INTRODUCTION
Anterior shoulder instability, frequently resulting from a Bankart lesion, is common among athletes participating in collision or contact sports, and often leads to substantial functional limitations and time lost from competition.1,2 In high school populations, the sport of football has one of the highest injury rates for shoulder dislocations, with anterior dislocations accounting for 97% of all shoulder dislocations (regardless of age).1,3 Collision positions, such as linebackers, are particularly vulnerable due to repetitive high-intensity tackling and forceful contact.1 In addition to participation in collision sports, other risk factors, including male sex, generalized joint hypermobility, and small glenoid index, are also associated with first-time shoulder dislocations.4
A Bankart lesion involves detachment of the anteroinferior labrum, often with associated injury to the glenohumeral ligaments, and typically occurs during anterior shoulder dislocation when the shoulder is positioned in abduction and external rotation.3,5,6 This mechanism results in excessive anterior translation of the humeral head and increased stress on the capsulolabral complex, potentially leading to recurrent instability and impaired ability to tolerate collision forces.3,6 A Buford complex is an anatomical variant characterized by a cord-like middle glenohumeral ligament and absence of the anterosuperior labrum, which occurs in approximately 1.2% to 7.5% of the general population.7 Although often considered a normal variant, the altered labral and capsuloligamentous morphology may affect load distribution across the anterior-superior glenoid and could contribute to instability when combined with traumatic labral injury.7 The coexistence of a Bankart lesion and a Buford Complex, as in this case, presents a unique clinical scenario that may influence rehabilitation considerations.
Surgical stabilization surgery is commonly recommended for young collision sport athletes with recurrent anterior instability because of their high risk of recurrence and the physical demands of their sport.1 Arthroscopic Bankart repair demonstrates favorable outcomes; however, rates of recurrent instability and variable timelines for return to sport (RTS) remain concerns in adolescent and contact-sport populations.2,4 A recent systematic review reported that approximately 81% of adolescent athletes returned to preinjury levels at a mean of 5.3 months following arthroscopic and open Bankart repair for traumatic anterior shoulder instability.2 These data highlight the need for rehabilitation strategies that safely restore strength, stability, and confidence in a time-efficient yet tissue-protective manner for collision sport athletes.
RTS testing for the upper extremity remains less standardized than for the lower extremity, particularly for collision-sport athletes whose demands differ from overhead throwers.8 Despite proposed frameworks distinguishing macrotraumatic (e.g. collision) and microtraumatic (e.g. throwing) shoulder injuries, clinicians frequently rely primarily on time-based criteria rather than performance-based assessments when clearing athletes for return to play.8,9 This gap highlights the need for rehabilitation approaches that not only restore range of motion and strength but also provide objective benchmarks of stability, resilience, and psychological readiness.
Early postoperative rehabilitation following Bankart repair is often challenged by restrictions on active motion and external loading, increasing the risk of muscle atrophy and delayed neuromuscular recovery. These challenges are particularly consequential for collision-sport athletes who must rapidly regain the ability to absorb and produce force. Blood flow restriction (BFR) training offers a potential strategy to mitigate muscle atrophy and support early neuromuscular adaptations by allowing low-load resistance exercise while respecting tissue-protective precautions.10–12 Although BFR is well studied in the lower extremity, its application in postoperative shoulder rehabilitation remains limited, and standardized protocols for upper extremity use are lacking.
Given these gaps, the purpose of this case report is to describe the integration of early-phase BFR within a structured, criterion-based rehabilitation program following arthroscopic Bankart repair in the presence of a Buford complex in a high school collision-sport athlete, and to highlight considerations for return-to-sport testing in this athlete.
CASE DESCRIPTION
The athlete was a 17-year-old right arm-dominant male high school football linebacker who presented with an eight-week history of anterior left shoulder pain. The initial injury occurred following a lateral traction-type force sustained in a collision with an opposing player. Immediately after the injury, he reported a sensation of transient shoulder dislocation followed by a spontaneous relocation. Over the remainder of the competitive season, he experienced three additional instability episodes yet continued to participate as a starting linebacker despite ongoing symptoms.
