
INTRODUCTION
Multidirectional shoulder instability (MDI) is a complex shoulder disorder characterized by symptoms including discomfort, apprehension, and chronic shoulder pain, making it challenging to diagnose, manage, and treat.1 MDI is defined as symptomatic glenohumeral subluxation or dislocation occurring in at least two directions.2
The treatment for MDI typically begins with conservative management, including a structured rehabilitation program that focuses on dynamic stabilization and scapular control. If conservative management is ineffective, surgical stabilization is generally recommended.3 The core of conservative management is exercise therapy aimed at strengthening the rotator cuff and periscapular muscles,4,5 thereby restoring shoulder joint stability. However, previous studies evaluating the effectiveness of rehabilitation for those with MDI have been limited, with some reporting favorable outcomes, while others demonstrating only minimal effects, resulting in inconsistent conclusions.6 Such discrepancies may be attributed to differences in MDI characteristics (traumatic vs. non-traumatic), subject characteristics, age, and levels of sports activity. Recently, the Watson program proposed by Watson et al. has been reported to be effective for subjects with MDI.7 However, the participants in this program had a mean age of 21.8 ± 6.5 years, and the program includes multiple exercises requiring dynamic control of the scapula and rotator cuff. Therefore, in school-aged subjects with shoulder instability, whose physical functions and motor control abilities are still developing, it may be difficult to perform these exercises accurately and consistently, indicating potential limitations in the applicability of this program. In such cases, shoulder taping may be a useful option that helps support the unstable shoulder and facilitates participation in exercise therapy. Its potential effects may involve not only external support and altered sensory input, but also psychological reassurance and other non-specific influences, including placebo-related effects, which may help reduce apprehension during shoulder movement and facilitate participation in exercise therapy.8–10
Kawabata et al.11 applied figure-of-eight taping to the shoulder in baseball pitchers with significant anterior instability and reported immediate pain reduction and improved throwing performance. In addition, Aruga et al.12 described a case of traumatic recurrent massive rotator cuff tear in which figure-of-eight taping to the shoulder, combined with ultrasound-guided exercise therapy, was associated with improvement in pain and shoulder function. In these previously reported adult cases, the underlying pathology primarily involved either anterior instability associated with repetitive throwing loads or traumatic structural damage. In contrast, the present case involved a school-aged female karate athlete with MDI, characterized by predominant anterior and inferior instability associated with intrinsic laxity and no history of trauma. This difference in underlying pathophysiology represents a key unique aspect of the present case and highlights its clinical significance.
This case report details a five-month rehabilitation program for a school-aged female karate athlete diagnosed with MDI, in which figure-of-eight taping was incorporated into rehabilitation to support exercise.
Case Description
Participant History
The subject was a 12-year-old female karate athlete with right-hand dominance. She had no apparent precipitating factors such as trauma but began experiencing a sense of discomfort in her right shoulder around 2022. Pain developed in addition to the discomfort that started in 2024, and she was diagnosed with MDI upon presentation in April 2025. Her sports history included karate, which she began in the first grade of elementary school and had continued to practice. There was no history of shoulder intervention, and the rehabilitation intervention described in this study was implemented for the first time. Written informed consent for publication of this case report and any accompanying images was obtained from the subject and her parent.
Initial examination
The subject’s chief complaint was a “clicking” sensation in the right shoulder, which made carrying a backpack difficult. The pain was localized to the posterior aspect of the right shoulder and was present at rest and during movement. Shoulder flexion was limited, with the subject reporting a sensation of subluxation before reaching 90° of flexion. On orthopedic examination, the sulcus sign was positive bilaterally and was more pronounced on the right side. The load and shift test was also positive bilaterally, with greater laxity on the right side and notable anterior instability. Instability of the right shoulder was observed in the dependent external rotation position, and the relocation test result was positive. Overall, inferior and anterior instabilities were predominant. Assessment of scapular movement revealed that the scapula was positioned in a depression, anterior tilt, and downward rotation at rest, with diminished upward rotation during shoulder flexion. The scapular assistance test13 result was negative, and scapular manipulation did not relieve the symptoms. Joint laxity was assessed using the Beighton Hypermobility Score14 and was negative (Table 1).
