

INTRODUCTION
Over the past 20-plus years, baseball has seen a proliferation of injuries to the ulnar collateral ligament (UCL) and subsequent reconstructive surgical procedures.1–5 More recently, there has been a growing interest in the role of the dynamic stabilizers of the medial elbow for protecting the UCL, in particular the roles of the flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS). Anatomically, the FCU and FDS tendons have insertions on the ulnar attachment of the anterior bundle of the UCL and can provide dynamic stability to the medial elbow.6,7 In cadaveric models, loading the FDS and FCU provided restraint to valgus stress, with lesser contributions from the pronator teres (PT).8,9 In human studies, maximal grip contractions decreased medial elbow joint gapping during valgus stress,10 and fatigue of the wrist flexors increased medial elbow joint gapping during valgus stress.11 More recently, repetitive baseball pitching was shown to increase medial elbow joint gapping,12 and the FCU was shown to be the primary dynamic restraint to medial elbow joint gapping with repeated baseball pitching.13 Based on these findings, there has been increased interest in training the dynamic stabilizers of the medial elbow in baseball pitchers.
There is limited research on exercises to activate the dynamic stabilizers of the medial elbow. Forearm pronation with elastic resistance activates the FDS and PT more than the FCU, while ulnar deviation with elastic resistance activates the FCU more than the FDS and PT.14 In contrast, middle and ring finger flexion activate the FCU and FDS more than the PT.15 Furthermore, middle and ring finger flexion strength was decreased after a pitching performance in baseball pitchers with high valgus torque on the elbow during pitches, but not in pitchers with low elbow torque.16 This finding indicates that the dynamic stabilizers of the medial elbow have to work harder in pitchers with higher torque at the elbow. Furthermore, middle finger flexion fatigue progresses rapidly during a pitching performance with 21% strength loss after only four innings compared to only 7% for ring finger flexion strength and 5% for grip strength.16 Importantly, middle finger flexion strength loss after four innings was much greater in pitchers with high valgus elbow torque versus pitchers with low torque,16 confirming the earlier finding.15 Based on these fatigue findings there has been increased interest in finger flexion strength training for baseball pitchers. Pitchers have started using finger flexor dynamometers as a part of their routine training. However, there is a lack of research examining how effective this dynamometer is at activating the dynamic stabilizers of the medial elbow, and in general there is limited research on the effectiveness of finger flexion exercises at activating the FCU and FDS. Therefore, the purpose of this study was to compare FCU, FDS, and PT electromyographic activation during finger flexor exercises using a finger flexor dynamometer versus rubber bands.
It was hypothesized that middle and ring finger flexion would activate the FCU and FDS more than the PT, and that there would be no difference in activation between the rubber band exercise and the finger flexor dynamometer.
MATERIALS AND METHODS
Participants
Nine healthy adults (8 men, 1 woman) volunteered to participate. All participants gave informed consent, and the study was approved by institutional review board (IRB #: 24-0973).
Procedures
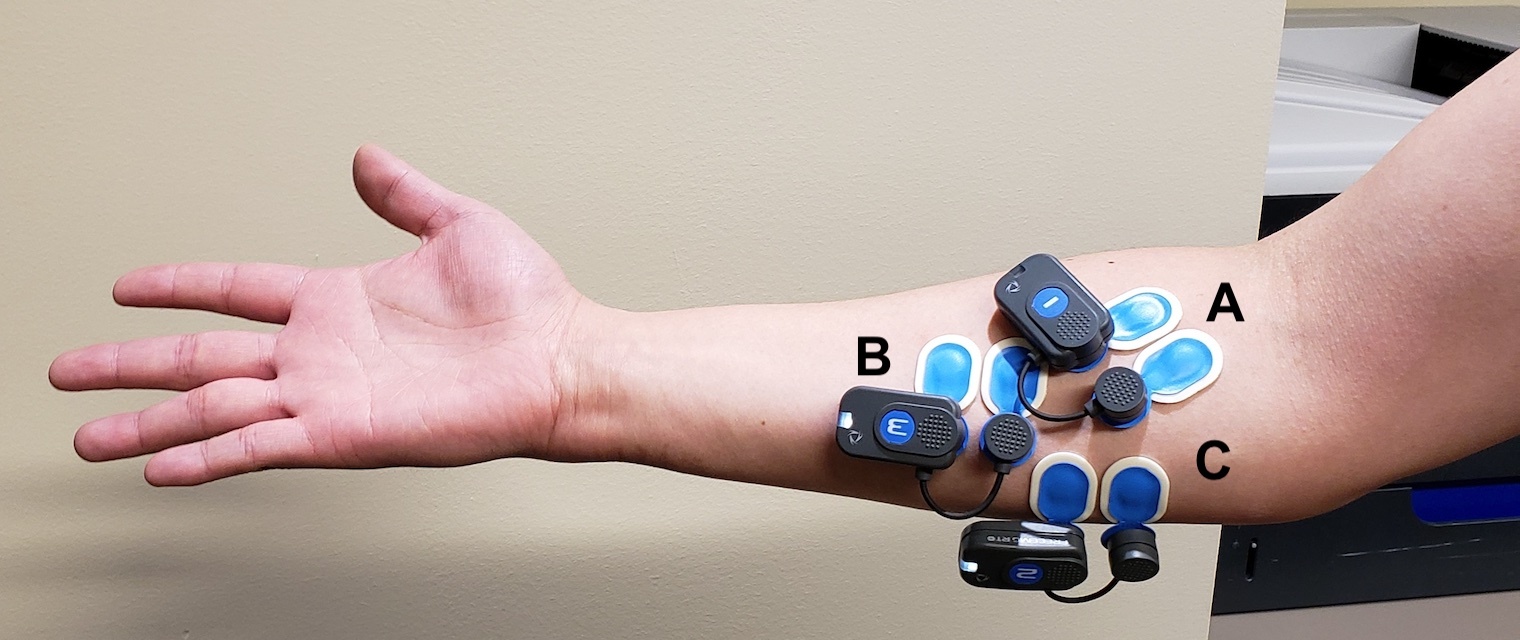
Electromyography (EMG) was used to record activation of the FCU, FDS and PT during finger flexion exercises using a 16-channel BTS FREEEMG 300 system, CMRR: >110 dB at 50–60 Hz; input impedance: >10 GΩ (BTS Bioengineering, Milan, Italy). After the skin of each participant was shaved, cleaned, and lightly abraded, disposable silver/silver chloride dual electrodes (2.0-cm interelectrode distance) (Ambu, Inc., Columbia, MD) were applied. Electrodes were placed as shown in Figure 1. The same investigator placed the electrodes for all subjects that were tested.