Following the season, the athlete sought an orthopedic surgical evaluation with the goal of playing competitive football at the collegiate level. Magnetic resonance arthrography revealed an anteroinferior labral tear consistent with a Bankart lesion, a Hill-Sachs lesion, and detachment of the superior labrum. The imaging report also described an anatomic variant consistent with a Buford complex, characterized by the absence of the anterosuperior labrum and a cord-like middle glenohumeral ligament.
Surgical Intervention
The athlete elected to undergo arthroscopic stabilization following recurrent anterior instability and confirmatory imaging findings. He underwent anterior Bankart repair, anterior capsulorrhaphy, labral debridement, subacromial decompression, distal clavicle excision, chondroplasty, and biceps tenotomy with tenodesis. Two #2 FiberWire sutures and two push-lock anchors were placed using standard arthroscopic technique.
Postoperatively, the athlete had to conform to the following instructions: 1) always remain in a sling and begin weaning from the sling at postoperative week 3, 2) avoid all active shoulder motion, and 3) initiate physical therapy within the first two weeks, respecting surgeon-directed precautions.
Examination
At the initial physical therapy evaluation, the athlete was 5’11" tall, weighed 203 lbs, and demonstrated a mesomorphic body type. He presented with the left upper extremity supported in a sling in accordance with postoperative precautions. Postural assessment revealed mild depression of the left shoulder. Systems review and medical screening were unremarkable.
Examination was performed in accordance with surgeon-directed precautions and published postoperative guidelines.13 The athlete demonstrated mild scapulothoracic hypomobility and a five-degree limitation in left elbow extension (lacking full extension to neutral). Neurovascular screening was normal, with intact sensation to light touch and minimal localized dysesthesia at well-healing incisions (3 portals: posterior, anterior rotator interval, and accessory anterior-superior portal). Local examination of the shoulder revealed minimal swelling and mild tenderness to palpation at the anterior deltoid and proximal long head of biceps region, with no signs of infection or wound complications.
Manual muscle testing of elbow extensors and all wrist movements demonstrated symmetrical strength bilaterally. Glenohumeral active motion and strength testing (as well as strength testing for elbow flexion and forearm pronation and supination) were deferred due to postoperative restrictions and tissue healing timeframe considerations.
Baseline grip strength measured via hand-held dynamometry exhibited 98 lbs in the right (dominant) upper extremity and 92 lbs in the left. Upper extremity girth measurements revealed mild asymmetry, with forearm circumference measuring 27.5 cm on the left and 29.5 cm on the right, and biceps circumference measuring 34.0 cm on the left and 34.5 cm on the right.
The athlete also completed the Western Ontario Shoulder Instability Index (WOSI) at initial evaluation, scoring 810 out of 2100 (38.6%), indicating a moderate-to-high perceived impact of shoulder instability on function and quality of life.
OUTCOME
Examination and Evaluation
Per the treating surgeon’s direction, a standardized protocol informed by published guidelines from the sports medicine division of Massachusetts General Hospital was selected and adapted by the physical therapist to progress the athlete toward collision sport readiness.13 Rehabilitation was organized into four phases: Protective (Phase I), Intermediate (Phase II), Advanced Strengthening (Phase III), and Return to Activity (Phase IV).
The athlete participated in 18 physical therapy sessions at a frequency of one to two sessions per week over an 18-week period. Formal physical therapy services concluded earlier than planned due to logistical and financial barriers. However, the athlete subsequently transitioned to independent and team-based training under the supervision of the athletic training and strength and conditioning staff, with guidance from the treating physical therapist. Beginning in Phase II, a structured weekly home exercise program was provided and regularly reviewed with both the athlete and athletic trainer to support progression outside the clinic.
Intervention
Phase I: Protective Phase (Weeks 0-6)
The primary goals of Phase I were protection of the surgical repair, pain and swelling control, early neuromuscular activation within postoperative restrictions, and optimization of adjacent joint mechanics and range of motion. The athlete was educated on strict adherence to sling immobilization, postoperative range-of-motion (ROM) limitations, and weight-bearing precautions to protect the repaired labral and capsuloligamentous tissues.
