INTRODUCTION
Evidence suggests that return to sport or competition is a significant milestone of anterior cruciate ligament reconstruction (ACLR) rehabilitation.1–3 Neuromuscular control, including muscle activation patterns, is considered an important component of functional recovery after ACLR.4,5 A previous study reported altered quadriceps and hamstring EMG activity following ACLR during isolated or controlled tasks.6 While frontal-plane knee valgus has historically been associated with ACL injury risk, recent evidence suggests that this relationship is complex and not necessarily causal.7 Contemporary perspectives emphasize the contribution of proximal neuromuscular control strategies to lower-limb movement strategies with ACL injury risk, including hip and trunk muscle activation.4,8 Non-contact ACL injuries frequently occur during dynamic movements such as landing, cutting, or pivoting, which often involve single-leg loading.9,10 During jumping and landing tasks, the ankle joint and triceps surae play a major role in force generation and absorption, contributing substantially to lower-limb kinetics and may contribute to knee joint loading.11–13 Alterations in triceps surae EMG activity may therefore represent an understudied aspect of neuromuscular function following ACLR.12–15 However, the role of triceps surae EMG activity during functional single-leg tasks after ACLR remains insufficiently investigated.16–18 While neuromuscular activation (including quadriceps pre-activation) may precede initial contact, the foot–ankle complex is the first mechanical interface with the ground during landing.17 Biomechanical evidence suggests that gastrocnemius loading may increase anterior tibial shear, whereas soleus loading may contribute to posterior tibial shear, which could be protective for the ACL.12 Previous studies have explored triceps surae function after ACLR using more comprehensive biomechanical approaches, including EMG-informed musculoskeletal modeling. However, differences in methodology and outcome measures limit direct comparison, and the role of triceps surae EMG activity during functional tasks remains understudied.16,19
Because the role of the triceps surae during functional single-leg tasks after ACLR remains insufficiently understood, the primary objective of this study was to compare triceps surae EMG activity during single-leg jumping tasks between individuals who had undergone ACLR and healthy controls. The secondary objective was to examine whether any observed neuromuscular differences were present bilaterally within the ACLR group. It was hypothesized that individuals after ACLR would demonstrate lower triceps surae EMG activity compared with healthy controls and that any observed differences would also be present in the non-operated limb.
MATERIALS AND METHODS
Study design
This case-control study received ethical approval (2023-A01099-34) by the local ethics committee, conducted in agreement with the Declaration of Helsinki, and all participants gave written informed consent. Subjects from both groups were informed of the protocol and measures recorded. Anthropometric, surgical, and sports-related data from all participants before inclusion in the study were recorded (i.e., gender, age, body mass, height, graft type, date of surgery, Tegner activity score before ACL injury).11
Participants
This study included twelve recreational athletes who had undergone an ACLR and nine healthy control individuals. Athletes with ACLR were recruited from patients going through their rehabilitation program in a single rehabilitation center. All surgeries were performed by three experienced surgeons from the same orthopaedic clinic following a standardized ACLR surgical protocol, in order to limit inter-surgeon variability. Healthy subjects were selected among healthcare professionals from the clinic and rehabilitation center with similar sports’ activity levels. Participants were included in the ACLR group if: they had undergone an ACLR surgery with hamstring autograft at least three months prior to the initial assessment, they were aged between 18 and 50 years old, and had a body mass index < 30 kg.m-2, their activity level before ACL injury was > 7 on the Tegner activity score, and they had completed the return to running criteria20 and resumed running without symptoms (full knee range of motion; pain <2 on visual analogue scale; knee extensor and flexor limb symmetry index (LSI) >70% on isokinetic dynamometry at 60°.s-1; and single-leg hop for distance LSI > 70%). All the ACLR patients completed the International Knee Documentation Subjective questionnaire (IKDC), and the Anterior Cruciate Ligament-Return to Sport after Injury (ACL-RSI) to assess their ability to perform jumping tasks of the study. Scores below 55 on the ACL-RSI and below 80 on the IKDC were considered as an exclusion criterion.21 Participants with meniscal repair or meniscectomy were eligible for inclusion.11,22 Limb dominance (preferred kicking leg) was recorded for all participants.
Exclusion criteria were a history of prior ACL injury or ACLR in the contralateral limb, previous major injury or surgery to either lower limb, associated multiligament knee injury, osteochondral lesion, or any condition preventing safe performance of the jumping tasks.
Maximal Isometric Torque
Subjects performed a 7-minute warm-up on a cycle ergometer.11 Following the warm-up, the EMG electrodes were placed over the soleus, gastrocnemius medialis, and gastrocnemius lateralis according to Surface Electromyography for the Non-Invasive Assessment of Muscles (SENIAM) recommendations.23 Maximal voluntary isometric contractions (MVICs) were then performed to normalize EMG amplitude for each muscle.