Intervention
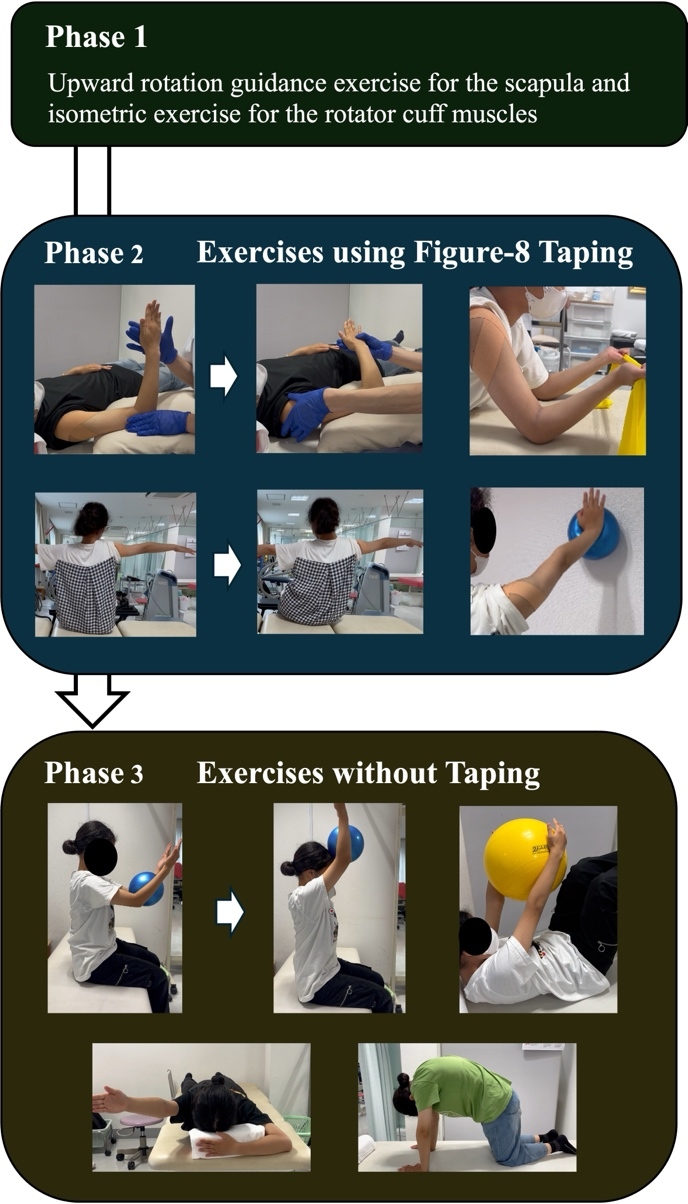
The intervention was conducted over a five-month period from April to September 2025, with a total of 22 sessions. The timeline of the rehabilitation process is shown in Figure 1. During the initial phase (Phase 1) of the intervention, based on a previous study,4 rehabilitation focused on exercises aimed at scapular upward rotation combined with isometric rotator cuff exercises. Scapular upward rotation exercises were initiated with active-assisted movement in the side-lying position and progressed to standing scapular setting into upward rotation with a shrug at 20° to 30° of shoulder abduction. The rotator cuff exercises consisted of isometric internal and external rotation exercises performed with the shoulder in the scapular plane. These exercises were performed for 2–3 sets of 10–20 repetitions, with each isometric contraction held for 5 seconds.
After one month, the pain at rest and during movement decreased from 5 to 0 on the numerical rating scale (NRS); however, the sensation of subluxation around 95° of shoulder flexion persisted, making it difficult to perform dynamic exercises effectively due to the feeling of instability. As the relocation test in the resting arm position was positive at the initial evaluation, local glenohumeral instability was considered to hinder the progression of rehabilitation.