Interventions emphasized regional interdependence while respecting glenohumeral precautions. Grade I–II glenohumeral joint mobilizations and passive ROM were performed within surgeon-directed limits (≤90° scaption, ≤20° external rotation) to minimize postoperative stiffness. Manual techniques targeting adjacent non-surgical regions, including the thoracic spine, ribs, scapulothoracic joint, and elbow, were applied to optimize kinetic chain mechanics, improve proprioception at local tissues, and reduce compensatory loading of the healing shoulder. Dry needling was used to modulate muscle tone in the latissimus dorsi using pistoning techniques based on the trigger point model. Soft tissue mobilization techniques (perpendicular and parallel strumming, kneading, and ischemic pressure) were applied to the biceps, pectoralis major and minor, deltoid, latissimus dorsi, and upper and middle trapezius. Maitland-based joint mobilizations of the humeroulnar, humeroradial, and radioulnar joints were performed to improve forearm supination and elbow extension, progressing from grade II to grade III as tolerated.
Active exercise during this phase was limited to the elbow, wrist, and scapulothoracic musculature to prevent stiffness and promote foundational neuromuscular control. Submaximal glenohumeral isometrics and passive-assisted exercise were initiated at postoperative week 2. Upper body ergometer (UBE) activity was introduced in a bilateral, active-assisted manner at week 4, with resistance progressing from a rate of perceived exertion (RPE) of 2/10 to 5/10 by week 6. Glenohumeral active ROM, closed kinetic chain (CKC) exercise, and loaded elbow flexion or forearm supination were avoided due to the increased stresses on the surgical repair.13 To mitigate global deconditioning, a 10-minute core and lower extremity circuit was included during weeks 2–6.
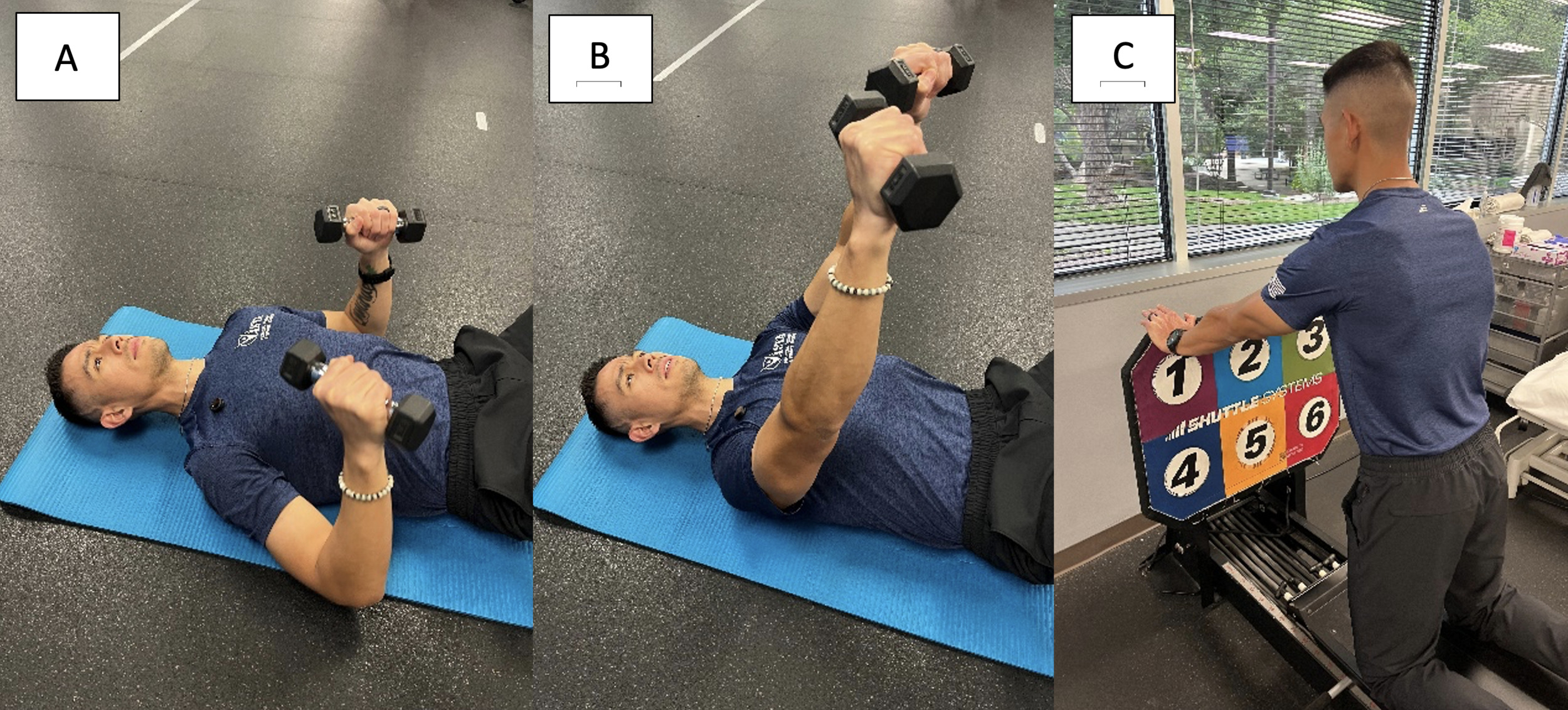
Toward the latter portion of Phase I (approximately weeks 4–6), select upper extremity exercises were introduced within restricted ranges of motion and with low external loads to emphasize neuromuscular activation rather than strength development, several of which were incorporated into the BFR training sessions. Exercises such as the floor press and triceps pulldown were selected because the floor constraint limited shoulder extension and anterior humeral translation during pressing tasks, while triceps pulldowns were performed with the shoulder maintained near neutral to minimize stress on the healing capsulolabral complex and the biceps tenodesis (Figure 1A & 1B). These exercises were also selected to provide controlled exposure to familiar movement patterns, facilitating adherence while reinforcing appropriate loading restrictions during early rehabilitation.
_floor_press_starting_position__(b)_floor_press_ending_position_.png)