The MVIC assessment was done with the subject in seated position, the knee flexed at 90° and braced against a fixed bar, and with the foot at 0° of dorsiflexion, resting on a flat surface. The individuals were instructed to perform a maximal plantarflexion effort by pushing the forefoot against the ground as hard as possible against the ground and to maintain the contraction for 6 seconds. Three measurements were taken for each side, with 30 seconds rest between each test.11
Jumping tasks
After the MVIC EMG muscle activity assessment, each participant performed four Single Legged Counter Movement Jump (SLCMJ) and four Single Leg Drop Jump (SLDL) (both tasks were performed bilaterally in a random order) following practice jumping tasks before EMG muscle activity recording.11 The order of the tasks (SLCMJ and SLDJ) was randomized for each participant using a simple randomization procedure.
For the SLCMJ, the participants were instructed to keep the hands on the hips and jump on one leg as high as possible while also landing on the same leg as close as possible to the point of takeoff. For the SLDJ, the participants were instructed to jump from a 15 cm high platform and perform a second jump as quickly as possible after landing, again keeping the hands on the hips. A 30-second rest was given between each trial, while 3 minutes rest was given between tasks.11 Trials were discarded if participants lost their balance, touched the ground with the contralateral foot, or released their hands from the hips. Discarded trials were repeated until four valid trials were obtained for each limb and task.
Outcome measures
All raw EMG data was transferred to the FREEEmg software (BTS Bioengineering® version 2.9.41.0) for processing. Each signal (MVIC and jumping task trials) was filtered with a Lowpass filter (20Hz) and processed mathematically using Root Mean Square (RMS). For the MVIC data, the maximum EMG value of the three measurements after RMS processing was retained for each evaluated muscle (soleus, gastrocnemius medialis and gastrocnemius lateralis) for both the operated/dominant and non-operated/non-dominant leg. The EMG signal of each jumping measurement was then normalized to the MVIC recorded value of the corresponding muscle. The data were expressed as a percentage of the MVIC.
For the SLCMJ, the outcome used for analysis was the peak normalized EMG amplitude during the propulsion (take-off) phase, corresponding to the period of maximal concentric demand on the triceps surae. Jumping phases were visually identified and synchronized with EMG recordings to ensure that the extracted peak EMG occurred during the propulsion phase. The mean of the four trials was retained for analysis.
For the SLDJ, EMG activity was quantified using a fixed 0.5-s time window preceding the peak EMG amplitude observed during the jump, representing the propulsion phase following ground contact.
Statistical Analysis
The normality of the anthropometric data was tested using a Shapiro-Wilk test and showed that it did not follow a normal distribution for the age, height, weight and Tegner activity Score. The between-group differences for height, weight, and age were tested using a Wilcoxon-Mann-Whitney test.
The normality of the EMG data corresponding to the analyzed variables was tested, and analyses were performed using the students T-test or the Wilcoxon-Mann Whitney test if data not normally distributed. The level of significance was set at α = 0.05.
RESULTS
Demographic and baseline characteristics
A summary of baseline data and the between-group differences are presented in Table 1. No statistically significant differences were observed between the two groups.
The time since surgery for the ACLR group ranged from 4.9 to 6.3 months postoperatively (mean: 5.6 ± 0.7 months). A meniscus repair was conducted in two individuals following the ACLR. Table 2 presents the descriptive statistics and distribution of electromyographic activation during the SLCMJ and SLL tasks for both groups.
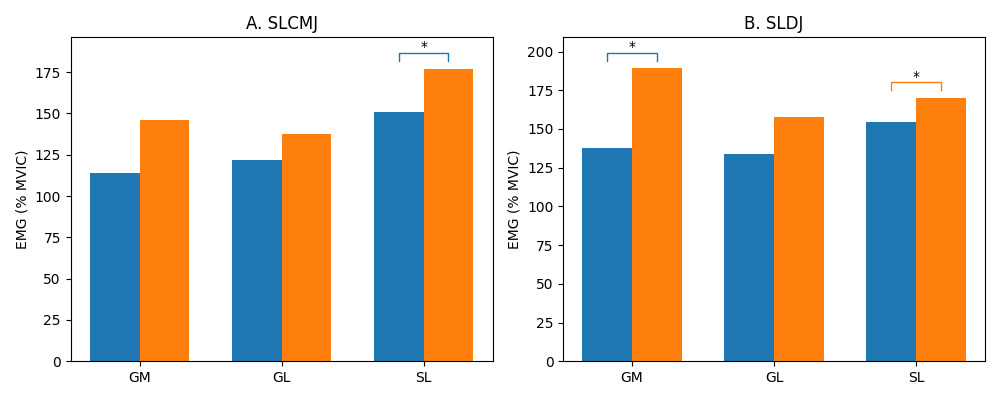
The EMG activity of the triceps surae during both tasks is illustrated in Figure 1. The between-group and between-limb differences in EMG data are presented in Table 3.