_pronator_teres_(pt)__(b)_flexor_digitorum_superficialis_(fds).jpg)
Prior to performing the finger flexor exercises, maximum voluntary contraction (MVC) testing was performed for each muscle: maximal resisted wrist flexion and ulnar deviation for the FCU performed in forearm supination; maximal resisted four-finger flexion with opposition applied across the middle phalanges for the FDS, performed in neutral forearm rotation; and maximal resisted forearm pronation with slight elbow flexion for the PT, performed in pronation. MVC testing was performed on both the dominant and nondominant arms. Each of the three MVC tests was performed twice, with each contraction lasting 3 seconds and the average EMG amplitude computed for each muscle. A single tester, a physical therapist with over 20 years of clinical experience, performed the MVC testing on all subjects. The EMG and MVC testing procedures have been used previously for studying the flexor pronator mass.14,15
The finger flexor dynamometer (Figure 2) has three different finger flexion test positions (long, intermediate, short). In this study isometric contractions were performed in the both the long and short positions to assess which muscle length maximally activated the target muscles. Testing in the long position was performed first, with three 3 second contractions performed by the forefinger, then middle finger, then ring finger, and lastly the little finger. Then the testing was repeated in the short position. In order to eliminate accessory arm movements, all subjects were seated for testing, and the testing was performed with the forearm supinated and resting on the subject’s thigh and the elbow flexed to 90° (Figure 2).

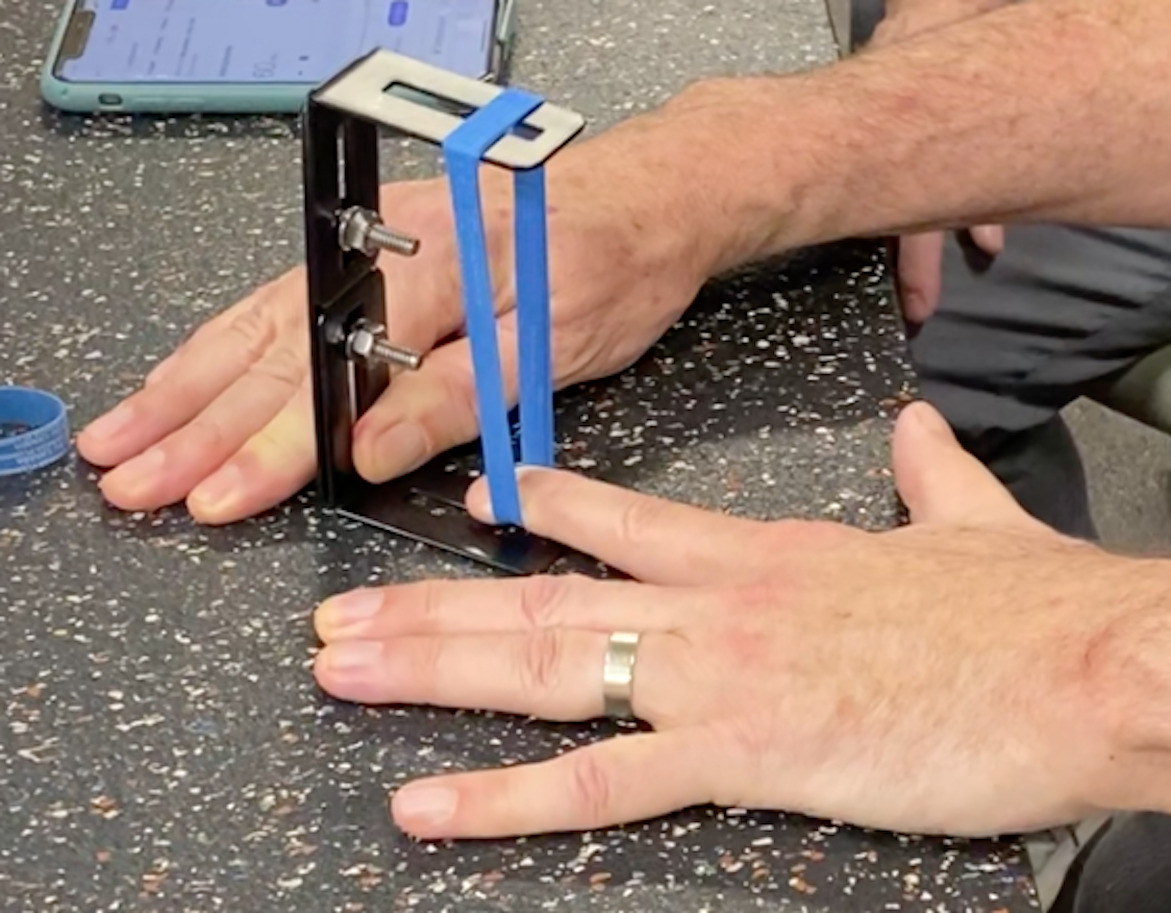
The elastic resistance finger flexor exercise device was fabricated by the authors for this study. The device consisted of an adjustable metal mounting bracket (ROADPRO, Elizabethtown PA) and two grocery store rubber bands (typically used to hold broccoli stalks together). The rubber bands were placed over the adjustable mounting bracket (Figure 3).