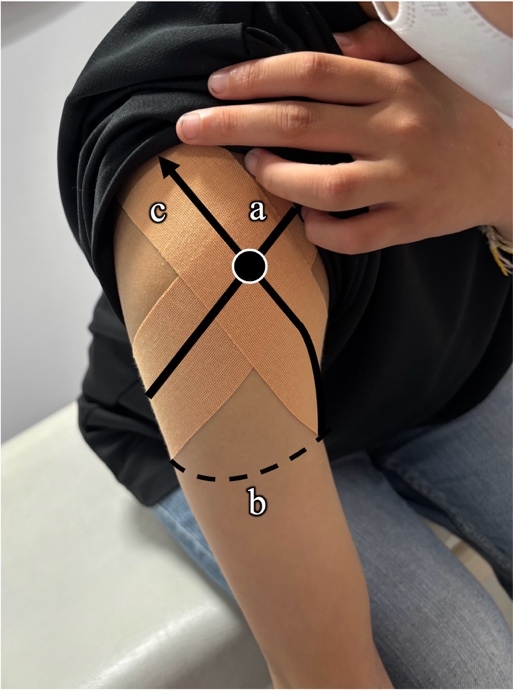
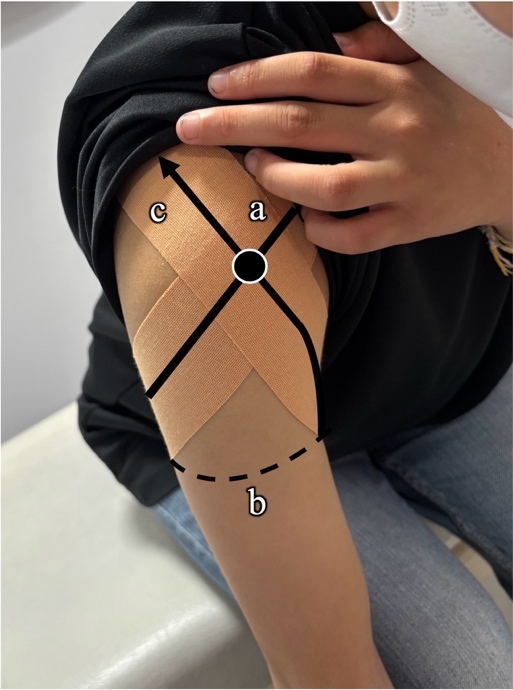
In Phase 2, exercises were performed while locally stabilizing the glenohumeral joint using a figure-of-eight tape. Based on the method reported by Kawabata et al.,11 the subject was positioned with the trunk leaning forward and arm hanging naturally from the side. One strip of kinesiology tape (25 mm wide; Daiwakan Kinesiology Tape, Daiwakan Co., Ltd., Osaka, Japan) was applied according to the following procedure (Figure 2).
-
Tape was applied from the coracoid process across the anterior humeral head, extending laterally to posteriorly around the upper arm (tensioned at 110–120%).
-
The tape was passed horizontally across the posterior aspect of the upper arm.
-
From the axilla, the tape was applied upward along the anterior humeral head toward the anterior acromion, again at 110–120% tension.
-
The tape was anchored to the posterior aspect of the scapular spine.
After the trunk was returned to the upright position, tape tension was directed anterosuperiorly toward the humeral head, thereby enhancing anterior glenohumeral joint stability.
