Introduction
Diagnostic musculoskeletal ultrasound (MSKUS) has become an essential tool for evaluating musculoskeletal structures. Rotator cuff injuries are one of the more common injuries that occur in the shoulder. Four muscles and tendons make up the rotator cuff. These include the supraspinatus, infraspinatus, subscapularis, and the teres minor. While much attention has historically focused on the supraspinatus and infraspinatus tendons, the teres minor remains comparatively underexamined. This paper aims to provide a comprehensive review of diagnostic MSKUS of the teres minor, including relevant anatomy, scanning technique, normal and abnormal imaging characteristics, and common pathological findings.
Anatomy of the Teres Minor Muscle of the Rotator Cuff Complex
The teres minor is the smallest of the rotator cuff muscles. It originates from the middle third of the lateral border of the scapula, just below the insertion of the teres major. It inserts onto the inferior facet of the greater tubercle of the humerus. The teres minor is innervated by the axillary nerve, and its muscular action is that of external rotation, and it can be a weak abductor of the shoulder. It is part of a larger force couple between the rotator cuff group and the deltoid, which stabilizes the humeral head during humeral elevation. An intact teres minor makes a huge contribution to overall shoulder function in a patient with a large or massive rotator cuff tear, providing at least a minimal degree of external rotation force1,2 that allows patients to perform important activities of daily living that would be absent without a teres minor.
The Role of MSKUS in Tendon and Muscle Evaluation of the Teres Minor
Advantages
-
Real-Time Imaging: MSKUS allows dynamic evaluation of the teres minor muscle and tendon while the shoulder can be moved through internal and external rotation, with an available range of motion.
-
High-Resolution Visualization: MSKUS provides detailed images of the teres minor tendon and its proximal enthesis at the posterior portion of the greater tuberosity.
-
Accessibility and Cost-Effectiveness: MSKUS is portable, widely available, and less expensive than magnetic resonance imaging (MRI).
Limitations
-
Operator Dependency: MSKUS requires skill and experience for accurate interpretation of findings. The ability to sonograph tendons and their respective muscles is to a large extent influenced by the operator and the availability and technical considerations of state-of-the-art equipment.
-
Depth Limitations: Visualization is usually not a problem as the tendon and muscle of the teres minor are superficial.
-
Artifacts and Shadows: Bone shadowing from the humeral head may create image artifacts, requiring adjustments in probe positioning and frequency. Calcifications are uncommon in the teres minor and typically occur in the supraspinatus tendon; however, several case studies have shown that this can occur.3–5
Sonographic Technique for Evaluating the Teres Minor
Equipment Setup
-
Probe Type: Because of the superficial depth of the teres minor muscle and tendon, a standard high-frequency, linear array probe is utilized.
-
Patient Position: The patient is seated with the shoulder in neutral or holding the opposite arm to put a slight stretch on the teres minor muscle and tendon for better visualization.
-
Dynamic Assessment: A passive or active movement of shoulder internal or external rotation can create lengthening or shortening of the muscle and tendon to better evaluate its excursion properties.