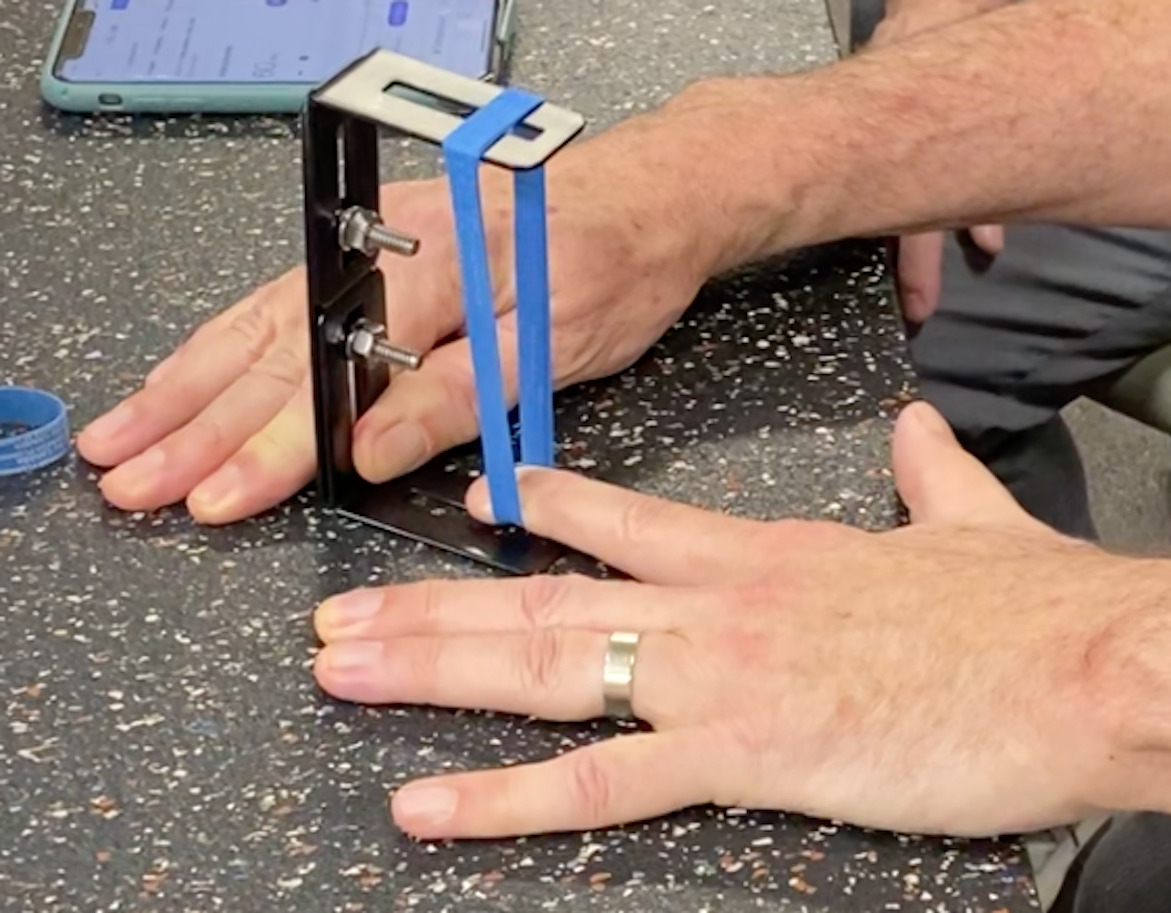
To control for the amount of elastic stretch during finger flexion, the mounting bracket was set such that the two rubber bands were stretched from a resting length of 1 inch to a maximum length of 5 inches (400% elongation). The subject placed the palm of the hand on the table and extended the test finger to reach the rubber bands. From a starting position at 1 inch the subject stretched the rubber band to a length of 5 inches, corresponding with the fingertip reaching the table (Figure 3). The rubber band was placed at the distal interphalangeal joint. A metronome was used to control the rate of flexion such that the subject took 3 s to stretch the rubber band to the table, then maintained this isometric point for 3 s, and then released back to the starting position in 3 seconds. Three repetitions were performed with each finger (forefinger, middle finger, ring finger) always starting with the forefinger. Little finger flexion was not tested with the rubber band because the elastic resistance exceeded the flexion strength of most subjects. The EMG activity for the 3 second isometric phase of the rubber band finger flexion was used for comparison to the isometric contractions performed on finger flexor dynamometer.
For both the finger flexor dynamometer and rubber band flexions, the dominant and nondominant hands were tested, with starting side alternated between subjects.
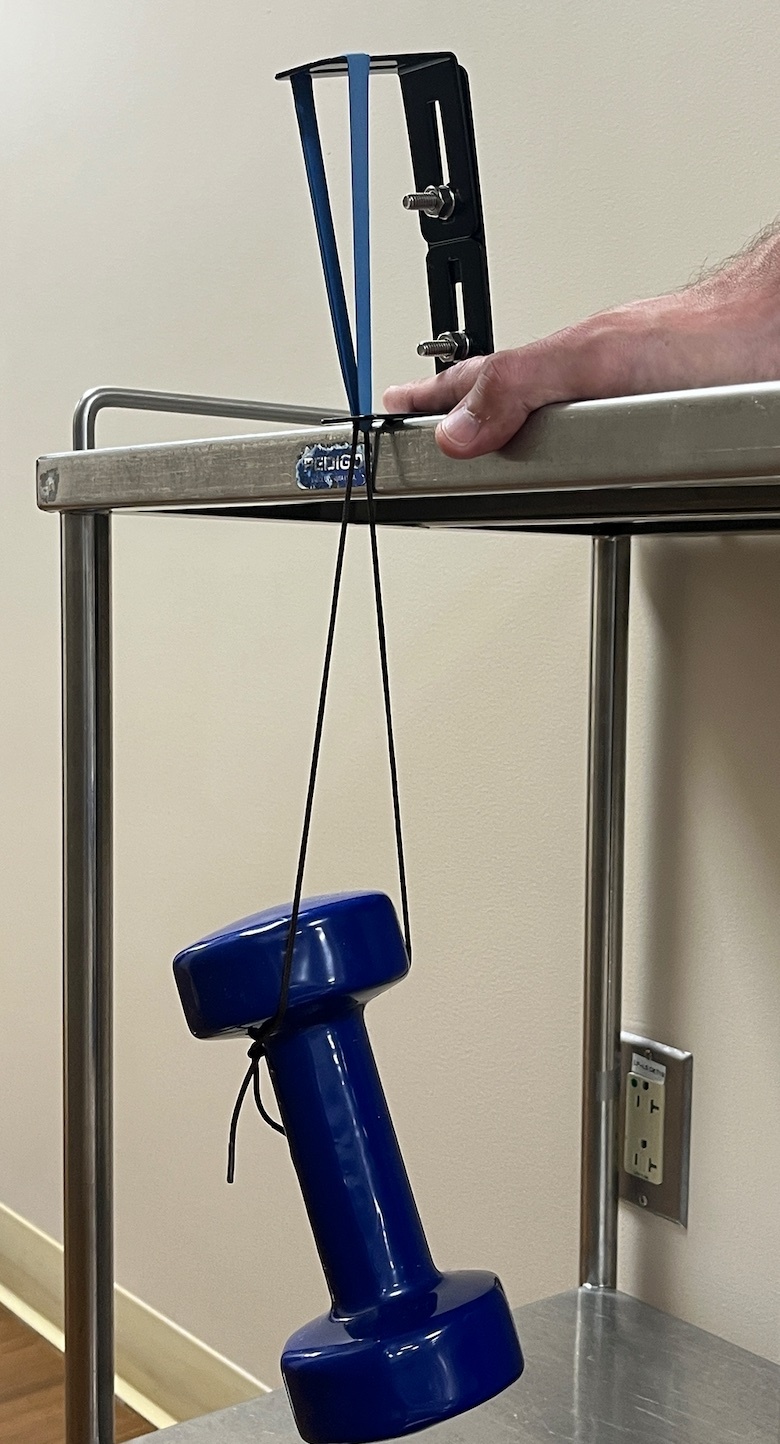
Since the elastic resistance exercise involved the same resistance for each finger (2 rubber bands stretched 5 inches), the force required to elongate the rubber bands to 5 inches was measured by hanging progressively more weight from the bands until they were stretched by 5 inches while they were attached to the mounting bracket (Figure 4). This was repeated three times to insure consistency. Then the finger flexion strength was recorded for the forefinger, middle finger and ring finger using a handheld dynamometer as previously described.15,16 The force required to stretch the rubber bands by 5 inches was expressed as a percentage of the subject’s finger flexion strength (100% of the dynamometer reading) to derive a contraction intensity for the rubber band flexions for each finger.
