
Introduction
Ankle sprains are among the most common injuries in sports. A systematic review estimated that the incidence of ankle sprains is approximately 0.72 to 13.6 per 1000 athletic exposure hours.1 Another epidemiological study reported that the rate of ankle sprains between the ages of 15 and 19 years is 7.2 per 1000 exposure hours.2 Between 80% and 90% of all ankle sprains are lateral ankle sprains (LASs).3–5 In addition, 80% of individuals who experience LASs experience recurrent injury, and 75% of individuals who experience recurrent ankle sprains develop chronic ankle instability (CAI).3–5 CAI can be differentiated into functional and mechanical ankle instability. LASs cause impaired movement and neuromuscular control deficits in patients with ankle proprioception and exemplify functional ankle instability. By contrast, tissue structure injuries, such as ankle ligament laxity, exemplify mechanical ankle instability. Both types of ankle instability often occur in individuals with CAI.6
Athletes with CAI typically protect their ankles with sports tape (ST), which can increase the stability of the ankle joint but limits range of motion and performance.7 A study reported that beyond increasing the stability of the ankle joint, ST was not associated with superior performance on the Star Excursion Balance Test.8 By contrast, elastic tape can stretch and enable athletes to move freely.9 Two types of elastic taping methods are commonly used in sports settings: kinesiology taping and dynamic taping (DT). Kinesiology taping has been extensively studied since the mid-2010s. Several authors have reported that Kinesiology taping stimulates skin receptors,10 improves proprioception,11 increases ankle mobility,12,13 and enhances posture control.14 However, kinesiology taping does not provide ankle support and stabilization.15 Moreover, although kinesiology taping can enhance postural control in simple balance tasks, a study suggested that it has a nonsignificant effect on postural control and stabilization in difficult balance tasks.16 This indicates that kinesiology taping can improve proprioception of the ankle joint and slightly influence postural control but does not clearly support or protect the ankle joint.
DT is an elastic taping method developed by Australian physiotherapist Ryan Kendrick.17–19 DT has distinct applications from those of kinesiology taping and is based on biomechanical principles. Notably, DT can be stretched in multiple directions, in contrast to kinesiology tape, which stretches only in one direction, and has high elasticity similar to a rubber band. Kendrick demonstrated that DT can manage load by modifying movement patterns and functions. Its strong elasticity also enables the body to absorb external loads and assists in force generation to minimize stress.17–20
Pawik et al. studied changes in postural stability on a stable surface in patients with Grade I and II inversion ankle sprains whose ankles had been taped using DT.17 The patients were enrolled in the acute or subacute phase of ankle sprain and were assessed for balance in a standing position with eyes open or closed and in the presence of visual feedback. The results revealed that the patients did not exhibit significant improvements in certain balance parameters in tests on a stable surface with eyes open or closed eyes.17 However, that study was limited to patients with acute or subacute ankle sprain and did not examine DT in patients with CAI, and the balance assessment was a static evaluation on a stable surface rather than a dynamic balance (DB) test. Lim and Park compared the effect of Kinesio tape and DT on static and DB in individuals with asymptomatic flexible flatfoot.18 Twenty-two participants were recruited to complete the Y-Balance test (YBT) and a 30-s standing test barefoot while the center of pressure (COP) was measured. The results revealed that the scores on the YBT significantly increased after the application of DT relative to no taping and of kinesiology tape relative to no taping, whereas the difference in COP during static standing between the three conditions was nonsignificant. However, these results may not be generalizable to patients with CAI. Addressing this gap, Kodesh et al. examined the effects of DT on balance control in individuals with CAI.21 In their experiment, the single-limb stance test with eyes open and closed was conducted before, 10 min and 24 h after DT was applied over the gastrocnemius muscle. The results revealed that DT enhanced balance control. However, Kodesh et al. did not assess DB, which indicates stability and balance during sports activities. Accordingly, whether DT improves DB in individuals with CAI remains unclear. Therefore, the purpose of this study was to compare the immediate effects of DT and ST on dynamic balance and proprioception in recreational athletes with CAI.