Examination Protocol
Normal Sonographic Appearance
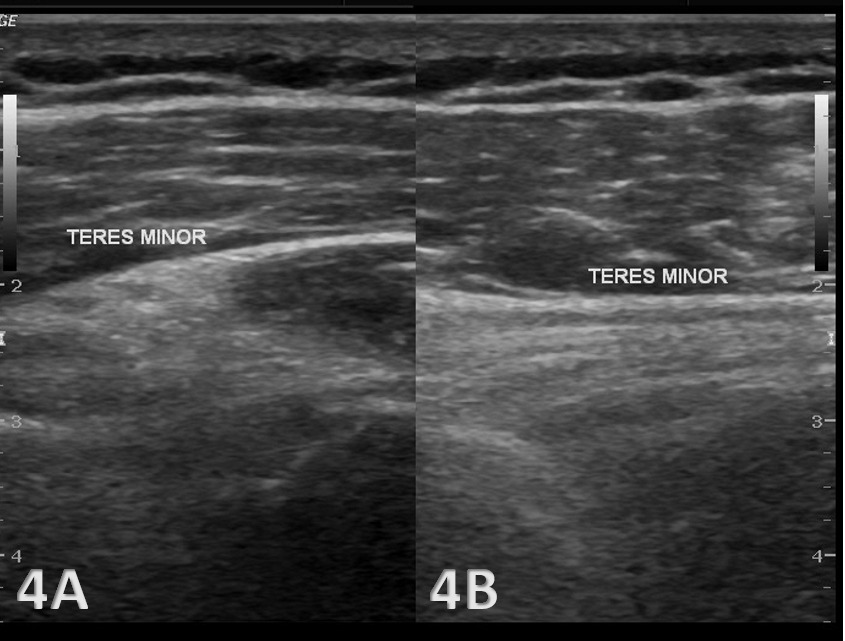
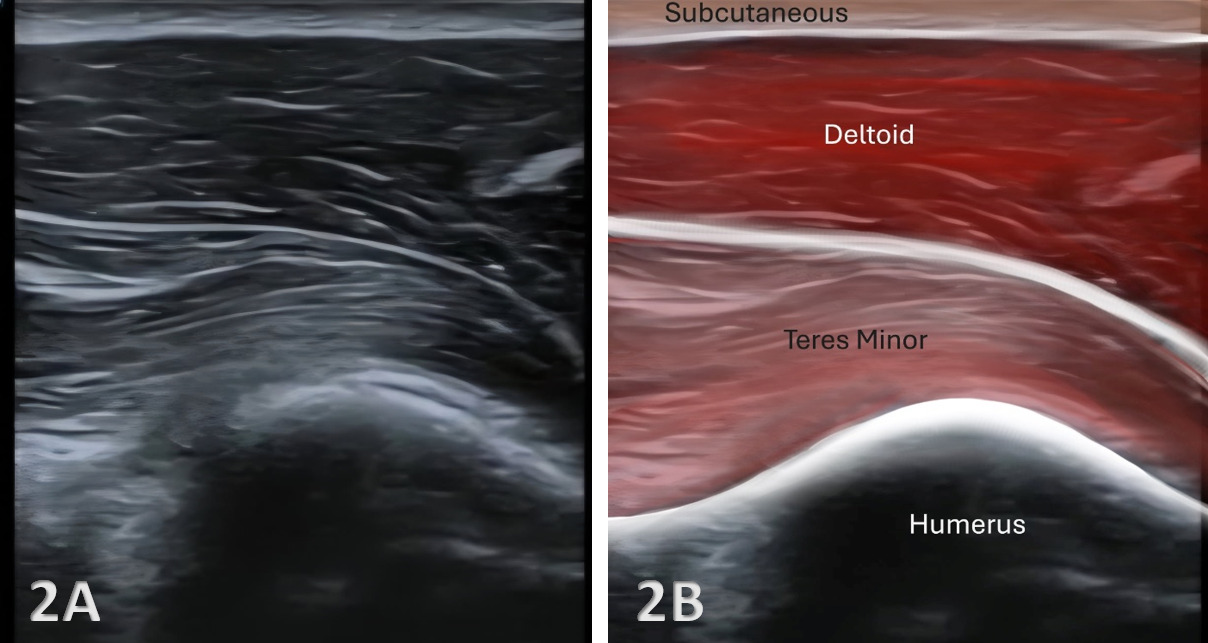
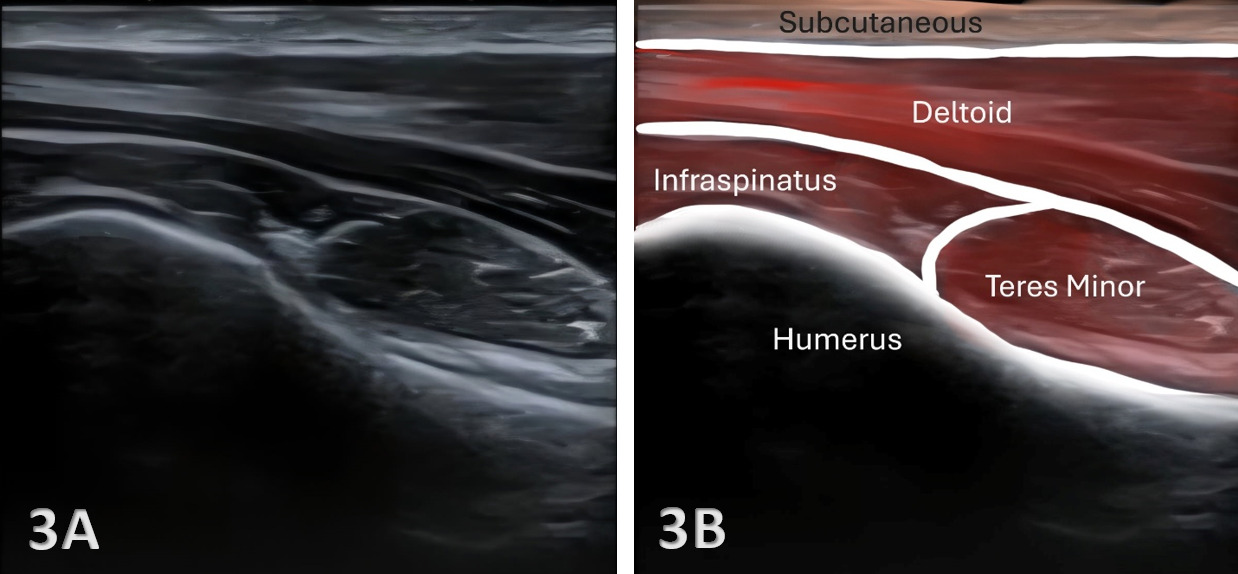
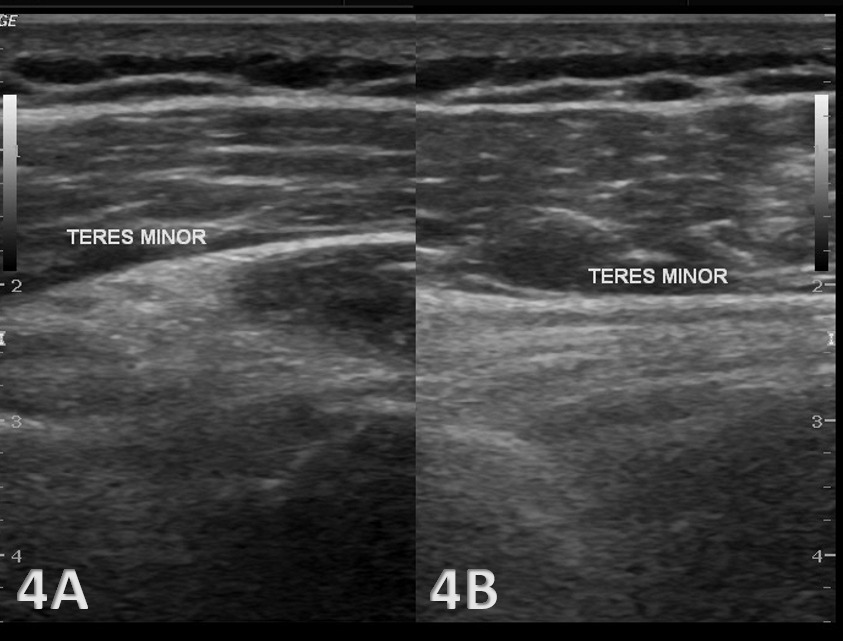
The starting point for examining the posterior rotator cuff tendons, including the teres minor, is to find the posterior greater tuberosity and humeral head. The greater tuberosity and humeral head will be easily seen by their hyperechoic cortical outline, with a large acoustic shadow beneath. The proximal portion of the teres minor tendon can be scanned in both the long axis (LAX) and the short axis (SAX). In the LAX view, depending on the probe width and size, one should start proximally to visualize the hyperechoic reflection of the bony cortex of the greater tuberosity. When viewed in LAX, the tendon will appear as a smaller tendon superficial to the larger proximal tendon of the infraspinatus. In the SAX, the ultrasound transducer can be rotated 90 degrees just below the scapular spine. Visualized from superior to inferior, the first tendon seen is the infraspinatus, while the deeper tendon will be that of the teres minor. As with many tendon locations, both views may require some toggling or heel-to-toe movements to reduce anisotropy.
