INTRODUCTION
Basketball is a contact sport that involves frequent jump landings, sudden changes of direction, and physical contact, which all contribute to the potential for injuries, including ankle sprains, lower back pain, and knee disorders. Dick et al.1 reported an injury incidence of 9.9 per 1,000 athlete-exposures in American collegiate basketball. They concluded that the sport’s inherent high-impact movements were the primary cause of injuries. Recently, movement quality has been reported to be strongly associated with injury risk,2–5 and the Functional Movement ScreenTM (FMSTM) has attracted attention as a simple method of screening. The FMSTM comprises seven components with a maximum total score of 21. Scores of ≤14 have been widely cited as a threshold for increased injury risk.3,6 However, in the meta-analysis by Moran et al. ,6 the sensitivity and specificity of this threshold was shown to vary considerably depending on the sport and sample characteristics, suggesting that reliance on the total score alone has limitations. Although the conventional total score has been regarded as a general indicator of injury risk across sports, it may overlook sport-specific demands. A weighted total score, constructed by optimally weighting individual FMSTM items, could provide a screening model that better reflects the unique movement characteristics and injury risks of basketball.
In fact, in a study of male high school football, lacrosse, and baseball players, Lisman et al.7 examined the association between FMS™ composite and individual task scores and lower extremity injury occurrence, finding that neither the composite score nor individual task scores demonstrated a significant association with injury risk. These findings highlight the population-specific limitations of FMS™-based injury prediction and suggest that sport-specific analyses may be required. Furthermore, in a large-scale cohort of US military recruits, Bushman et al.8 concluded that the total FMSTM score did not relate to prediction of stress fractures and that comprehensive assessments incorporating individual movement patterns, muscular function, and bone density were required. In a study of junior basketball and soccer players in Taiwan, Chang et al.9 demonstrated that the total FMS™ score was associated with sport injury occurrence over a one-year period. However, their study included a mixed-sport population and did not examine sport-specific injury risk profiles or the predictive utility of individual task scores in detail. Furthermore, a comprehensive analysis of the predictive utility of all seven FMS™ components within basketball players alone was not conducted.
There are few prospective studies using the FMSTM, with even fewer utilizing individual analyses. Indeed, many previous studies have based their analysis solely on the total FMSTM scores, and few have explored the characteristics of each task, associations with injury sites, or relationships with sport-specific demands in detail. In addition to the total score, incorporating a screening of the movement characteristics evaluated by each individual FMSTM task could enable more practical risk stratification. Each FMS™ task reflects a distinct movement chain and stability strategy. This distinction is particularly relevant in sports such as basketball, where athletes repeatedly perform complex movements under loaded conditions. For example, the DS component assesses the coordinated mobility of the hip, knee, and ankle joints along with core stability. The HS component requires control of the pelvis and trunk and dissociative movement of the lower limbs during single-leg stance. Meanwhile, the ILL component demands dynamic sagittal plane stability and joint flexibility. Each of these three tasks—the DS, HS, and ILL—may reveal early signs of injury risk through breakdowns in their respective movement chains.10
According to Kiesel et al.3 professional football players with a total FMS™ score of ≤14 were significantly more likely to be sidelined during the season than those with higher scores. Gribble et al.11 pointed out a relationship between instability in loaded positions and ankle sprain history, suggesting that single-leg loaded tasks within the FMSTM may be useful for identifying injuries in specific regions. Furthermore, Schneiders et al.12 reported that individuals in a young, active population demonstrated variability in individual FMS™ component scores, with certain tasks showing associations with functional movement capacity that may relate to injury susceptibility.
As such, rather than relying solely on the total score, analysis based on each task’s movement characteristics may provide important insights into site-specific injury risk association and screening tailored to each sport’s characteristics. Although epidemiological studies on injuries among high school athletes have been increasing in Japan, there are limited prospective studies using the FMSTM, and individual analyses are not yet sufficient. Basketball is a sport wherein specialization often begins at a relatively young age, and the development of injury prevention strategies is directly linked to career longevity and performance maintenance. Therefore, the present study aimed to prospectively investigate the relationship between individual FMSTM scores and sports injury incidence among university basketball players over the course of one year. In addition, the applicability of the conventional total score threshold of ≤14 was evaluated, and the screening utility of individual and total FMS™ tasks was compared.