Methods
Study Design
This study adopted a pretest-posttest comparative design. The sample size estimation was conducted using GPower 3.0 software (Heinrich Heine University, Germany). The authors calculated the sample size using a repeated-measures analysis of variance (ANOVA) with between-group factors and the following parameters: two-tailed test, effect size f = 0.5, power = 0.8, and α = .05. Accounting for a 10% withdrawal rate, this study determined that a sample size of 28 participants was required (14 per group).
Participants
This study screened 28 recreational athletes with chronic ankle instability by using the Cumberland Ankle Instability Tool (CAIT) and randomly divided them into two groups: an ST group (n = 14) and DT group (n = 14). The inclusion criteria were (1) having had at least one ankle sprain and having a CAIT score of <25 points,22 (2) not having other musculoskeletal injuries or surgery on the lower extremities in the three months before the experiment, and (3) engaging in physical activities for at least two hours twice a week. The exclusion criteria were (1) having experienced a fracture of the lower limbs or undergone surgical treatment, or (2) having neurological deficits or vestibular system deficits that rendered performing the experimental procedures impossible. All participants were familiarized with the experimental procedure and associated risks and provided written informed consent before the experiment commenced. The protocol of this study was approved by the Institutional Review Board of Fu Jen Catholic University in Taiwan (IRB No.: C109054).
Taping Application
ST. In this study, Mueller MTape 1.5 in × 13.7 m (Mueller Sports Medicine, Inc., United States) was used to tape the participants’ ankle joints. Before taping, a skin wrap was used to cover the foot and ankle joints. After the upper part of the ankle joint and the forefoot were anchored, a predetermined taping technique (horseshoe, stirrup, figure-eight, or lock-heel) was applied (Figure 1).23 These taping techniques limited ankle range of motion and provided increased stability to the injured ankle.
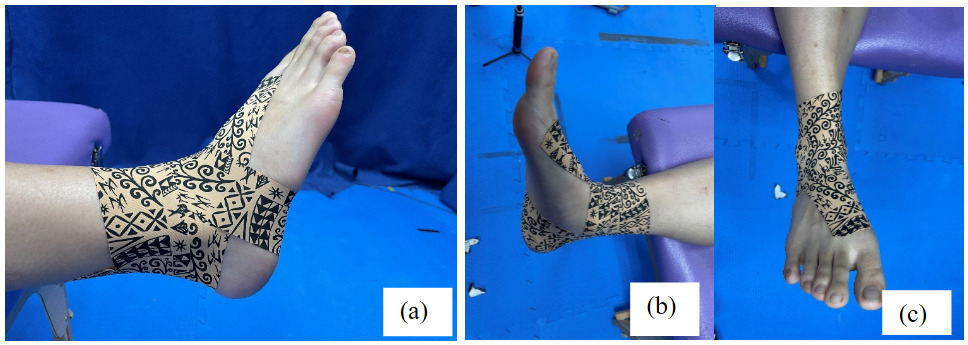
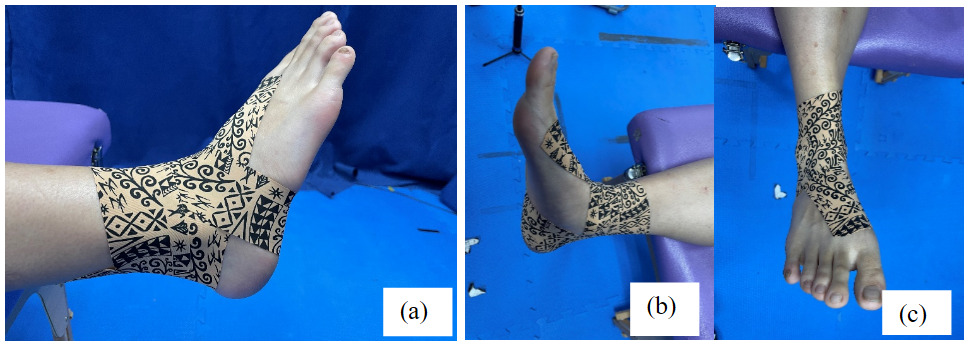
DT. The ankle DT technique used in this study followed the method indicated in the official DT teaching video (Supplemental Video). All taping personnel had obtained DT Levels 1 and 2 International certifications. All participants were seated during taping. First, the participants were asked to maintain the foot dorsiflexed and everted. Tape was applied from the dorsal side of the first toe across the foot and ankle joint at an oblique 30° to 45° angle to the lateral malleolus, after which the tape was wrapped across the heel. The participants were