal segments to achieve the desired output.31 Therefore, alternative exercises may need to be sought to sufficiently challenge these muscles. A standard press-up has been shown to elicit favourable activity in PM and AD,66 although prescribing countermovement, fall and jump push-up variations can also elicit high levels of PM activity.67 The latter may be favourable when focusing on potential pre-stretch applications as the throwing arm is cocked. Other open-chain exercises that could be employed to generate moderate-to-high LD activity include monster walks, plank on balance board, and the athletic position on a balance board.68
Study Limitations
There were some limitations to this study. Only the first set of the ATT was completed, consisting of bilateral movements being completed during repetitions. Sets two and three of the ATT when completed in full include a sustained hold element which may elicit greater muscle activity levels of glenohumeral and scapula muscles, as proposed by Wilk and colleagues.33 The inclusion of sustained holds has been reported to improve the muscular endurance of the glenohumeral and scapular muscles during the exercises, requiring additional neuromuscular challenge when completing the repetitions. Muscular hypertrophy can be positively impacted by incorporating sustained holds into exercise provision.69 However, Myers and colleagues29 found strength and endurance improvements in some participants when comparing scaption-focussed exercises from either the ATT or from traditional isotonic training exercises over a six-week period, although there were no differences identified between exercise groups. Therefore, while sustained holds were not a focus in this study, it is possible that desired strength and/or endurance development of key KC could be achieved using other approaches. The final exercises within the ATT, namely bicep curl, tricep extensions, wrist flexion/extension and supination/pronation movements seated on a stability ball were not investigated as part of this study. Due to the nature of overhead throwing, strengthening of the wrist and elbow is important for overhead athletes, and therefore exercises for these segments are part of the ATT.33 Therefore, it can be postulated that despite low BB activity found in the exercises investigated in this study, higher activity may be possible during bicep curl and tricep extension exercises which were excluded. However, the authors are satisfied that the findings of this study can provide key baseline information to therapists and rehabilitators when constructing prehabilitation and rehabilitation programs for overhead athletes. Finally, it is likely the study could be considered underpowered as a result of the participants numbers. However, the authors are satisfied that the study findings are consistent with other exploratory/descriptive studies in the field.24,37,43
Future Research
Future research should focus towards investigating muscle activity elicited during sets two and three of ATT where sustained holds are a key component to fully understand strength and/or endurance development potential of each exercise. In addition, investigating the load that is used within each exercise could be beneficial as greater loads may change the results. While maintaining the participant-orientated principles of the ATT, altering the weight of the dumbbells and the tension of the resistance tubing used across exercises could also be explored. This would provide further evidence-based recommendations to be proposed in line with KC principles and construction of prehabilitation and rehabilitation approaches for targeted strengthening and stability development of key muscles. In addition, exercises that challenge muscle activity across KC segments should be investigated for both healthy and injured populations. This could help identify muscle activity levels elicited for strengthening and stability purposes, particularly for engaging the core and lower limb segments, and provide evidence for both prehabilitative and rehabilitative approaches.
CONCLUSION
Few differences between groups were evident for mean muscle activity when performing exercises within The Advanced Throwers Ten, with higher AD and ISP activities in injured throwers evident across only five exercises. Only exercises performed in a prone position were found to provide sufficient challenge to elicit strengthening levels of activity for posterior deltoid, lower trapezius and infraspinatus, all of which were predominantly evident in injured throwers. However, the lack of strengthening stimuli generated in key muscles across KC segments is concerning, particularly in the core and lower body, and in muscles that aid energy transfer through the KC. These results provide key considerations for design of future rehabilitation programs and descriptive considerations for muscle activity levels in healthy and injured throwers during selected ATT program exercises.
Conflicts of Interest
The authors have no conflict of interest to declare.