METHODS
The study period was set at 12 months (April 2023 to March 2024). The FMS™ was administered at baseline prior to the start of the competitive season before any structured team training had commenced, and injury occurrence was tracked throughout the subsequent competitive season. This study was approved by the institutional review board (approval number: 18638-210630) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants and their guardians.
Participants and Procedures
A research briefing was provided to athletes with over five years of basketball experience who were affiliated with the Niigata Basketball Association. At baseline, 92 athletes consented to participate in the study. However, seven were excluded based on the following criteria: (1) history of trauma or surgery without having returned to sport at the time of baseline assessment, (2) central nervous system or cardiovascular disorders, and (3) switch to another sport during the study period. The final analytic sample included 85 athletes.
Height, weight, and playing experience were self-reported by each participant using a standardized questionnaire administered at baseline. Using the standard protocol proposed by Cook et al.,2 the following FMSTM components were scored from 0 to 3 points each (total score range: 0–21): DS, HS, ILL, Shoulder Mobility (SM), Active Straight-Leg Raise (ASLR), Trunk Stability Push-Up (TSPU), and Rotary Stability (RS). Two physiotherapists independently performed the FMS™ screenings and recorded scores. When scoring disagreements occurred, a third physiotherapist was consulted on the same day, and the movement was re-evaluated through group discussion. Where necessary, scores were revised based on consensus. The kappa coefficient between the initial and finalized scores was calculated to verify the reliability of this scoring procedure, yielding a value of 0.83, which was interpreted as “almost perfect agreement.”
A sports injury was defined as “a medical condition resulting in restriction from participation in training or competition for more than seven days,” in accordance with the sports injury classification of Fuller et al.13 In addition to the time-loss definition, injuries were further classified based on mechanism and type. Injury mechanism was categorized as contact or non-contact according to whether the injury resulted from direct external contact with another player or object. Injury type was classified as acute or overuse based on clinical diagnosis, where acute injuries were defined as those resulting from a specific identifiable event, and overuse injuries were defined as those developing gradually without a single identifiable cause. Injuries and conditions were diagnosed either by a physician upon clinical consultation or by an accompanying physiotherapist. Reports were submitted to the study supervisor within one week of the incident. Moreover, weekly reports were prepared by the attending physiotherapist to document each athlete’s match and training participation. These data were entered into a secure cloud-based research system and included details, including injury date, diagnosis, duration of time lost, treatment content, and classification of clinical severity.
Statistical Analysis
All statistical analyses were performed using Python (version 3.10; Python Software Foundation, Wilmington, DE, USA) along with its primary library, pandas. Participants were classified into two groups based on injury occurrence during the follow-up period: an injury group (those who sustained at least one time-loss injury) and a non-injury group (those who remained injury-free). Normality of the data distribution was assessed using the Shapiro-Wilk test, and since the assumption of normality was not met for the variables, the Mann–Whitney U test was used for between-group comparisons. Receiver operating characteristic (ROC) curves were generated for each FMS™ component, and the maximum Youden index was used to determine the cutoff values. Logistic regression analysis was also extended to develop a weighted total score model based on optimal individual coefficients, enabling evaluation of sport-specific predictive accuracy. Meanwhile, sex, playing experience, height, and weight were included as covariates to control for potential confounding effects. The significance level was set at 5%, and the effect sizes (Cohen’s d or r) were calculated, with values of 0.2, 0.5, and 0.8 interpreted as small, medium, and large effects, respectively. An a priori power analysis was conducted using G*Power 3.1. The required sample size was calculated to be 64, based on the effect size of 0.8 reported by Chorba et al.4 with α = 0.05 and β = 0.20. Therefore, the inclusion of 85 participants in the present study was determined to provide sufficient statistical power. This manuscript was prepared in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement to ensure transparent and comprehensive reporting of this prospective cohort study.