subsequently asked to maintain the sole of the foot in plantar flexion in the valgus position as tape was applied from the lateral malleolus to the heel and wrapped around the bottom of the calcaneus. The participants next pointed the sole of the foot in the direction of the heel in a neutral posture as the tape was wrapped from the outside of the foot to the talus, and the final anchor point was placed on the medial malleolus close to the calf side (Figure 2).
_underwrap__(b)_anchor__(c)_stirrup__(d)_horseshoe.png)
Outcome Measurements
Baseline evaluations involved demographic assessments, medical histories, and a physical examination. To mitigate fatigue after DB had been tested, this study assessed the proprioceptive joint position sense error before the single-leg multiple hop stabilization test. The measurement sequence after the taping was identical. The outcome variables were assessed before tape application and 15 min after tape application.
Proprioceptive error of joint position sense measurement24
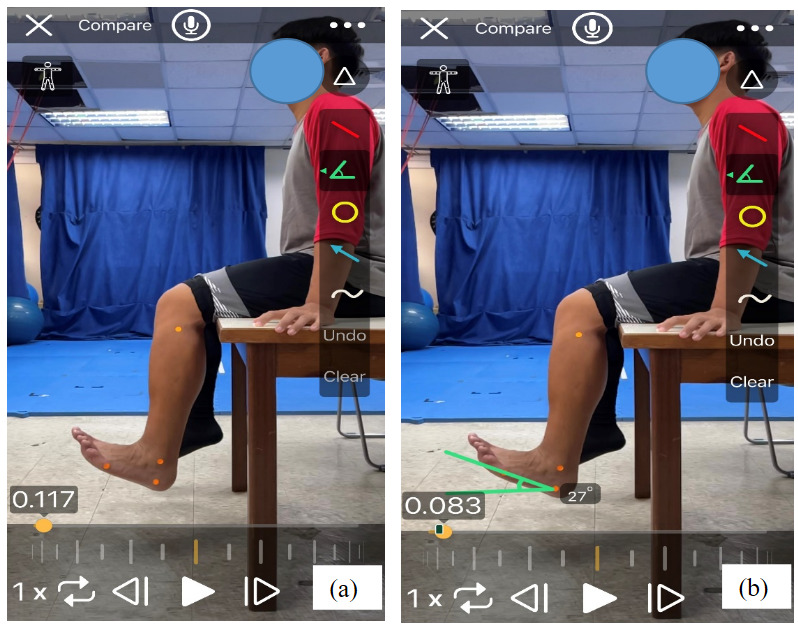
At the beginning of the measurement of proprioceptive joint position sense error, the participants sat with the knee joint at 90° flexion and the ankle hanging naturally (Figure 3). Before assessing the joint position sense error, the researcher used a mobile phone with a G-pro Goniometer app to establish the range of motion of the ankle joint at a distance of 1.5 m between the mobile phone and the participants. During the measurement, four color markers were placed on the lateral side of the leg at the fibular head, lateral malleolus, head of the fifth metatarsal bone, and lateral side of the foot in the line connecting the fibular head to the lateral malleolus of the ankle. The researcher asked the participants to dorsiflex or plantarflex the foot with eyes closed, after which the angle was calculated using a mobile phone app. The participants practiced moving the ankle joint to the specified test angle and were asked to remember this position. The specified test angle was set at 50% of full ankle range of motion (ROM), which was calculated as the sum of plantarflexion plus dorsiflexion active ROM established before the joint position sense error measurement. The participants performed three practice trials. After the practice trials had been completed, joint position sense error was assessed for three trials, and the average of those three trials was calculated as the final result value. During the measurements, the participants were blindfolded and wore headphones that played white noise to ensure that no visual or vestibular cues biased the measurements. Before the formal measurements, test-retest reliability was established; the intraclass correlation coefficient was 0.940.