BFR training was introduced at postoperative week 3 to promote neuromuscular and hypertrophic adaptations while minimizing mechanical load on healing tissues. Exercises were divided into a Day A and Day B format to improve patient engagement, reduce monotony when scheduling forced consecutive-day training, and promote comprehensive hypertrophic gains. A SmartCuffs 1.0 system with SD3 Series ultrasonic Doppler (SmartCuffs LLC, San Antonio, TX, USA) was used, with the cuff applied proximally on the arm. BFR sessions consisted of five low-load exercises per session, totaling 20–25 minutes of occlusion time, using a 30:15:15:15 repetition scheme and load progression guided by repetitions-in-reserve (RIR) and modified Borg rating of perceived exertion (RPE).14,15 The specific exercises performed with BFR are outlined in Table 1. Limb occlusion pressure (LOP) was measured at 170 mmHg and initiated at 50% LOP, progressing to 60% based on patient tolerance, consistent with published recommendations of 40–80% LOP for BFR training, with lower pressures favored in smaller limbs and conservative postoperative loading contexts. External loads were initiated at low intensity (~40% estimated 1RM), with intensity regulated and progressed using repetitions-in-reserve (RIR = 3) and perceived exertion (target RPE ≤7/10) to ensure an adequate training stimulus while minimizing excessive fatigue.15
At the conclusion of Phase I, the athlete demonstrated readiness to progress to Phase II due to meeting the following progression criteria without pain provocation: 90 degrees of passive shoulder elevation, 20 degrees of passive shoulder external and internal rotation in the scapular plane, and no complications.
Phase II: Intermediate Phase (Weeks 7-11)
The goals of Phase II were to restore full active glenohumeral range of motion, progress scapulothoracic and glenohumeral neuromuscular control, and initiate controlled loading while minimizing compensatory strategies. Passive range of motion was maintained throughout the phase, with active range of motion progressing to achieve full, pain-free motion by week 11. As soft tissue limitations became less prominent, manual soft tissue techniques described in Phase I were de-emphasized. Greater emphasis was placed on dynamic stability, including rhythmic stabilization using manual perturbations to facilitate isometric activation across multiple planes (flexion, abduction, and rotation) and body positions.
Isotonic strengthening was initiated using low loads and high repetition schemes to emphasize muscular endurance and motor control while limiting excessive joint stress. CKC exercise was introduced in low-load positions and progressed sequentially, beginning with quadruped activities. Progression of higher-demand CKC tasks (e.g., push-up patterns) was intentionally conservative due to the athlete’s history of recurrent instability and the presence of a Buford complex, which influenced tolerance to anterior and superior glenoid loading.7 Loading of the biceps, shoulder extensors, and external rotators was initially restricted during early Phase II (weeks 7–9), given the concomitant biceps tenodesis and ongoing tissue-healing constraints, with resisted biceps loading introduced gradually in late Phase II (weeks 9–12) as tissue tolerance improved. Repetitions-in-reserve (RIR) were used to guide intensity and prevent early fatigue-related compensations.