Data Processing
Raw EMG signals were high-pass filtered at 10 Hz, full-wave rectified, and smoothed using an RMS filter with a 100-ms window. For each 3-s contraction, the peak RMS value from 250 ms after the start of the isometric contraction to 250 ms before the end of the contraction, was identified. Then a 500 ms average amplitude was computed for the period 250 ms either side of the peak value. This insured that the sampled EMG activity was entirely within the isometric phase of the exercise. EMG amplitudes for the finger flexor dynamometer and rubber band exercises were expressed as a percentage of MVC.
Statistical Analyses
Repeated-measures analysis of variance was used to assess differences in activations between devices (finger flexor dynamometer vs. elastic resistance) and muscles (FCU, FDS, PT). Bonferroni corrections were applied to planned pairwise comparisons such that the adjusted p- value for significance was p<0.017 (finger flexor dynamometer vs. elastic resistance for each of 3 muscles or FCU vs. FDS, FCU vs. PT, FDS vs. PT for either device). For the finger flexor dynamometer, effect of starting position (short vs. long) and hand dominance were also assessed using repeated-measures analysis of variance. Based on the variability in EMG amplitudes for the three muscles for middle finger flexion versus ring finger flexion from a prior study15 it was estimated that with nine subjects there would be 80% power to detect a 28% MVC difference between finger flexion with