RESULTS
The final analytic sample consisted of 85 athletes (42 males and 43 females; age 20.2 ± 2.1 years). Male participants had a mean height and weight of 178.4 ± 6.8 cm and 70.2 ± 7.1 kg, respectively. Female participants had a mean height and weight of 166.9 ± 5.7 cm and 60.7 ± 5.9 kg, respectively. The average duration of playing experience across all participants was 5.3 ± 1.2 years. No significant difference was observed in the total FMSTM score between male and female athletes (males: 15.4 ± 2.3; females: 15.2 ± 2.4; p = 0.82).
During the one-year follow-up period, 35 sports injuries were recorded, including 11 lateral ankle sprains, nine cases of low back pain, six hamstring strains, four cases of knee pain, one concussion, two finger ligament injuries, and two thigh muscle contusions. Of these, 24 were classified as non-contact injuries and 11 as contact injuries. Additionally, 22 injuries were categorized as acute, whereas 13 were classified as overuse conditions. Sixteen athletes (18.8%) were classified into the injury group. The median number of cumulative days missed because of injury was 11 days (range: 8–23 days).
No significant difference was observed in the total FMSTM score between the injury and noninjury groups (15.1 ± 2.4 vs 15.4 ± 2.2, p = 0.64). The conventional total FMSTM cut-off score (≤14) was not associated with subsequent injury occurrence (AUC = 0.52, p = 0.84), with a sensitivity of 0.38 and specificity of 0.61, suggesting limited clinical utility. Group comparisons of individual FMS™ task scores revealed that the injury group demonstrated significantly lower scores in the DS and HS compared with the non-injury group (DS: 2.1 ± 0.7 vs 2.5 ± 0.6, p = 0.037, effect size r = 0.225; HS: 2.0 ± 0.7 vs 2.4 ± 0.6, p = 0.018, r = 0.251). No significant differences were observed in the remaining FMS™ components, including ILL, SM, ASLR, TSPU, and RS (all p > 0.05). Effect sizes for these variables were small, indicating limited practical differences between groups. (Table 1)
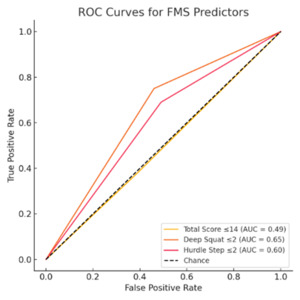
For a cut-off score of ≤2 in the DS, the sensitivity and specificity were 0.75 and 0.54, respectively. Meanwhile, for a cut-off score of ≤2 in the HS, the sensitivity and specificity were 0.69 and 0.51, respectively. (Figure 1)
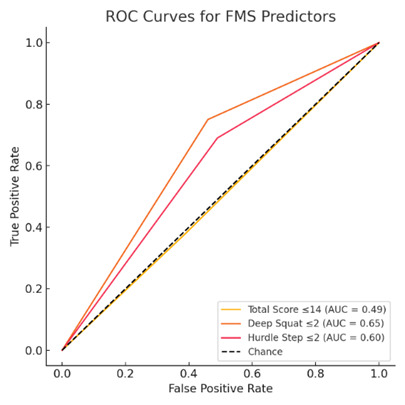
The figure shows the ROC curves for three FMSTM-based associative indicators of sports injury: total score ≤14, DS ≤2, and HS ≤2. The horizontal axis represents the false positive rate (1 – specificity), whereas the vertical axis represents the true positive rate (sensitivity). The 45° dashed line indicates the reference line for random associative. The DS and HS demonstrated higher associative accuracy (AUC) than the total score.