BFR training was continued during this phase to augment strength and hypertrophic adaptations, while higher mechanical loads and rapid force production movements remained contraindicated. As active motion and loading demands increased, BFR allowed progression of muscular capacity without exceeding tissue-healing constraints, serving as a transitional strategy between protected loading and conventional resistance training. BFR dosing and exercise selection were progressed in accordance with the parameters established in Phase I, with gradual transition toward conventional loading strategies as tolerance improved.
Interventions continued to emphasize regional interdependence, with Maitland-based mobilizations directed to the upper and mid-thoracic spine and ribs, and exercise strategies addressing thoracic mobility, trunk endurance, and proximal control to optimize force transfer and reduce stress on the healing glenohumeral joint. Neuromuscular re-education techniques targeting glenohumeral joint centration and coordinated movement patterns were progressed as tolerated across increasingly demanding positions.
Objective reassessment occurred in week 9 and included repeat strength testing and the introduction of the Posterior Shoulder Endurance Test (PSET), selected due to ongoing restrictions on higher-load and impact-based testing. Patient-reported outcomes were monitored throughout this phase, with the Western Ontario Shoulder Instability Index (WOSI) administered at regular intervals and the Shoulder Instability Return to Sport after Injury (SIRSI) initiated at week 9 to assess psychological readiness as physical demands increased.16,17
At the conclusion of Phase II, the athlete demonstrated no pain with passive shoulder elevation to 135 degrees, 50 degrees of passive shoulder external and internal rotation in the scapular plane, 45 degrees of passive shoulder external rotation at 90 degrees of abduction, and active shoulder forward elevation to 115 degrees. Although the athlete demonstrated greater available motion during assessment, passive range of motion exposure was intentionally constrained to remain within protocol-defined limits.13 Minimal compensatory movement patterns were observed, supporting advancement to Phase III.
Phase III: Advanced Strengthening Phase (Weeks 12-20)
The goals of Phase III were to maintain mobility gains, establish baseline RTS testing, and progress strength, endurance, and power through increasingly complex movement patterns relevant to collision sport demands. During this phase, intermittent increases in latissimus dorsi tone contributing to limitations in overhead motion were addressed with dry needling, including a session performed at week 17. Beginning in week 12, BFR training was intentionally discontinued in favor of traditional loading strategies, as the athlete demonstrated tolerance to active range of motion and resisted exercise beyond early tissue-protection constraints.18
Progressive strengthening emphasized horizontal pushing and pulling, diagonal movement patterns, and gradual exposure to higher-load tasks. Advancement of horizontal push and pull exercises was intentionally conservative due to the athlete’s history of recurrent instability and the presence of a Buford complex, which informed cautious progression of anterior and superior glenoid loading. Plyometric activity was introduced at week 13 using low-amplitude, bilateral tasks (e.g., push-up claps on wall, medicine ball chest passes to a rebounder, and tall kneeling shuttle push-ups [Figure 1C]), with progression guided by movement quality and symptom response.
At week 12, objective reassessment included repeat dynamometry, the PSET, and the addition of the Y-Balance Test–Upper Quarter (YBT-UQ) and Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST). Testing identified mild residual limitations in end-range shoulder mobility and external rotation strength, which informed continued emphasis on controlled loading and motor control during this phase.
Following surgeon clearance at week 12, the athlete began modified participation in team-based strength and conditioning sessions. Engagement with auxiliary rehabilitation sessions outside the clinic was variable due to scheduling constraints. Despite this, in-clinic performance demonstrated tolerance to progressive strengthening and bilateral plyometric activities without symptom provocation or instability events.
The final documented physical therapy session occurred at week 17. At that time, repeat functional testing and advanced bilateral strengthening tasks were performed. Further progression toward higher-load and unilateral plyometric activities was deferred due to inconsistent exposure to structured rehabilitation, with the goal of minimizing risk during ongoing tissue maturation.
Phase IV: Return to Activity Phase (Weeks 21+)
The goal of Phase IV was to transition the athlete toward unrestricted participation in football-related activities while maintaining strength, power, and endurance gains achieved during earlier phases. Formal physical therapy services concluded prior to completion of this phase; therefore, Phase IV progression occurred primarily through independent training and team-based strength and conditioning under the supervision of the athletic trainer and strength and conditioning staff.