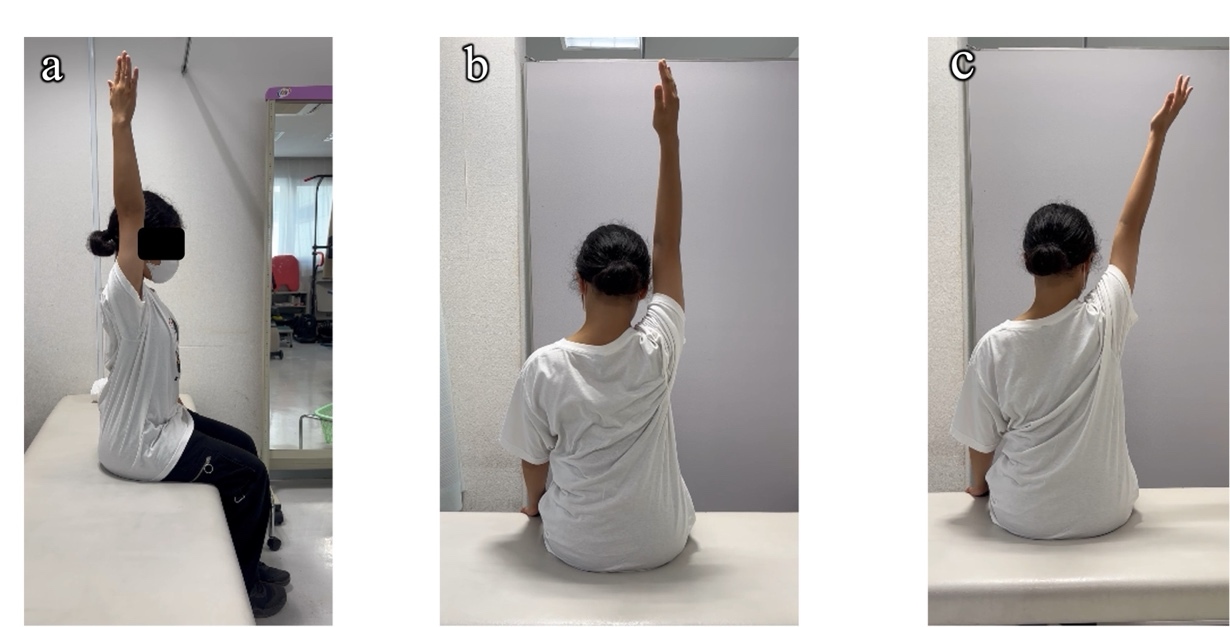
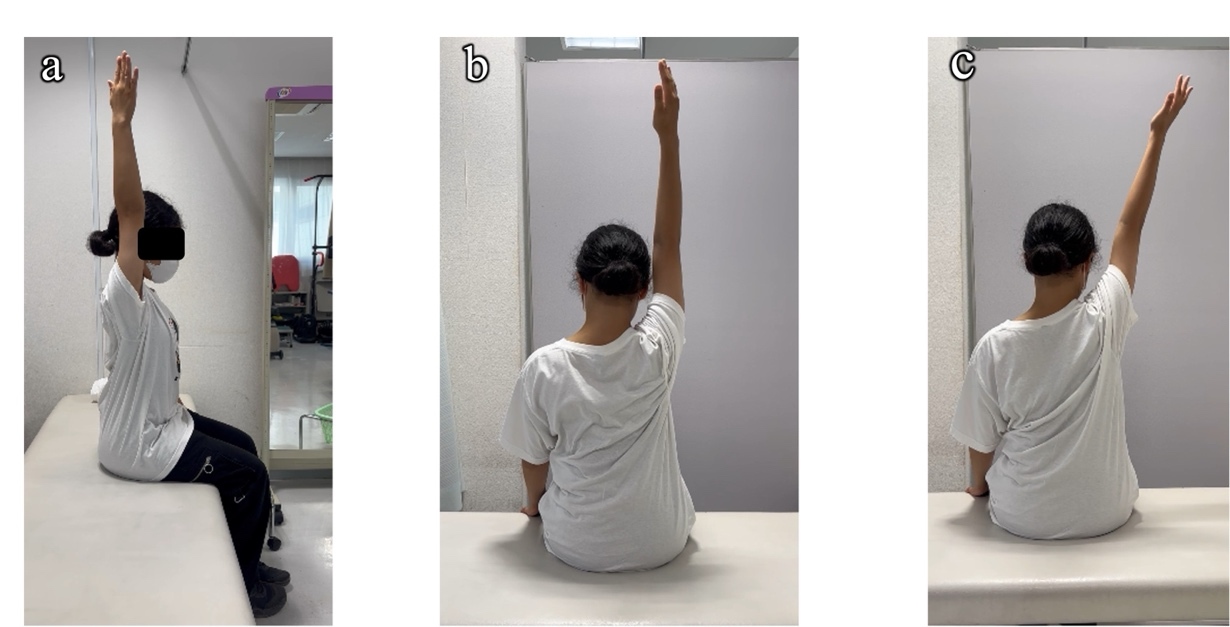
Following the application of figure-of-eight taping, the subject’s active shoulder flexion range of motion immediately increased from 95° to 140°, and shoulder instability decreased from an NRS of 10 to 3 (Figure 3, Video. 1). Consequently, the rehabilitation program was modified to include rotator cuff and scapular muscle exercises performed while wearing the tape. Rotator cuff exercises were initiated with internal and external rotation through the full range of motion against manual resistance in the scapular plane in the supine position and then progressed to active shoulder abduction exercises in the side-lying position and internal and external rotation exercises using an elastic band with the shoulder in an elevated position. Scapular muscle exercises were also progressed to closed kinetic chain exercises performed with the shoulder in an elevated position. These sessions were conducted approximately once or twice per week for approximately two months, and each exercise was performed for 2–3 sets of 10-20 repetitions according to symptom tolerance. The subject and her parent were instructed on how to apply the tape at home, allowing it to be used during daily activities, self-training, and karate practice.
After two months of rehabilitation with taping during Phase 2, the program progressed to Phase 3. At this stage, the subject was able to actively perform shoulder flexion to 120° without taping. During this phase, the rehabilitation program without taping was further progressed to include scapular setting in the elevated position, scapular muscle exercises integrated with core exercises, and closed kinetic chain exercises, each performed for 2–3 sets of 10–20 repetitions according to symptom tolerance. These interventions contributed to further improvement in shoulder stability during active shoulder flexion.

OUTCOME