_starting_position_and_(b)_ending_position.png)
Dynamic Balance test (single-leg multiple hop stabilization test)25,26
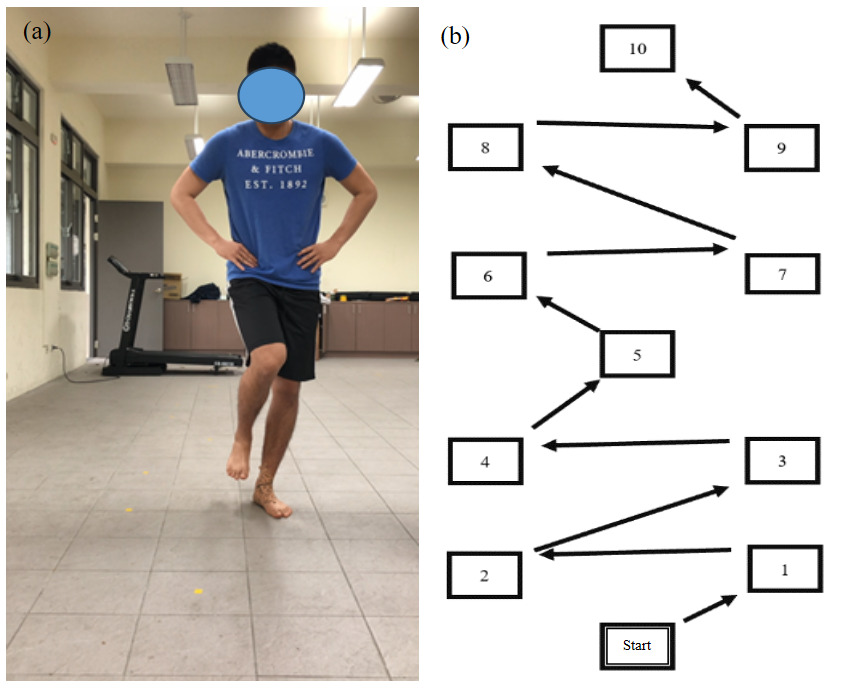
The single-leg multiple hop stabilization test was used to assess DB. The test used the standard functional performance measurement of Reiman et al.26 Before testing, the participants performed a standardized warm-up consisting of 3 to 5 single-leg hopping exercises to familiarize themselves with the movement task without practicing on the test markers. After the warm-up, the participants performed consecutive single-leg hops across a predefined sequence of markers and were required to stabilize their position for 5 s after each landing. Performance was evaluated based on two types of errors: (1) landing errors (eg, incorrect foot placement or loss of alignment) and (2) balance errors (eg, loss of postural control or additional foot contact). The total DB score was calculated using the following formula:
DB = (number of landing errors × 10) + (number of balance errors × 3)
A lower score indicates superior DB.25,26 Figure 4 illustrates the test procedure. Before the formal measurements, the test-retest reliability was established; the intraclass correlation coefficient was 0.868.