the dynamometer versus rubber band at p<0.05. Since little finger flexion was only tested on the finger flexor dynamometer, and not with the rubber bands, it was not included in the comparisons between devices. These data are reported separately at the end of the results section.
RESULTS
The study participants (8 men, 1 woman) were age 39±16 yr, height 1.79±0.09 m, mass 82.2±15.0 kg. For the finger flexor dynamometer, EMG amplitudes were not significantly different between the long and short positions (p=0.766); therefore, the long position was used for comparison to rubber band finger flexion as it replicated finger length for the rubber band finger flexions. EMG amplitudes were not significantly different between the dominant and nondominant hands (p=0.353); therefore, subsequent analyses were collapsed across sides. EMG amplitudes varied between devices, fingers, and muscles (device by finger by muscle p<0.001), therefore, the results are reported as follows: (1) the effect of device (finger flexor dynamometer vs. rubber band) for each muscle and each finger; (2) the effect of muscle (FCU vs. FDS vs. PT) for each device and each finger; (3) the effect of finger (forefinger vs. middle finger vs. ring finger) for each device and each muscle. The reported p-values for each pairwise comparison have been multiplied by 3 such that an uncorrected threshold for significance of p<0.05 is actually p<0.017.
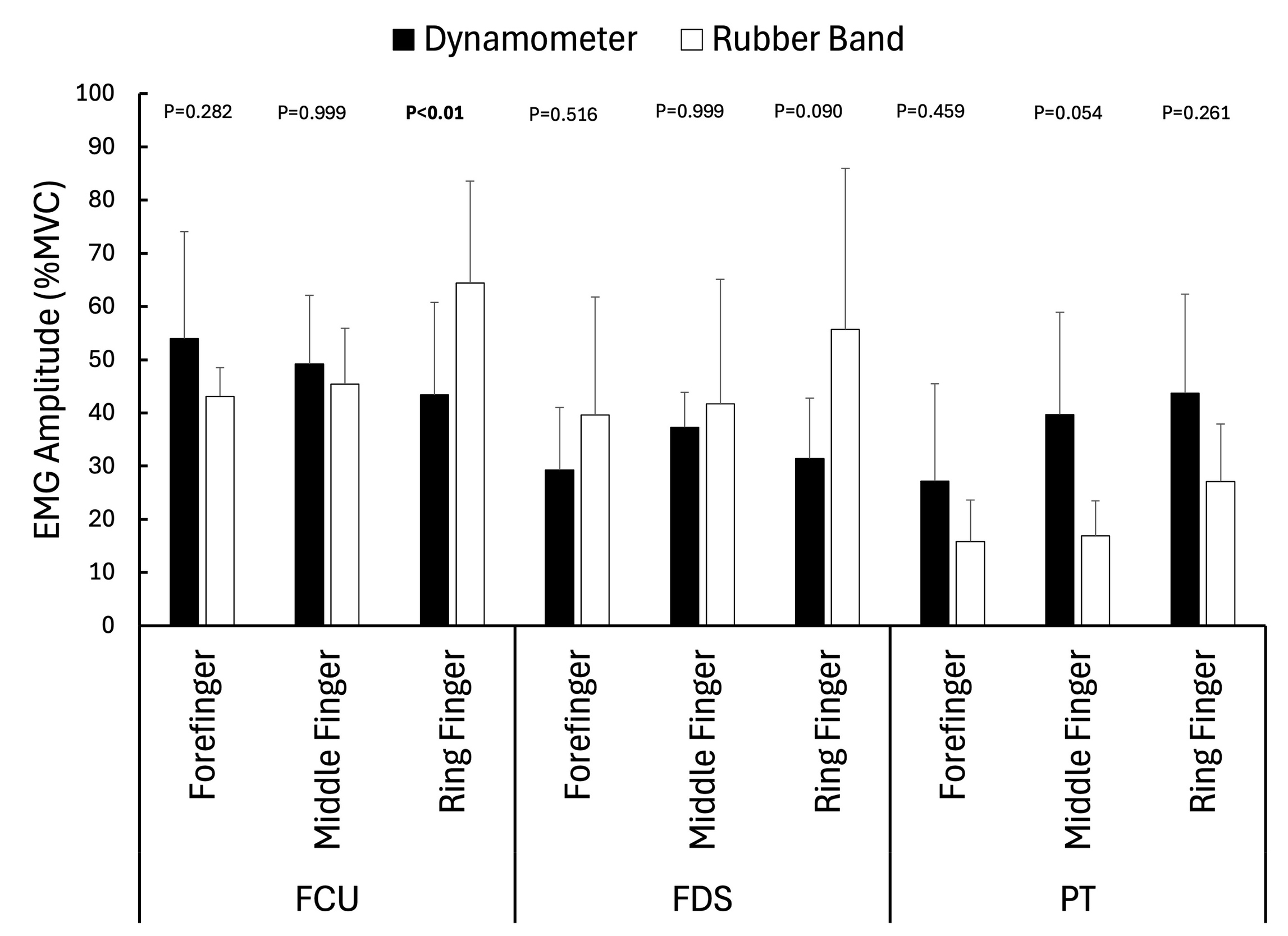