Logistic regression analysis showed that athletes scoring ≤2 on the DS demonstrated a significantly increased risk of injury (OR = 3.47, 95% CI [1.02–11.83], p = 0.047). Similarly, those scoring ≤2 on the HS had an increased risk, although this did not reach statistical significance in the unadjusted model (OR = 2.26, 95% CI [0.71–7.21], p = 0.166). When both variables were entered into the model simultaneously, the model fit was χ²(2) = 12.2, p = 0.002, with a Nagelkerke R² of 0.21, and it correctly classified 72% of injury cases. By contrast, the model using a total FMSTM score of ≤14 as the explanatory variable had a Nagelkerke R² of only 0.04. A weighted logistic regression model incorporating all seven FMSTM items improved discrimination (AUC = 0.75) compared with the conventional total score, although the predictive contributions of individual items varied.
DISCUSSION
This study contributes incrementally beyond previous literature by focusing on university basketball players, using a one-year prospective design, and incorporating individual analyses across all FMSTM tasks. These aspects address limitations in prior studies that primarily relied on total scores, shorter follow-up durations, or restricted populations.
Low scores on the DS and HS were significantly associated with injury occurrence among university basketball players over a 1-year period, whereas the conventional total FMS™ score of ≤14 demonstrated limited predictive ability. This finding suggests the clinical utility of screening focusing on individual task scores rather than the composite score alone. In particular, the DS and HS require coordinated mobility of the hip, pelvis, and trunk under bilateral loaded conditions, which may explain their stronger association with injury in this cohort. Although the ILL similarly demands lower limb coordination and stability under loaded conditions, it was not significantly associated with injury occurrence in the present study. This discrepancy may reflect the differing loading demands between tasks: the DS and HS impose bilateral loaded positions, whereas the ILL captures unilateral dynamic stability. Given that the most prevalent injuries in this cohort were lateral ankle sprains and low back pain, the movement patterns assessed by the DS and HS may more closely reflect the injury mechanisms characteristic of basketball than those captured by the ILL. Dysfunctions detected in the DS and HS may contribute to ankle sprains or lumbar injuries by disrupting dynamic lower limb alignment. The predominance of non-contact and acute injuries observed in this cohort further suggests that movement-related factors play a substantial role in injury occurrence, supporting the clinical relevance of the FMS™ as a pre-season screening tool for identifying athletes at risk.
In this cohort of collegiate basketball players, the conventional FMS™ total score cut-off (≤14) did not demonstrate predictive validity for sports injury, which aligns with previous reports.6,8 By contrast, deficits in specific tasks—particularly the DS—were associated with approximately a threefold higher risk of injury (OR = 3.47), whereas the HS demonstrated an approximately twofold increased risk (OR = 2.26) that did not reach statistical significance in the logistic regression model, highlighting the importance of task-specific screening for lower limb stability. The weighted individual model yielded a higher AUC (0.75) than the conventional score, suggesting potential to improve predictive accuracy, but this requires validation in larger samples. Taken together, these findings indicate that individual FMS™ scores may offer greater clinical utility than the total score, and focusing on DS and HS may be a practical approach for pre-season screening.
Previous studies have also highlighted the limitations of relying solely on the total FMS™ score. For example, Bushman et al.8 demonstrated in a large cohort of active military men that while a composite score of ≤14 was associated with injury risk, the authors noted that comprehensive assessments incorporating individual movement patterns may provide greater practical utility than the total score alone. Building upon these insights, the present prospective study demonstrated that individual task scores—specifically the DS and HS—were more strongly associated with injury occurrence than the total score in university basketball players.
Consistent with the present study, previous research has reported similar findings. Kiesel et al.3 demonstrated that a total FMS™ score of ≤14 could serve as a predictor of in-season injuries among National Football League players. However, larger cohort studies, including Bushman et al.8 found that the predictive utility of the total score alone was limited, and that scores on specific individual tasks may serve as more practical indicators of injury risk. Furthermore, low DS and HS scores have been associated with medial knee collapse, pelvic drop, or impaired single-leg stability, all of which are recognized as movement-related risk factors for anterior cruciate ligament injuries and ankle sprains. The findings of the present study support these observations and suggest that similar movement-related mechanisms may contribute to injury occurrence in basketball players.