After five months of rehabilitation, active shoulder flexion improved from 85° to 180° and abduction increased from 70° to 170° (Figure 4, Video 2). At the end of this period, the subject achieved a total Rowe score15 of 80 of 100, corresponding to a “good” outcome, and the SANE-Instability score16 reached 90% (Table 2). Regarding activities of daily living, the subject was able to carry a backpack, which had previously been impossible, and successfully resumed physical education classes. During karate practice, shoulder movements in the elevated positions that were previously limited could now be performed satisfactorily. Finally, the subject achieved second place in a regional karate tournament. Quick-DASH scores showed temporary worsening at three months; however, at five months, compared to the scores at one month, the disability/symptom component decreased by 6.8 points, and the sports component decreased by 25 points (Table 2).
DISCUSSION
This case report describes the clinical course of a school-age female karate athlete with MDI who underwent a staged rehabilitation program combined with figure-of-eight taping. Over the 5-month rehabilitation period, the subject showed improvements in pain and shoulder function. These findings suggest that figure-of-eight taping may have helped facilitate exercise therapy in this pediatric case of MDI.
In a previous case report,17 a 14-year-old female with Ehlers–Danlos syndrome and MDI initially underwent conventional rehabilitation for three months, which did not improve shoulder instability. Subsequently, she participated in the Watson program for three months, which resulted in clinical improvement and a favorable course. At the end of the total six-month intervention, the Rowe score had improved to 70 points, active shoulder flexion reached 155°/150° (right/left), and active abduction reached 110°/115° (right/left).17 In the present case, similarly, Phase 1 was based on the Watson program, focusing primarily on exercises that promoted scapular upward rotation.4 However, this intervention required the subject to perform exercises despite a sensation of glenohumeral instability, making it difficult for a school-aged subject to maintain sufficient stability during the movements.