Effect of Device (Comparison of EMG amplitudes between finger flexor dynamometer and rubber bands)
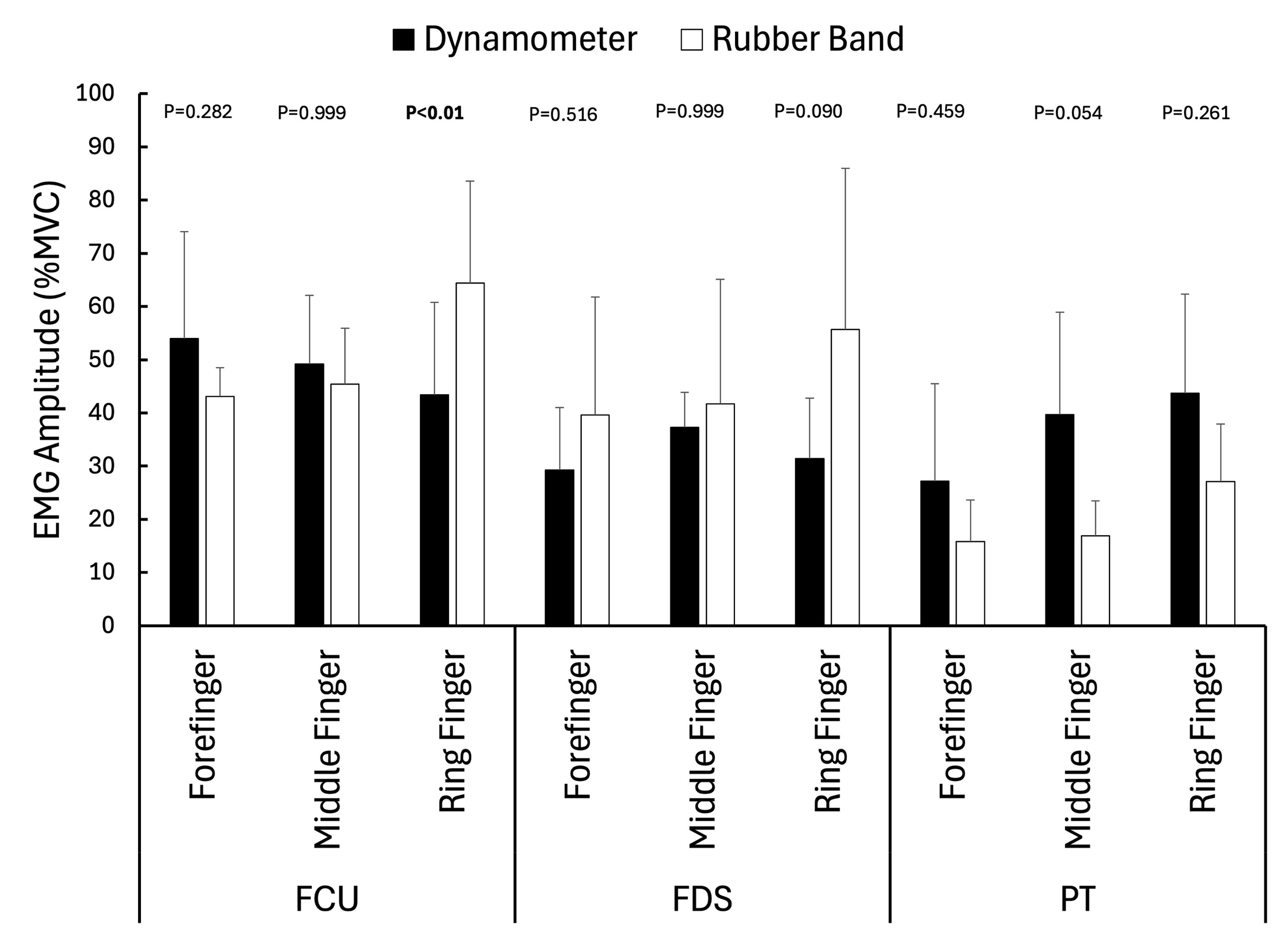
FCU activity during ring finger flexion was significantly higher (p=0.002) for the rubber band (64±19% MVC) compared with the finger flexor dynamometer (43±17% MVC). EMG amplitudes during finger flexion were not significantly different between devices for any other muscle or finger. (Figure 5)
Effect of Muscle (Comparison of EMG amplitudes between the FCU, FDS and PT)
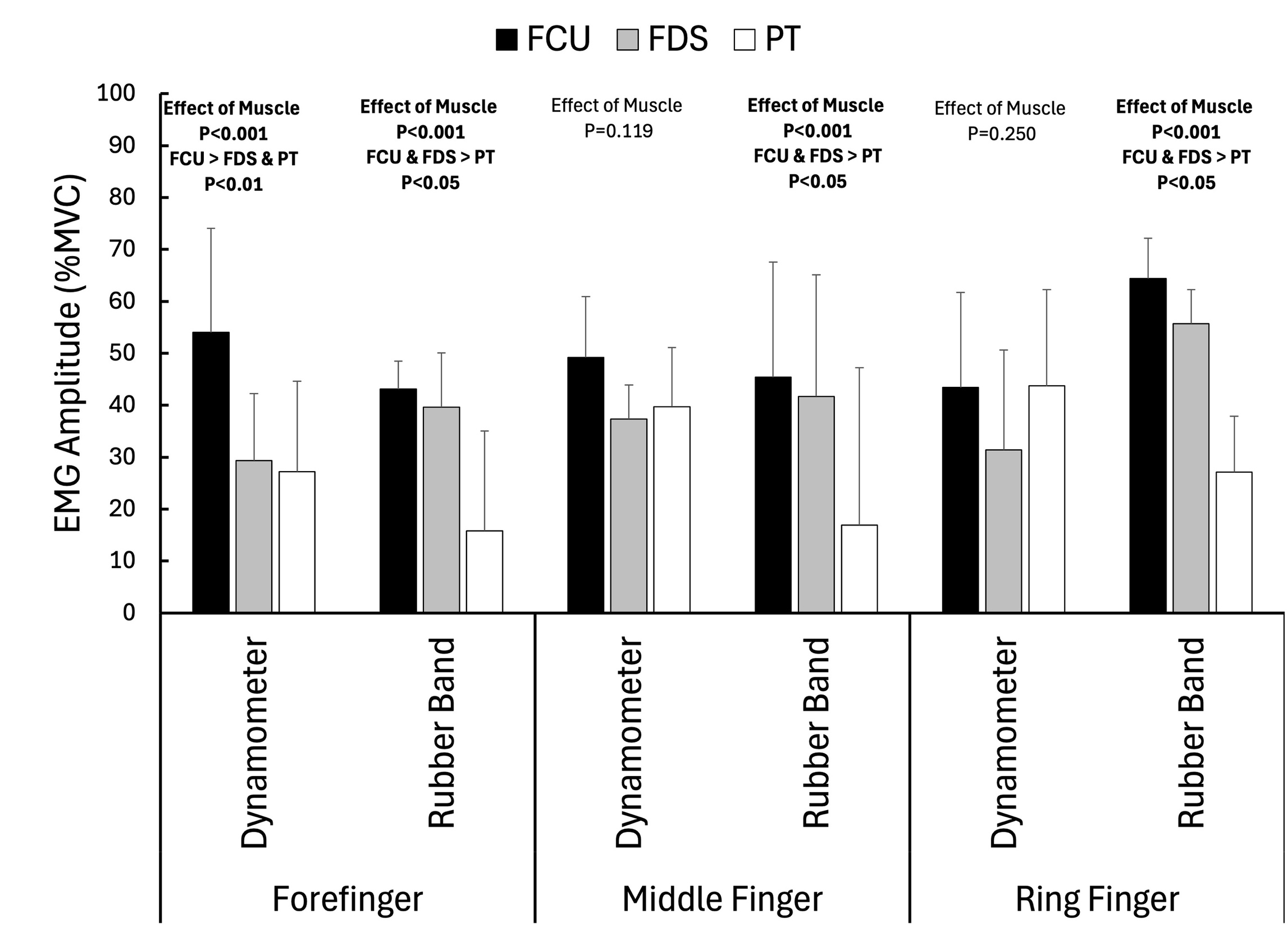
During forefinger flexion on the dynamometer, FCU activity (54±20% MVC) was significantly higher than FDS (29±12% MVC, p=0.002) and PT (27±18% MVC, p=0.006). There was no significant difference in activation between the muscles for middle (p=0.119) and ring finger flexion (p=0.250) on the finger flexor dynamometer. During finger flexion with the rubber bands, FCU and FDS activity was significantly higher than PT activity (Figure 6) for forefinger flexion (FCU 43±5% MVC, FDS 40±22% MVC, PT 16±8% MVC), middle finger flexion (FCU 45±11% MVC, FDS 42±23% MVC, PT 17±7% MVC), and ring finger flexion (FCU 64±19% MVC; FDS 56±30% MVC, PT 27±11% MVC).
__flexor_digitorum_su.jpeg)
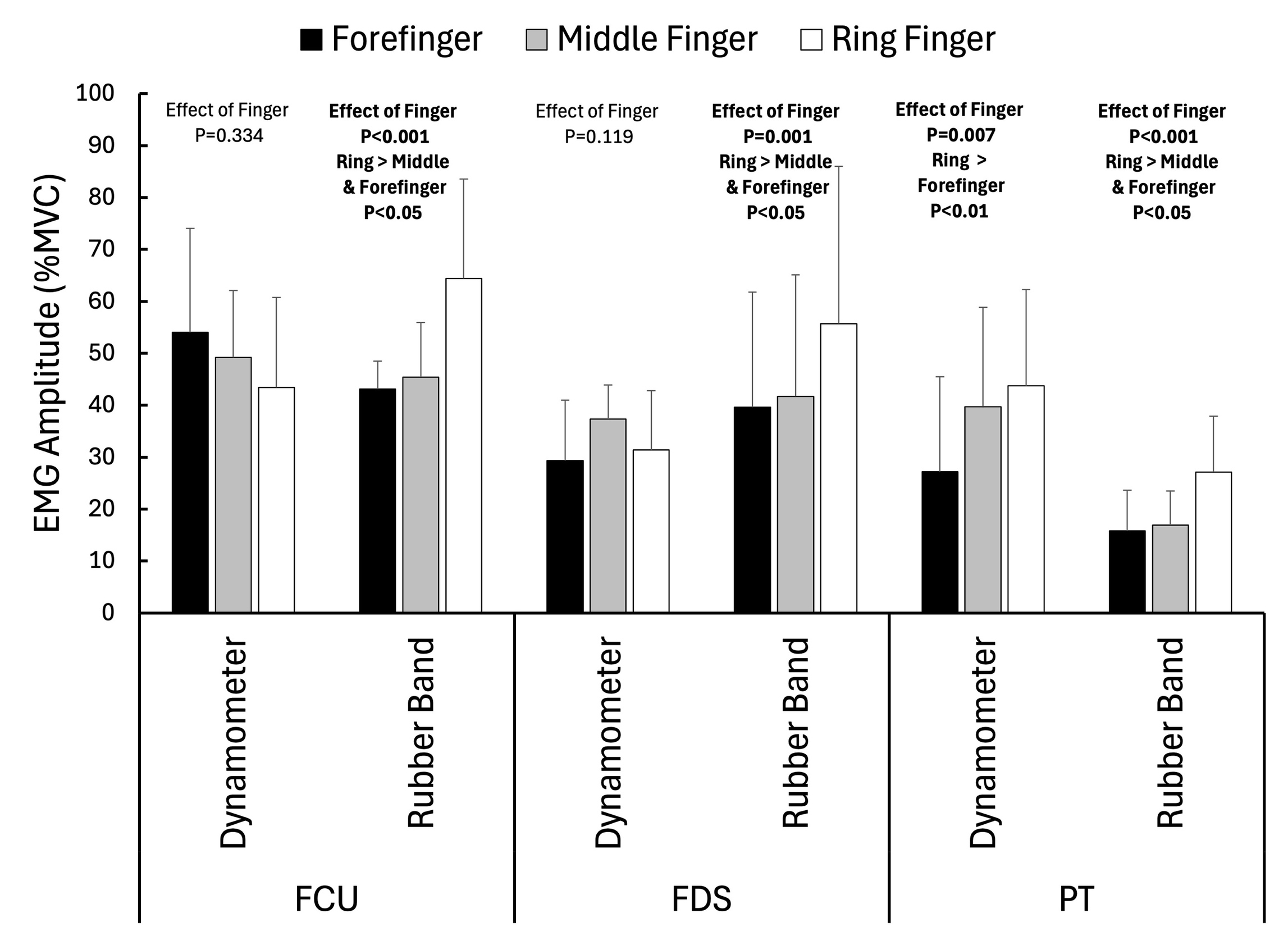
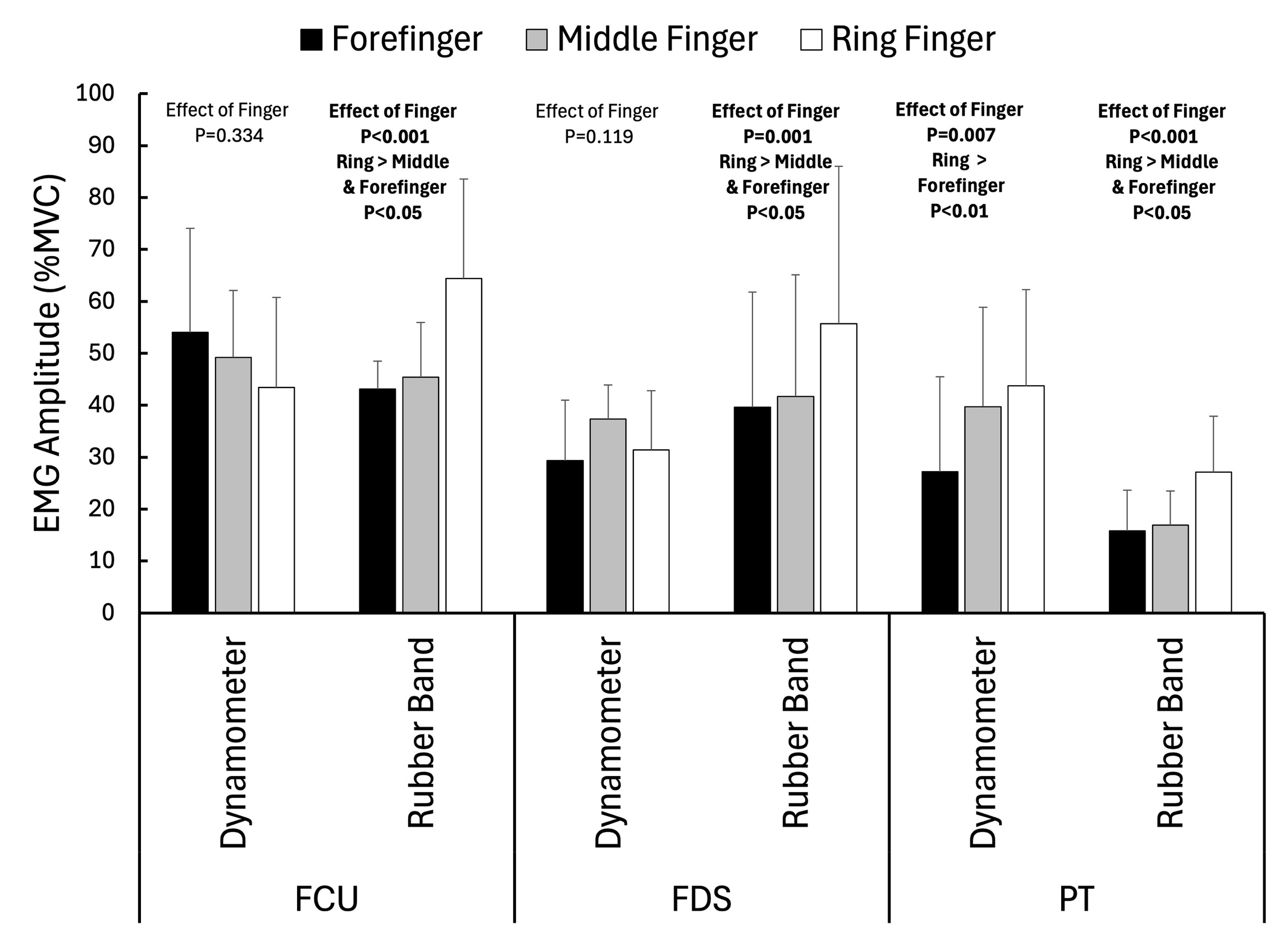
Effect of Finger (Comparison of EMG amplitudes between forefinger, middle finger and ring finger flexion)