From a clinical perspective, the DS and HS require no specialized equipment and can be performed in a short amount of time, making them practical pre-season screening tools. These findings suggest that DS and HS can be used as practical tools to identify athletes at higher risk of injury during pre-season screening. Athletes demonstrating low scores (≤2) on these tasks may require targeted interventions focusing on movement quality. Specifically, deficits observed during the DS may indicate limited ankle dorsiflexion, hip mobility, or trunk control, whereas poor performance in the HS may reflect impaired single-leg stability and neuromuscular control. Based on these task-specific deficits, clinicians can implement targeted exercise programs, such as hip–core strengthening, single-leg balance training, and mobility exercises. Therefore, incorporating DS and HS into routine screening may facilitate early identification of high-risk athletes and enable the design of individualized injury prevention strategies. Specific recommendations could include hip-hinge drills and single-leg squats to enhance the closed-chain lower limb function, “dead bug” and “bird dog” exercises to improve trunk rotation stability, and mobility exercises (e.g., ankle dorsiflexion and hip flexor stretches). Indeed, previous research has demonstrated that FMS™ screening-based risk stratification, such as that proposed by Lehr et al.14 may facilitate the identification of athletes at elevated risk for noncontact lower extremity injury, supporting the clinical value of incorporating individual task scores into pre-season screening protocols.
Individual FMSTM scores may also contribute to the development of individualized strategies based on the nature of injury sites. For example, compensatory movements (e.g., trunk flexion or anterior pelvic tilt) during the DS task should be observed for athletes with a history of low back pain. Meanwhile, foot stability and ankle joint range of motion during the HS task should be examined for those with a history of ankle sprain. Such an approach may lead to the design of more precise and effective injury prevention strategies.
This study has several limitations that should be acknowledged: (1) the playing experience varied among participants; (2) injury classification and incidence were based on time-loss criteria without incorporating athlete-exposure data, which is considered a standard approach in sports epidemiology. Because detailed exposure time for each athlete (e.g., training and match hours) was not available via the data collection system, the authors were unable to calculate injury incidence per athlete-exposure. This limitation may affect the comparability of these findings with previous epidemiological studies; (3) this study was an observational study with no intervention, limiting causal inference; (4) the biomechanical basis of low FMSTM scores remains unclear because of the lack of strength testing or three-dimensional motion analysis; and (5) the sample sizes for male (n = 42) and female (n = 43) athletes might have been insufficient to ensure adequate power for sex-specific analyses. Future studies should investigate the associations between FMSTM tasks and hip strategies, knee valgus moments, and ankle pronation angles during three-dimensional movements. Moreover, they should test the effectiveness of preventive interventions via randomized controlled trials targeting low scorers.
Finally, the value of prospective research is self-evident as it is essential for building practical screening models. As data accumulation continues, more sensitive and practical screening models tailored to specific sporting demands will become possible. To that end, collaboration among researchers and the importance of continuous, multicenter data collection will only grow. Maintaining the FMSTM as a screening framework while optimizing item weights for sport-specific demands may improve discriminatory performance compared with the conventional total score.
CONCLUSION
The results of this prospective cohort study demonstrated that low scores on the DS and HS tasks predicted a higher likelihood of injury in collegiate basketball players, whereas the total FMS™ composite score showed limited utility. These findings underscore the importance of focusing on individual task characteristics that reflect the complex, sport-specific demands of basketball. Incorporating individual task assessment into routine pre-season screening may enable earlier identification of high-risk athletes and the implementation of tailored corrective strategies. Future research should further refine associative models through larger, multicenter cohorts and explore the effectiveness of targeted interventions designed for athletes with low task scores. A sport-tailored, item-weighted FMSTM appears more discriminative than the conventional total score while larger multi-team and multi-sport validation is warranted.
CONFLICTS OF INTEREST
The authors have no conflicts of interest.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
ACKNOWLEDGEMENTS
The authors would like to thank all the athletes and staff who participated in this study for their valuable cooperation.