_test_.png)
Statistical Analyses
The data were analyzed with IBM SPSS Statistics, version 25.0 (SPSS Inc., Chicago, IL, USA). The normality of the distribution of all variables was verified using the Shapiro-Wilk test. The independent variables were the two taping groups (DT and ST group). The dependent variables were ankle joint position sense error and DB scores. The pre-test scores were subtracted from the post-test scores, and the result was divided by the pre-test scores and multiplied by 100 to obtain the change between the pre-test and the post-test. Group demographics were analyzed through an independent-samples t-test. A repeated-measures 2-way ANOVA was used to assess interaction effects with the taping method. Significance was set at α = .05.
Results
Table 1 presents the demographic characteristics of the participants. The CAIT score of all the participants was <25. The demographic characteristics of the groups did not significantly differ.
A significant interaction was observed between pretest and posttest values and group in the DB scores (F = 20.42, p < 0.05, η2 = 0.440), irrespective of landing error (F = 111.61, p < 0.05, η2 = 0.309) and balance error (F = 8.845, p < 0.05, η2 = 0.254). However, no significant differences were uncovered with respect to joint position sense error (F = 0.847, p = 0.366, η2 = 0.032; Table 2).
In the analysis of the pre-test and post-test values for the two groups, both the joint position sense error and DB scores significantly decreased, which indicated improvement in both variables. The joint position sense error scores were significantly reduced after the intervention in both groups, whereas the DB score significantly decreased only in the DT group (Table 3).
Discussion
This study compared the effects of ST and DT on ankle proprioception and DB. The results indicate that joint position sense errors decreased in both taping groups, which did not differ significantly in the pretest-posttest and intergroup comparisons. A significant interaction was observed between ST and DT and between the pretest and posttest balance scores. These findings suggest that DT may be more effective than ST in improving DB.
Taping on the skin can enhance proprioception, as the present study’s findings demonstrated. After an ankle sprain, proprioception is impaired. Individuals with CAI exhibit greater ankle JPSEs than those without CAI do.27 In a study on volleyball players with CAI, in addition to the immediate effect of ankle sport taping on proprioception, continual taping for two weeks and for two months also improved proprioception.28 Furthermore, Parka et al. applied DT on the shoulder and examined proprioception; after DT was applied, shoulder joint proprioception was enhanced.29 The present study compared the immediate effect of ST and DT on the ankle joint, and the results indicated that both tape groups exhibited significantly reduced joint position sense errors compared with the pre-taping condition. The underlying mechanism may involve enhanced stimulation of cutaneous receptors, particularly mechanoreceptors, that facilitate proprioceptive feedback. The skin transmits proprioceptive signals to the spinal cord and increases the activation of motor neurons, which enhances the positional sense of the ankle and feet.28,30 Because studies on ankle position sense with DT have yet to be conducted, this study referenced studies that have been conducted using kinesiology tape. Kinesiology tape has been demonstrated to enhance joint position sense of the ankle joint and affect the DB of individuals with CAI.31 In a study on the shoulders of healthy adults treated with kinesiology tape, the results revealed that kinesiology tape benefitted proprioception and neuromuscular control.32 Nevertheless, some studies have reported that kinesiology tape does not significantly increase proprioception,33–35 This difference may be attributable to differences in the health of the participants in these studies. Although ST and DT differ, both methods stimulate skin receptors, enhancing proprioception by reducing proprioceptive errors.
In the present study, both ST and DT reduced joint position sense errors and enhanced proprioception. However, only DT improved the dynamic balance. That indicated the proprioceptive improvement achieved through ST may have been insufficient to induce effective changes in postural control that influence DB. By contrast, DT enhanced both proprioception and DB, reflected in landing error and balance error scores. This result suggests that ST can enhance proprioceptive input by increasing sensory feedback on body position and movement; it may not translate into improvements in DB or postural control. DB involves maintaining stability during movement, whereas postural control involves maintaining stability while stationary; both are influenced by factors other than proprioceptive input.25 As elastic tape may is more adaptable than ST when applied to human skin it may stretch the skin and underlying fascial tissue with body movements, thereby increasing proprioceptive input. A previous study also showed that the elastic tape improves a simple balance task (e.g., barefoot on a hard floor with eyes open) and may slightly influence postural control.36 Therefore, although ST may enhance proprioceptive awareness, its influence on overall balance and postural stability warrants further evaluation in additional interventions.