On the finger flexor dynamometer, PT EMG amplitude was significantly higher during ring finger flexion compared with forefinger flexion (44±19% MVC vs. 27±18% MVC, p=0.028), but FCU and FDS amplitudes were not significantly different between fingers during flexion on the finger flexor dynamometer. For finger flexion with the rubber bands, FCU, FDS, and PT amplitudes were significantly higher during ring finger flexion (64±19% MVC, 56±30% MVC, 27±11% MVC) compared with forefinger (43±5% MVC, p=0.023; 40±22% MVC, p=0.028; 16±8% MVC, p=0.041) and middle finger flexion (45±11% MVC, p=0.006; 42±23% MVC, p=0.012; 17±7% MVC, p=0.004).
Intensity of Elastic Resistance Finger Flexion
Ring finger flexion strength (48.2±6.3 N) measured with the handheld dynamometer was significantly lower (p<0.001) than middle finger (61.5±4.8 N) and forefinger flexion strength (70.7±9.5 N). Forefinger strength was not significantly different from middle finger strength p=0.084). There was no significant difference in finger flexion strength between the dominant and nondominant hands (p=0.245). The force required to stretch the two rubber bands to 5 inches was 40.1 N (9lb), which was 57.9±7.8% of forefinger strength, 66.1±5.1% of middle finger strength, 97.1±16.5% of ring finger strength, and 114.5% of little finger strength.
Little Finger Flexion (Tested only on the finger flexor dynamometer)
During little finger flexion on the dynamometer, PT activation (44±20% MVC) was significantly higher (p=0.033) than FCU activation (26±10% MVC). FDS activation (32±13% MVC) was not significantly different from PT (p=0.450) or FCU activation (p=0.378).