At the conclusion of Phase III, the athlete demonstrated full pain-free range of motion, tolerance to progressive strengthening, and the ability to perform bilateral plyometric activities without symptom provocation. Based on these findings, continued progression toward higher-load, multiplanar strength and power tasks was recommended, including advancement of compound lifting patterns and graded progressive exposure to unilateral force production and absorption activities consistent with football demands.
Additional RTS testing, such as upper extremity endurance tasks, unilateral power assessments, and reactive or neurocognitive-based measures, was planned to further inform return-to-sport decision-making but was not completed under direct physical therapy supervision.
Outcomes
Over the course of rehabilitation, the athlete demonstrated progressive improvements in shoulder range of motion, strength, functional performance, and patient-reported outcomes
Range of Motion
Passive and active glenohumeral range of motion demonstrated progressive improvement across the rehabilitation period (Table 2). Passive motion increased throughout the protective and intermediate phases, with full or near-full passive range achieved by Week 12. Active range of motion progressed in accordance with postoperative restrictions, with full, pain-free active motion achieved by the conclusion of Phase II (Week 11) and maintained through later testing intervals.
Strength and Anthropometric Measures
Shoulder strength, assessed via manual muscle testing initially and later by hand-held dynamometry (ActivForce 2, ActivForce, USA), demonstrated progressive bilateral improvements across testing time points (Table 3). Early strength testing in protected ranges at Week 6 established baseline values, followed by measurable increases in shoulder flexion, external rotation, internal rotation, and horizontal plane strength by Weeks 9 and 12. Residual asymmetries persisted at later stages, particularly in external rotation strength at higher abduction angles. Upper extremity anthropometric measures demonstrated increases in biceps circumference over time with relatively stable forearm girth, while grip strength increased bilaterally with near-symmetrical values achieved by Week 12 (Table 3).
Functional Performance
Functional performance testing was initiated at Week 9 with the PSET and expanded at Week 12 to include the YBT-UQ and CKCUEST. As Table 4 indicates, performance improved between testing intervals, with increased endurance times and higher repetition counts observed at later assessments. Despite improvement, values at Week 12 remained below performance levels typically considered sufficient for unrestricted collision sport participation. Although medial reach distance increased between Weeks 12 and 15, decreases were observed in the superolateral and inferolateral directions, particularly on the involved side. Testing procedures were consistent across sessions and performed by the same examiner; however, these variations may reflect fatigue effects or differences in training load and scheduling, as sessions frequently occurred following team activities performed in a limited capacity per surgeon, athletic training, and physical therapy guidance. While directional variability was present within the YBT-UQ, improvements were observed in other functional performance measures, including the PSET and CKCUEST, supporting overall progression in functional capacity.
Patient-Reported Outcomes
Patient-reported outcome measures demonstrated consistent improvement throughout rehabilitation (Table 5). WOSI scores decreased over time, reflecting progressive improvements in shoulder-related quality of life, whereas SIRSI scores increased following initiation at week 9, indicating greater psychological readiness for return to sport.
At the final documented assessment (postoperative Week 15–17), the athlete reported no shoulder pain or instability symptoms and demonstrated tolerance to progressive strengthening and bilateral plyometric activities. Formal physical therapy services concluded at postoperative week 17 due to transportation limitations, at which time care transitioned to collaborative management with the athletic training staff and strength and conditioning coach. The athlete subsequently received medical clearance at Week 19, and athletic training staff reported continued offseason football participation without observed limitations or reported symptoms.
DISCUSSION
This case report describes the unique presentation, surgical treatment, postoperative rehabilitation, and RTS progression in a high school collision sport athlete following arthroscopic stabilization for recurrent anterior shoulder instability, including Bankart repair, capsulorrhaphy, and biceps tenodesis, in the presence of a Buford Complex. Current evidence regarding the use of BFR in postoperative upper extremity rehabilitation remains limited, particularly in the presence of anatomical variants such as a Buford complex. Additionally, RTS decision making commonly relies heavily on time-based progression rather than criterion-based functional performance measures.19 In this case, the athlete demonstrated favorable postoperative recovery and successfully completed a structured rehabilitation program incorporating BFR and functional testing to support readiness to return to sport at his prior level of participation.