Pathologic Findings in Teres Minor Tendon and Muscle Injury
-
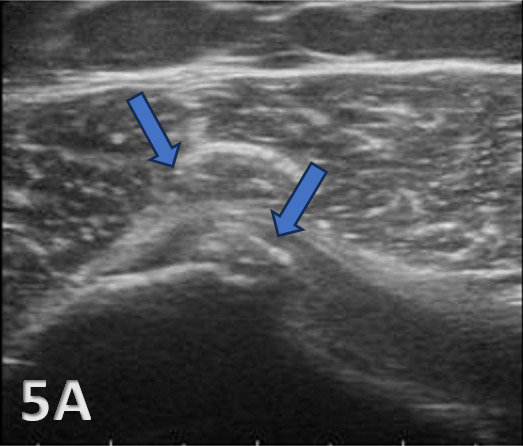
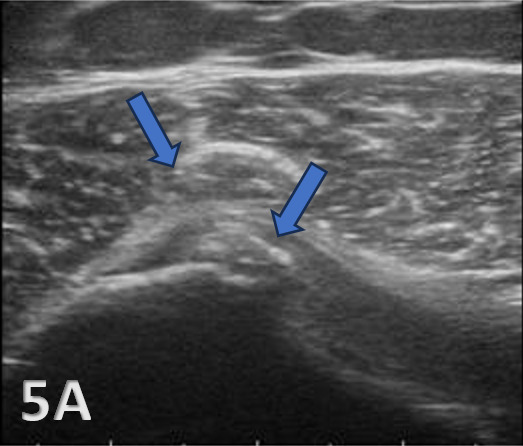
Isolated teres minor tears are rare.6–10 Disruption of fibrillar pattern is seen in partial tears and ruptures. Proximally, it is important to determine whether the injury is a free-tendon injury or a purely myotendinous injury. When there is a tear present, it will appear as either an anechoic or hypoechoic defect that disrupts the continuity of the insertion11 onto the greater tuberosity.
-
Atrophy of the tendon can be measured using volume estimations embedded into the ultrasound calculations. Atrophic changes are seen in up to 5% of patients presenting for routine shoulder imaging.12 Quadrilateral space syndrome is caused by compression of the humeral artery and axillary nerve within the quadrilateral space.13,14 The teres minor can contribute to this problem as it is the superior border of the space, while the teres major is inferior, the humerus laterally, and the long head of the triceps medially.15
-
Calcifications or retraction of the tendon may be visualized near the enthesis sites.
Clinical Implications for Rehabilitation Providers
MSKUS provides real-time feedback for rehabilitation professionals, facilitating early diagnosis and intervention. Key applications include:
-
Early Detection of Injury / Accurate Injury Grading: MSKUS can quickly differentiate between a tendinopathy versus a strain, or more severe tendon rupture or muscle tear, to help guide treatment planning.
-
Dynamic Functional Testing: Rehabilitation professionals can use MSKUS during physical therapy sessions to monitor recovery and assess tendon and muscle function dynamically. Serial MSKUS imaging aids in assessing muscle healing and remodeling, helping determine readiness for rehabilitation progression.
-
Guided Interventions: Ultrasound imaging assists in precision-guided dry needling or injections, such as corticosteroids for inflammation.
-
Patient Education: Real-time imaging serves as a visual aid to explain the nature of the injury and set realistic expectations for recovery.
Limitations and Challenges
Despite its advantages, MSKUS cannot entirely replace MRI for complex cases of rotator cuff and teres minor injury imaging. Additionally, the expertise required for optimal imaging techniques limits its immediate adoption across all rehabilitation settings.
Conclusion
In summary, diagnostic MSKUS offers rehabilitation professionals a powerful, clinically relevant extension of the physical examination when evaluating the teres minor. Its ability to provide high-resolution, real-time, and dynamic visualization of the teres minor tendon and muscle architecture enhances diagnostic precision, supports early clinical decision-making, and allows serial monitoring of tissue healing and load tolerance. When integrated with a thorough understanding of teres minor anatomy, injury mechanisms, and functional biomechanics, MSKUS becomes more than an imaging modality—it becomes a performance-informed clinical tool. While operator skill and certain anatomic limitations must be acknowledged, the thoughtful incorporation of MSKUS into sports and orthopedic practice has the potential to elevate assessment accuracy, refine rehabilitation progression, and ultimately improve return-to-play outcomes for athletes with rotator cuff injury, particularly involving the teres minor muscle and tendon.

.png)
.png)