_activity_of_the_triceps_surae_muscles_(gm__gl__and_soleus)__expressed_as_a.png)
For the SLCMJ test, between-group differences showed no statistically significant differences for the gastrocnemius medialis (GM: 113.9% ± 27.7 vs 146.0% ± 27.0, p = 0.35) or gastrocnemius lateralis (GL: 121.6% ± 9.9 vs 137.5% ± 56.7, p = 0.38). However, soleus (SL) activity was significantly lower in the ACLR group compared to controls (150.6% ± 31.2 vs 176.7% ± 14.1, p < 0.01). No statistically significant between-limb differences were observed within the ACLR group for any muscle (all p > 0.05).
For the SLDJ test, GM activity was significantly lower in the ACLR group compared to controls (137.4% ± 29.3 vs 170.1% ± 12.9, p < 0.01). GL activity was also lower in the ACLR group, although this difference did not reach statistical significance (134.0% ± 22.3 vs 157.8% ± 25.4, p = 0.06). Similarly, soleus activity was significantly lower in the ACLR group (154.7% ± 39.2 vs 189.2% ± 25.9, p = 0.02). No significant between-limb differences were observed for any muscle in the SLDJ task (all p > 0.05).
Overall, soleus activity was consistently lower in the ACLR group across both tasks, while GM differences were task-specific and reached a statistically significant difference only during the SLDJ.
DISCUSSION
The aim of this study was to compare triceps surae EMG activity during two single-leg jumping tasks between individuals after ACLR and healthy controls. The main finding is that triceps surae EMG activity was generally lower in the ACLR group, with the most consistent and significant differences observed for the soleus across both tasks, and for the gastrocnemius medialis during the SLDJ.
The most consistent finding of this study concerns the soleus muscle, which showed significantly lower EMG activity in the ACLR group across both tasks. Clinically, these findings may reflect a reduced contribution of the soleus during single-leg function. Importantly, this alteration appeared to be bilateral and muscle-specific, as it was not consistently observed for both heads of the gastrocnemius. From a biomechanical perspective, soleus activation may contribute to posterior tibial shear, which has been suggested to play a protective role for the ACL.24 In addition, the soleus may contribute to lower-limb control during stretch-shortening cycle activities. However, because joint kinetics were not assessed in the present study, the mechanical implications of lower soleus EMG activity remain uncertain.12,24 A reduced soleus EMG activity, as observed in this study, may therefore indicate a diminished contribution of the ankle–foot complex during single-leg functional tasks in individuals after ACLR. However, because joint kinetics and injury outcomes were not assessed, the mechanical and clinical implications of these neuromuscular differences remain to be established. Whether these alterations persist and are associated with return-to-sport outcomes or secondary ACL injury risk should be investigated in future studies.
Regarding the gastrocnemius medialis, the results were more task specific. GM EMG activity was significantly lower in the ACLR group during the SLDJ task, but not during the SLCMJ. This suggests that GM involvement may be more dependent on task demands, particularly during rapid stretch-shortening cycle activities involving high loading rates. In contrast, GL activity did not show significant between-group differences in either task, indicating a less prominent or more variable role in these functional conditions. These findings highlight a muscle-specific adaptation within the triceps surae following ACLR, supporting the idea that neuromuscular alterations may not be uniformly distributed across muscles.
Overall, triceps surae EMG activity tended to be lower in the ACLR group compared with controls. However, these findings should be interpreted with caution, as EMG amplitude does not directly reflect muscle force production.12 Measures of triceps surae strength and external kinetics (e.g., ground reaction forces) were not assessed, which limits the ability to determine the mechanical relevance of the observed neuromuscular differences. The EMG–force relationship is complex and influenced by multiple physiological and methodological factors.25 Therefore, concurrent assessment of muscle strength and external loading would be necessary to better understand the functional implications of these findings.
No significant differences were observed between the operated and non-operated limbs within the ACLR group. These findings support the presence of bilateral neuromuscular alterations following ACL injury and reconstruction.26,27 Therefore, the non-operated limb should not be assumed to be unaffected, and bilateral assessment remains warranted. This observation is consistent with the hypothesis of central neuromuscular adaptations following ACL injury, which may affect motor control strategies in both limbs.28 In this context, within-subject approaches such as limb symmetry indices may provide more meaningful insights than comparisons with normative values, especially given the high inter-individual variability of EMG data.