BFR was utilized in this case as a strategy to bridge early protective phases of rehabilitation with subsequent loading phases. Several factors informed this decision, including the presence of a Buford complex, the substantial mechanical demands associated with the athlete’s position as a football linebacker, and developmental considerations common in adolescent athletes, such as elevated risk tolerance and motivation to return to sport. Collectively, these factors necessitated an intervention strategy that supported early muscle activation and muscular adaptation while maintaining appropriate protection of the surgical repair.
The presence of a Buford complex did not independently alter the surgical approach in this case; standard arthroscopic Bankart repair technique and anchor placement were utilized, and the variant was managed without modification to the capsulorrhaphy. However, given that its altered labral and capsuloligamentous morphology may influence load distribution and anterior-superior glenoid stability, particularly in the presence of concomitant traumatic labral injury, this anatomical variant was considered a relevant factor in guiding rehabilitation progression and early loading strategies.
Although the overall rehabilitation framework followed established postoperative guidelines for Bankart repair, the presence of the Buford complex informed a cautious progression of anterior loading during early strengthening, particularly in closed-chain tasks (e.g., push-up progressions).13 This was clinically relevant given the need to balance early progression toward sport-specific demands (e.g., blocking) with protection of the inherently vulnerable anterior glenohumeral structures. In this context, BFR provided a strategy to support early neuromuscular activation and strength development while minimizing mechanical stress on the healing capsulolabral complex.
Across the rehabilitation period before discontinuation of BFR at postoperative week 12, the athlete demonstrated measurable improvements in shoulder flexion strength, grip strength, upper extremity girth, and posterior shoulder endurance, alongside progressive improvements in range of motion and patient-reported outcomes. Upper arm circumference increased over time; however, similar bilateral changes were observed. As girth measurements may reflect multiple factors, including overall training adaptations and measurement variability, these findings should be interpreted cautiously and cannot be attributed directly to BFR. Rather, this case demonstrates that BFR was incorporated within a broad rehabilitation program during early post-operative recovery, during which a favorable clinical progression was observed.
Return-to-sport testing for the upper extremity remains less standardized than for the lower extremity, particularly for collision sport athletes. Wilk et al. emphasize that shoulder pathology and sport demands differ substantially between a macrotraumatic athlete (e.g., football linebackers) versus a microtraumatic athlete (e.g., baseball pitchers), necessitating that functional assessments should be selected with consideration to sport.8 In this case, functional tests such as the CKCUEST and YBT-UQ were selected to assess horizontal force acceptance, closed chain stability, and multi-planar control relevant to a football linebacker. Psychological readiness measures also contributed to RTS decision making, especially given the athlete’s limited verbalization of confidence and perceived readiness during the rehabilitative process.
This case highlights several clinically relevant considerations, including rehabilitation following a Bankart repair in the presence of a Buford complex, early integration of BFR in upper extremity postoperative care, and the use of criterion and time-based functional testing in a collision sport athlete. Planned later-stage assessments, including unilateral power and reactive testing, were not completed due to early discontinuation of formal physical therapy, but are presented as examples of how RTS evaluation may be further expanded in similar populations.
Limitations of this study include the single case design, which cannot determine cause-and-effect relationships, and being subject to selection bias. Additionally, late-stage testing was unable to be performed due to logistical barriers in transporting the athlete to physical therapy. Despite these limitations, this case provides a practical example of integrating BFR and functional performance testing within postoperative shoulder rehabilitation and supports further investigation into standardized upper extremity BFR protocols and collision sport-specific RTS frameworks.
CONCLUSION
This case report describes the rehabilitation of a high school collision sport athlete with a Buford complex anatomical variation following surgical repair of recurrent anterior shoulder instability. Early integration of BFR training was used to support neuromuscular activation and strength development while respecting postoperative loading constraints, providing a practical example of BFR application in upper extremity rehabilitation. Although early discharge limited completion of later-stage RTS testing, this case illustrates the use of time and criterion-based functional and psychological measures to guide progression toward return to the demands of a collision sport. Further research is needed to establish standardized upper extremity BFR protocols and validated RTS testing frameworks for athletes participating in high-force impact contact sports.
Conflicts of Interest
The authors declare that they have no conflicts of interest related to this study.