However, in athletes with CAI, both neuromuscular control and mechanical structures may be compromised, potentially leading to positional faults.37,38 Authors who reported that on lateral ankle radiographs, found that the position of the talus was significantly more anterior in the ankle with CAI than in the unaffected ankle.37 Therefore, if the positional fault of the ankle with CAI can be corrected or the ankle’s structure can be addressed, ankle stability could be enhanced.19,20 Consequently, it is possible that DT applied to the ankle joint may have produced a stabilizing effect at the joint. DT also exhibits strong recoil and elastic resistance, which assist the body in absorbing load and help generate force to reduce stress. This stress reduction may modify faulty joint or movement patterns and enhance biomechanical efficiency.19,20 For example, Lim and Park applied DT in patients with asymptomatic flat foot and assessed performance on the YBT.18 Their results revealed that YBT scores significantly increased after the application of DT compared with no tape. Lim and Park posited that DT holds the foot more firmly than ST while not limiting the ROM during the YBT. This result is consistent with that of the present study. The unique elastic materials used in DT provide resistance to structural faults through their inherent elasticity and enhance proprioceptive feedback. This dual mechanism may be responsible for the observed improvements in DB in the athletes with CAI in this study. Studies have also explored the effects of DT on postural control and neuromuscular function in individuals with ankle sprain or CAI. It has been demonstrated that DT may enhance balance and reduce postural sway in individuals with various musculoskeletal conditions (eg. ankle sprain or CAI).17,21 In addition, evidence from studies on elastic taping suggests that improvements in proprioception and sensorimotor control may contribute to enhanced functional performance during dynamic tasks. These findings suggest the potential of DT as a biomechanical and neuromuscular intervention, although further high-quality studies are required to verify its effectiveness. Future research should investigate the application of DT with subsequent assessment during more complex movements and sport-specific tasks such as cutting maneuvers or shuttle runs to evaluate its ability to enhance functional performance and mitigate injury.
This study has several limitations. First, although the sample size was determined using an a priori power analysis, the paucity of participants may have limited the generalizability of the findings. In addition, the limited sample size may have increased the risk of Type II error, particularly for variables that did not significantly differ between groups. Second, the results should be interpreted with caution and may not apply to populations other than recreational athletes with CAI. Future studies with larger and more diverse samples are required to enhance external validity. Third, this study only assessed immediate effects, which may not reflect responses during prolonged physical activity or training. Consequently, the persistence of improvements in proprioception and DB remains unclear. Furthermore, the relationship between taping interventions and injury was not evaluated in this study. Future longitudinal and sport-specific studies are required to examine the effects of DT during extended periods of activity, determine whether its benefits are sustained over time, and investigate its role in reducing injury incidence in athletes with CAI.
Conclusions
This study investigated the immediate effects of DT on athletes with CAI relative to the effects of ST. The results revealed that both DT and ST enhance proprioception, but only DT improved the dynamic balance in individuals with CAI.
Corresponding author:
Hsiao-Yun Chang
E-mail: yun1130@ntsu.edu.tw
Address: Department of Athletic Training and Health, National Taiwan Sport University, No. 250, Wenhua 1st Rd., Guishan Dist., Taoyuan City 333325, Taiwan
Tel: 886-3-3283201#2503
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
Acknowledgments
The authors would like to thank all participants in this study. This manuscript was edited by Wallace Academic Editing.
Funding
This study did not receive any funding.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because of privacy or ethical restrictions.