Previous studies have also highlighted task- and phase-specific alterations in triceps surae function after ACLR, reporting alterations in both the timing and magnitude of muscle activation during landing tasks, suggesting persistent neuromuscular adaptations related to anticipatory control mechanisms.15,16,29,30 Together, these findings support the idea that neuromuscular alterations after ACLR may involve both the magnitude and timing of muscle activation and may be present approximately five to six months after surgery in individuals who have resumed running.
Participants in the ACLR group were assessed at a mean of 5.6 ± 0.7 months postoperatively and had resumed running without symptoms according to predefined return-to-running criteria. The persistence of such neuromuscular alterations raises important clinical considerations. Current rehabilitation and return-to-sport criteria often emphasize strength and performance outcomes but may not fully capture underlying neuromuscular alterations.28 As a result, individuals may meet conventional performance criteria while still exhibiting altered neuromuscular strategies. In routine clinical practice, direct EMG assessment is not always feasible. Therefore, clinicians may rely on functional tests such as single-leg heel-rise capacity or hop tasks, combined with symmetry-based approaches, to monitor recovery of triceps surae function and guide rehabilitation progression.
The practical relevance of these findings should be interpreted with caution. In the present study, EMG data indicate altered neuromuscular activity of the triceps surae during single-leg functional tasks after ACLR, particularly for the soleus. However, because no kinematic, kinetic, or performance measures were collected, these results cannot be interpreted as direct evidence of altered movement mechanics, impaired functional performance, or increased ACL injury risk.31 Rather, these findings suggest that the triceps surae, and especially the soleus, may deserve greater attention during neuromuscular assessment and rehabilitation after ACLR.
Finally, it is not possible to discern whether some of the observed neuromuscular alterations may have been present prior to injury, rather than being solely a consequence of ACL injury or reconstruction. Although this interpretation should be considered with caution, it aligns with emerging evidence suggesting that pre-existing neuromuscular deficits may contribute to ACL injury risk. Saunders et al. reported that altered neuromuscular activation patterns may precede ACL injury, although prospective data remain limited.32 Further research is needed to determine whether such motor patterns represent a cause or a consequence of ACL injury and reconstruction.
LIMITATIONS
This study has several limitations regarding the conclusions that can be drawn from the results. Participants were assessed at a mean of 5.6 ± 0.7 months postoperatively. Although this postoperative window was relatively narrow, participants may have differed in rehabilitation progression, strength recovery, exposure to running or jumping activities, and sport-specific training. These factors were not controlled in the present study and may have influenced EMG outcomes. In addition, although all procedures followed a standardized surgical protocol within a single center, the involvement of three different surgeons may have introduced some variability. These sources of heterogeneity should be considered when interpreting the results and may limit the generalizability of these preliminary findings.
EMG amplitude was the primary outcome, but no concurrent measures of plantarflexor strength, jump performance, ground reaction forces, or joint kinetics were collected. Therefore, it cannot be determined whether the observed differences in EMG activity were associated with differences in muscle force production, movement strategy, or functional performance. In addition, although standardized instructions were provided, maximal effort during each jumping task could not be objectively verified because jump height and other performance outcomes were not recorded. The inclusion of participants with meniscal repair may have introduced some variability due to differences in early rehabilitation protocols, which should be considered when interpreting the results.
The relatively small sample size may have limited the statistical power to detect between-group or between-limb differences, particularly for variables with high inter-individual variability. Therefore, a power calculation should be integrated into a future protocol, along with inclusion of a larger number of participants.
Finally, the analysis of the activity was limited to the propulsion phases of the SLCMJ and the anticipation phase of the SLDJ. Jump performance outcomes were not assessed in this study, which limits the ability to relate neuromuscular findings to functional performance. A more detailed analysis of the complete motor pattern of our subjects would allow us to better understand the interactions between modification of the intensity of activation of each muscle, independently and interacting with each other, and their timing. This is particularly relevant in a context where central neurological adaptations are becoming increasingly studied and identified in the causes and consequences of ACL injuries.
CONCLUSION
The results of this study indicate that individuals after ACLR demonstrated lower triceps surae EMG activity during single-leg jumping tasks compared with healthy controls, with the most consistent differences observed for the soleus. Gastrocnemius medialis activity was also lower during the SLDJ, whereas gastrocnemius lateralis activity did not differ significantly between groups. No significant differences were observed between the operated and non-operated limbs within the ACLR group. These findings suggest that triceps surae neuromuscular activity, particularly soleus activity, may warrant further investigation during rehabilitation after ACLR.
Corresponding author
Ayrton Moiroux –Sahraoui
Orthopaedic Surgery Department, Clinic of Domont, Ramsay Healthcare, @OrthoLab, Domont, France, +33634099012
ayrton.moirouxsahraoui@gmail.com
Conflicts of interest
The authors declare no conflicts of interest.