Therefore, a figure-of-eight taping technique was applied, and active shoulder flexion immediately increased from 95° to 140°. Based on this response, the treatment plan was modified, and Phase 2 rehabilitation was performed with the subject performing exercises while wearing the tape. Previous reports describing figure-of-eight taping for shoulder disorders involved two adult cases. Kawabata et al.11 reported immediate pain reduction and improved throwing performance in baseball pitchers with marked anterior instability after application of figure-of-eight taping. In addition, Aruga et al.12 reported improvement in pain and shoulder function in a subject with traumatic recurrent massive rotator cuff tear. In contrast, the present case involved a school-aged female karate athlete with MDI and therefore differed from the previously reported adult cases in terms of age, pathology, and sports background. Although direct comparison is limited, this case may add to the existing literature by illustrating the clinical application of rehabilitation combined with figure-of-eight taping in a pediatric subject with MDI. As a possible explanation for the effects of figure-of-eight taping, Aruga et al.12 reported, based on dynamic ultrasonographic findings, that during shoulder flexion, the humeral head translated smoothly beneath the acromion without impingement, thereby allowing greater shoulder flexion. These findings suggest that figure-of-eight taping may contribute to improved centering of the glenohumeral joint. However, because no imaging assessment of humeral head motion was performed in the present case, the observed effects cannot be explained solely by biomechanical stabilization. In addition, the effects of taping may involve psychological reassurance and non-specific influences, including placebo-related effects.8–10 Through these multifactorial effects, the subject may have been able to perform exercises with less apprehension while wearing the tape during Phase 2, which may have supported progression of the rehabilitation program. Importantly, figure-of-eight taping should be viewed as a temporary adjunct rather than a long-term intervention. In this case, taping was used during the early phase to provide support and facilitate exercise therapy while the subject experienced a sensation of shoulder instability. The taping intervention was discontinued after two months, allowing the subject to progress to the final phase of rehabilitation without external support.
In Phase 3, active shoulder flexion remained improved, even without taping, and the subject was able to perform scapular upward rotation exercises in the elevated position as well as rotator cuff exercises without taping. Over the five-month phased rehabilitation program, the subject demonstrated improvements in shoulder instability scores and range of motion and was able to perform karate movements effectively. In the school-aged subject with MDI, when exercise therapy such as the Watson program is difficult owing to glenohumeral joint instability, the use of taping in the early phase may serve as a useful adjunct to support exercise therapy aimed at improving shoulder function.
LIMITATIONS
This case report had several limitations. First, the intervention period was relatively short (five months), and the long-term outcomes remain unclear. Considering the high recurrence rate of MDI associated with conservative therapy,18 long-term follow-up is necessary. Second, as a single case report without a control condition, it cannot establish a cause-and-effect relationship between figure-of-eight taping and the observed outcomes. Third, taping was used as part of a multimodal rehabilitation program, and its specific effects could not be separated from those of exercise therapy or other aspects of care. Fourth, the observed improvements may have been influenced by non-specific factors, including psychological effects and placebo-related effects. A strength of this report is that it provides a detailed description of the rehabilitation course and serial outcomes in a school-aged athlete with MDI. Further prospective and comparative studies involving multiple cases are needed to evaluate the effectiveness of figure-of-eight taping as an adjunct to rehabilitation for shoulder disorders.
CONCLUSIONS
In the school-aged female karate athlete with MDI, figure-of-eight taping may have provided immediate support in the early phase and served as a useful adjunct to facilitate exercise therapy. However, because this report describes a single case with a relatively short intervention period, further prospective studies involving multiple subjects are needed to evaluate the effectiveness and long-term outcomes of this specific taping intervention.
Conflict of Interest
The authors declare no conflicts of interest.
Acknowledgments
We would like to thank the subject for their cooperation and consent in allowing us to share this case report. We also thank Editage (www.editage.jp) for English language editing.