DISCUSSION
With respect to providing dynamic stability to the medial elbow with finger flexor exercises, the goal was to identify exercises that activate the FCU and FDS. In this regard, ring finger flexion with rubber bands activated the FCU more than ring finger flexion with the finger flexor dynamometer. Of note, the relative force during the ring finger rubber band exercise was comparable to the finger flexor dynamometer exercise (97.1% and 100% of maximum, respectively). Activations for other muscles, and other fingers, were not significantly different between the finger flexor dynamometer and the rubber bands despite the fact that forefinger and middle finger flexion with the rubber bands constituted a force of only 57.9% and 66.1% of MVC, respectively, compared with maximal effort on the finger flexor dynamometer.
The rubber band exercise was also more selective for the FCU and FDS versus the PT. For the rubber band finger flexion activation of the FCU and FDS were higher than PT for all three fingers. By contrast, for the finger flexor dynamometer there were no significant differences between the three muscles for middle and ring finger flexion contractions. For forefinger flexion, FCU activation was significantly greater than FDS and PT. The current results with the rubber band confirm previous work15 showing that middle and ring finger flexion selectively activate the FCU and FDS relative to the PT during strength testing on a handheld dynamometer.
During the finger flexions with the rubber band, EMG amplitudes were higher for ring finger flexion versus middle and forefinger flexion. This is primarily due to the fact that the ring finger was weaker than the middle and forefinger during flexion, and therefore, the ring finger was working at a higher intensity to stretch the rubber bands. EMG amplitudes were generally not different between fingers during finger flexion on the finger flexor dynamometer, as intensity was maximal for each finger. The exception was higher PT activity on the dynamometer during ring finger flexion versus forefinger flexion.
Despite a relatively small sample size, differences in EMG activity were demonstrated between devices and muscles. The muscle effects are noteworthy considering the proximity of the electrode placements and the risk of crosstalk between electrode pairs obscuring the signal from the target muscles. The practical and clinical significance of these results pertain to training the muscles that provide dynamic stability to the medial elbow. This is an important issue for baseball pitchers, but it is important to note that the subjects in this study were not baseball pitchers. It cannot be assumed that the activation patterns for the FCU, FDS and PT during finger flexion are similar between baseball pitchers and non-baseball players, and this should be examined in future work.
Future work should also examine finger flexion strength in baseball pitchers. Importantly, for comparison between players it is important to measure the lever arm (finger length) so that finger flexion torque can be computed. Considering that middle finger flexion fatigues progressively over just four innings,16 and that fatigue is greater in pitchers with high medial elbow torque,15,16 there may be an advantage for pitchers with longer fingers. Pitchers with longer fingers may need to produce less force to achieve the same torque compared with pitchers with shorter fingers. This may delay fatigue. Professional pitchers with prior ulnar collateral ligament reconstructions had smaller hands than uninjured pitchers.17 It was theorized that a smaller hand could result in the FDS working harder to hold the ball potentially leading to earlier fatigue.
The finger flexor dynamometer used in the present study provides a force output, but unfortunately it is reported in arbitrary units. It was not possible to reliably calibrate the device to convert the values to Newtons or to compute torques. Therefore, the finger flexor dynamometer force values were not reported here. This finger flexor dynamometer is primarily used for training, and is typically used with all four fingers flexing simultaneously. The activations of the FCU, FDS and PT may be higher when all fingers are flexed at the same time versus individually. However, in the present study, simultaneous contraction of all fingers was not studied because it would mask which finger selectively contributed to activating which muscle. The rubber band exercise described here could easily be adapted to exercise all four fingers at once and future work could compare this to the finger flexor dynamometer used with all four fingers at once. However, based on the current evidence,15,16 exercising the middle and ring finger flexors may be most appropriate for training the FCU and FDS to address fatigue resistance.
Testing with the finger flexor dynamometer was performed with the forearm supinated, while testing with the rubber bands was performed with the forearm pronated. These test positions were chosen as they provided the best way to control for accessory motion during the testing for each device. However, this difference affects the length-tension relationship; thus, it may have affected the differences in activations between the two devices. It would be logical to have expected greater PT activity in the pronated rubber band test position compared to the supinated finger flexor dynamometer test position. However, there was no statistically significant difference in PT activity between devices with a trend for greater PT activity during middle finger flexion with the finger flexor dynamometer versus the rubber bands. Surprisingly, testing with the forearm pronated (rubber band) was selective for the FCU and FDS over the PT while testing with the forearm supinated was not selective for the FCU and FDS. Active insufficiency of the PT in the fully pronated test position may have reduced activation. An additional difference between the exercises was that the contractions with the finger flexor dynamometer were all isometric, while the rubber band finger flexions involved a concentric phase, followed by an isometric phase, and finally an eccentric phase. However, only the isometric phase was used for comparisons to the finger flexor dynamometer, but the prior concentric phase might have affected muscle activations.
Previous work has focused on middle and ring finger flexion in baseball pitchers,15,16 but has not examined forefinger or little finger flexion. In the present study muscle activations were also examined during forefinger flexion (finger flexor dynamometer and rubber bands) and little finger flexion (finger flexor dynamometer only). During little finger flexion on the dynamometer FCU and FDS activations were low (26% and 31% MVC, respectively) and therefore, little finger flexion strength likely does not play a significant role in dynamic stability of the medial elbow. However, during forefinger flexion FCU activation was relatively high on both the dynamometer (54% MVC) and the rubber bands (43% MVC). Previously, forefinger, middle finger and ring finger flexion contractions against fixed resistance were each effective at reducing medial elbow joint gapping during valgus stress.18 The effects were greater for forefinger and middle finger contraction compared with ring finger.18 Future work should examine whether forefinger fatigue is comparable to middle finger fatigue with pitching, and if forefinger fatigue is affected by the magnitude of the valgus torque on the elbow during pitching.
CONCLUSION
The results of this study indicate that the dynamic stabilizers of the medial elbow, specifically the FCU and FDS, are highly active during middle and ring finger flexion performed on a finger flexor dynamometer or performed with rubber bands. Middle and ring finger flexion with the rubber bands selectively activated the FCU and FDS over the PT, however, FCU, FDS, and PT activations did not differ during middle and ring finger flexion with the dynamometer. Furthermore, FCU activation was significantly higher during ring finger flexion with the rubber bands compared to the dynamometer. Overall, these findings support the use of finger flexion exercises to train the dynamic stabilizers of the medial elbow. Isometric finger flexion exercises with rubber bands provide an inexpensive, practical means of activating the dynamic stabilizers of the medial elbow.
Corresponding Author:
Malachy P. McHugh
NISMAT
MEETH
210 East 64 Street, 5th floor
New York, NY 10065
PH: 212 434 2700
Fax: 212 434 2687
Email: mchugh@nismat.org
Conflicts of Interest
The authors report no conflicts of interest